Rashes and skin ulcers in diabetes
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"diabetic skin" AND "ulcer" AND "rash"
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive, well-illustrated content from Fitzpatrick's, Rosen's, Andrews', and Dermatology 5e. Here is the full answer:
Rashes and Skin Ulcers in Diabetes Mellitus
Nearly all patients with diabetes develop at least some cutaneous manifestations during their lifetime. These fall into four broad mechanistic categories: (1) metabolic/insulin-related, (2) vascular/neuropathic, (3) immunologic (infections), and (4) conditions of unknown pathogenesis. - Fitzpatrick's Dermatology, Ch. 137
Pathogenesis Overview
- Advanced glycation end-products (AGEs): Hyperglycemia accelerates nonenzymatic glycosylation of collagen and structural proteins, reducing acid solubility and enzymatic degradation of dermal collagen. Cutaneous AGE levels correlate with retinopathy, nephropathy, and other microvascular complications.
- Hyperinsulinemia / insulin resistance: Excess insulin acts on IGF-1 receptors on keratinocytes and fibroblasts, driving conditions like acanthosis nigricans.
- Immune dysfunction: Hyperglycemia and ketoacidosis impair chemotaxis, phagocytosis, and bactericidal activity of white blood cells, predisposing to aggressive infections.
- Neuropathy + vasculopathy: Peripheral sensory neuropathy and peripheral vascular disease (PVD) combine to produce foot ulcers and impair wound healing.
1. Conditions With a Known Metabolic Mechanism
Acanthosis Nigricans (AN)
- Appearance: Velvety, hyperpigmented, brown-black thickening of skin at flexural/intertriginous areas (axillae, neck, groin). Can also affect extensor surfaces.
- Mechanism: Hyperinsulinemia stimulates IGF-1 receptors on keratinocytes, causing proliferation.
- Associations: Strongly linked to insulin resistance (Type 2 DM), obesity, polycystic ovary syndrome. Also seen with certain malignancies (gastric carcinoma) and drugs (glucocorticoids, nicotinic acid, estrogens).
- Treatment: Difficult; weight loss and metformin (to improve insulin sensitivity) may help. Topical calcipotriol, retinoids, or keratolytics used with variable success. - Fitzpatrick's
Eruptive Xanthomas
- Appearance: Sudden crops of red-yellow papules on the buttocks, extensor surfaces, often with an erythematous base.
- Mechanism: Hypertriglyceridemia in poorly controlled diabetes causes triglyceride-laden macrophage foam cell deposits in the dermis.
- Treatment: Glycemic control and lipid-lowering therapy lead to regression. - Dermatology 5e; Rosen's
Diabetic Thick Skin / Limited Joint Mobility (LJM / Cheiroarthropathy)
- Appearance: Thickened, waxy, smooth skin on the hands and fingers with painless flexion contractures beginning at the 5th digit DIP joint and progressing radially. The classic "prayer sign" - inability to approximate the palmar surfaces fully.

- Prevalence: 30-50% of adults with Type 1 DM; also common in Type 2.
- Associations: Longer duration of diabetes, higher HbA1c (2.5-fold increased risk per unit HbA1c increase), and microvascular disease.
- Treatment: Tight glycemic control is the cornerstone of both prevention and management. - Fitzpatrick's
Scleredema Diabeticorum
- Diffuse, non-pitting induration of the posterior neck and upper back, distinct from scleroderma.
- Caused by dermal mucin and collagen accumulation from AGE formation.
2. Conditions of Unknown or Debated Pathogenesis
Diabetic Dermopathy ("Skin Spots")
- Most common cutaneous finding in diabetes.
- Appearance: Discrete, atrophic, brownish, slightly depressed macules/patches typically <15 mm on the shins (pretibial area).
- Mechanism: Possibly related to trauma with altered healing due to microangiopathy; not directly proportional to glycemic control.
- Clinical note: Often overlooked; presence correlates with other microvascular complications (retinopathy, nephropathy). No specific treatment needed. - Rosen's; Dermatology 5e
Necrobiosis Lipoidica (NL)
- Appearance: Begins as erythematous papules or nodules, typically on the pretibial region. Lesions expand and coalesce into a single area of atrophic, yellow-waxy skin with a red-brown border and overlying telangiectasias. The center frequently ulcerates.
- Association: ~0.3% of diabetics; however, up to 65% of NL patients have DM. Can precede the diagnosis of diabetes.
- Mechanism: Unknown - proposed theories include microangiopathy, immune complex deposition, and abnormal collagen metabolism.
- Treatment: Difficult. Options include potent topical or intralesional corticosteroids (at the active border), PUVA, cyclosporine, TNF-alpha inhibitors, and platelet-derived growth factor. Wound care for ulcerated lesions. - Andrews'; Fitzpatrick's
Granuloma Annulare (GA)
- Appearance: Erythematous annular papules/plaques, particularly the disseminated variant (hundreds of lesions over the trunk/extremities).
- Association with DM: The exact relationship is controversial - disseminated GA is more strongly linked to diabetes than the localized form.
- Mechanism: Unknown; thought to involve altered collagen/macrophage interaction.
Bullosis Diabeticorum (Diabetic Bullae)
- Appearance: Spontaneous, tense, non-inflammatory bullae filled with clear (occasionally hemorrhagic) fluid on the distal lower extremities, especially the feet and toes. No preceding trauma.

- Mechanism: Uncertain - microangiopathy may be a contributor.
- Outcome: Usually heal spontaneously within weeks without scarring. Treatment is conservative (sterile drainage if large; avoid rupture). - Rosen's; Dermatology 5e
Acquired Perforating Dermatosis
- Appearance: Pruritic keratotic papules, primarily on the legs.
- Association: Seen in diabetics, particularly those with concurrent renal failure (dialysis patients). Also occurs in prurigo nodularis context.
- Transepidermal elimination of altered dermal collagen is the proposed mechanism. - Fitzpatrick's
3. Infections (Immunologic Dysfunction)
Impaired WBC function in diabetes allows normally-contained organisms to become aggressive:
| Infection | Key Features |
|---|---|
| Candidiasis | Intertrigo in skin folds, angular cheilitis, onychomycosis, genital candidiasis |
| Dermatophytosis | Tinea pedis, onychomycosis - common, often precede foot ulcers |
| Malignant external otitis | Pseudomonas aeruginosa; aggressive, can spread to skull base |
| Necrotizing fasciitis | Rapidly spreading, life-threatening soft-tissue infection |
| Mucormycosis | Rare but devastating rhinoorbital/cerebral infection; often in DKA |
| Impetigo / Intertrigo | Resistant, recurring cases should raise suspicion for undiagnosed DM |
4. Diabetic Foot Ulcers (Skin Ulcers)
About 34% of people with diabetes develop a foot ulcer during their lifetime. Annual progression to osteomyelitis is ~5%. - Harrison's Principles of Internal Medicine, 22e

Pathogenesis
The three principal contributors are:
- Peripheral sensory neuropathy - loss of protective sensation allows unrecognized pressure injury. Diminished neuropeptide signaling impairs wound healing.
- Peripheral vascular disease - ischemia impairs tissue perfusion and healing.
- Pressure / foot deformity - Charcot arthropathy creates high-pressure points; callus precedes ulceration. Ill-fitting footwear was the most common identifiable cause in one study of 314 patients.
Risk factors: Prior foot ulcer, prior amputation, DM duration >10 years, poor glycemic control, impaired visual acuity, onychomycosis, monofilament insensitivity.
Types of Ulcers
| Type | Neuropathic | Neuroischemic/Ischemic |
|---|---|---|
| Location | Pressure points (metatarsal heads, plantar) | Margins, tips of toes, heels |
| Wound bed | Pink, granulating | Pale, necrotic, dry |
| Pulses | Present | Absent/diminished |
| Sensation | Absent | May be present |
| ABI | Normal | ≤0.8 |
Management - Step-by-Step
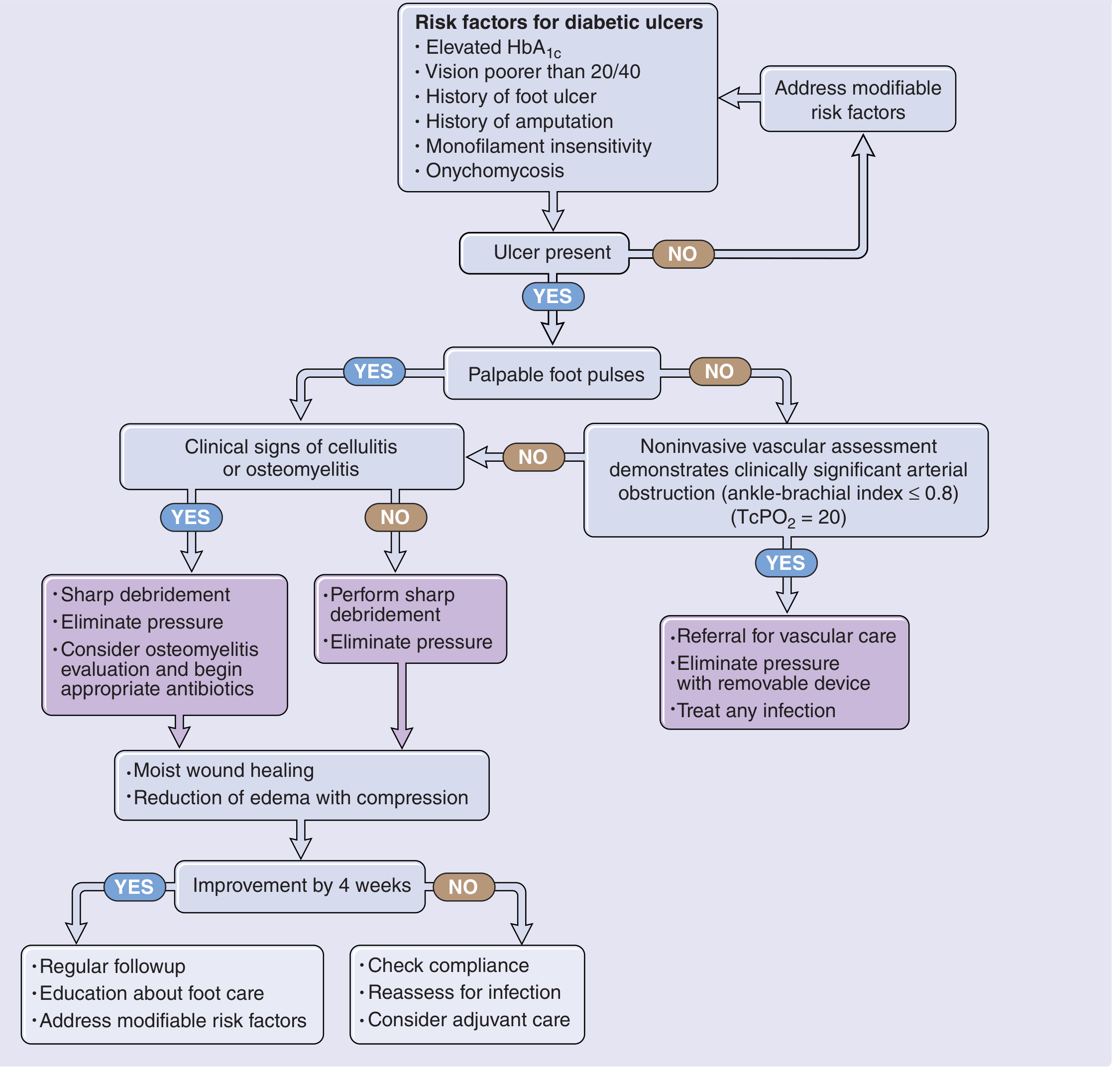
Standard care for neuropathic ulcers:
- Off-loading - total contact casting or removable cast walker is the gold standard. No weight-bearing.
- Sharp debridement of necrotic tissue and callus.
- Infection control - assess for cellulitis and osteomyelitis; appropriate antibiotics.
- Moist wound care - moisture-retentive dressings.
- Vascular assessment - if pulses absent or ABI ≤0.8, refer for vascular surgery evaluation.
- Glycemic optimization - tight control (HbA1c target <7%).
- Adjunctive therapies - recombinant PDGF (becaplermin) provides modest benefit when combined with off-loading and debridement. Bilayered living skin equivalents showed 56% healing at 12 weeks vs. 38% for standard care alone.
- If no improvement by 4 weeks: reassess for occult infection, compliance, and consider advanced wound biologics. - Fitzpatrick's; Harrison's
Complete Summary Table of Diabetic Skin Conditions
| Condition | Appearance | Mechanism | Key Association |
|---|---|---|---|
| Acanthosis nigricans | Velvety hyperpigmented flexural plaques | Hyperinsulinemia → IGF-1 | Insulin resistance, obesity |
| Eruptive xanthomas | Yellow-red papules, buttocks/extensors | Hypertriglyceridemia | Poor glycemic control |
| LJM / Cheiroarthropathy | Thickened skin, prayer sign | AGE collagen accumulation | Type 1 DM; retinopathy |
| Scleredema diabeticorum | Posterior neck/upper back induration | AGEs, mucin deposition | Obese Type 2 DM |
| Diabetic dermopathy | Brown atrophic shin spots | Trauma + microangiopathy | Most common finding |
| Necrobiosis lipoidica | Yellow atrophic plaque, red border, ulcerates | Unknown | 0.3% of diabetics |
| Granuloma annulare | Erythematous annular lesions | Unknown | Disseminated form more linked to DM |
| Bullosis diabeticorum | Spontaneous acral bullae | Microangiopathy (unclear) | Rare; heals spontaneously |
| Acquired perforating | Pruritic keratotic papules, legs | Collagen extrusion | DM + renal failure |
| Candidiasis/tinea | Intertrigo, onychomycosis | Immune dysfunction | All DM; onychomycosis precedes ulcers |
| Foot ulcers | Neuropathic (plantar) or ischemic (margins) | Neuropathy + PVD + pressure | 34% lifetime incidence |
Sources: Fitzpatrick's Dermatology, 9e (Ch. 137) | Andrews' Diseases of the Skin, Clinical Dermatology | Dermatology 2-Volume Set, 5e (Ch. 53) | Rosen's Emergency Medicine, 9e | Harrison's Principles of Internal Medicine, 22e
This is a shared conversation. Sign in to Orris to start your own chat.