Detailed note on Medicolegal autopsy for forensic medicine mbbs note
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
I have extensive content from the textbooks. Now I have enough to write a comprehensive MBBS-level medicolegal autopsy note. Let me compose it.
Medicolegal Autopsy - Comprehensive MBBS Notes
Sources: P C Dikshit Textbook of Forensic Medicine and Toxicology; The Essentials of Forensic Medicine and Toxicology (36th ed., 2026); Parikh's Textbook of Medical Jurisprudence, Forensic Medicine and Toxicology
1. DEFINITION
Autopsy (syn: necropsy, thanatopsy, postmortem examination) means examination of a body after death. The word derives from Greek - autos (self) + opsis (sight), meaning "to see for oneself."
In India, a complete autopsy is mandatory - every cavity must be opened and every organ examined. A partial autopsy has no place in forensic practice. A poor or incomplete autopsy is worse than no autopsy at all, as it is more likely to lead to a miscarriage of justice.
2. TYPES OF AUTOPSY
| Feature | Medicolegal Autopsy | Pathological (Clinical) Autopsy | Anatomical Autopsy |
|---|---|---|---|
| Conducted by | Forensic Medicine Dept. | Dept. of Pathology | Anatomists |
| Requested by | Police Officer / Magistrate | Relatives (consenting party) | Medical college (donated body) |
| Consent required | NOT required | Yes (relatives) | Yes (donor/family) |
| Extent | Complete - all cavities | Partial (organ suspected) | Varies |
| Main purpose | Cause, manner, time of death + evidence | Extent of disease, treatment efficacy | Teaching/study of body |
| Clinical history | Often absent, sketchy or misleading | Readily available | N/A |
| Scene visit | May be required | Not required | Not required |
3. OBJECTIVES OF MEDICOLEGAL AUTOPSY
- Establish identity of the deceased (unknown bodies) - using bodily appearance, anomalies, surgical scars, implants, fingerprints, dental records
- Determine cause of death (exact mechanism that killed the person)
- Determine manner of death - Natural / Accidental / Suicidal / Homicidal (NASH classification)
- Determine mechanism of death - which organ system failed first (brain, heart, or lung)
- Determine time since death - using postmortem changes (rigor mortis, livor mortis, decomposition, eye changes, etc.)
- Collect and preserve trace evidence - viscera, blood, hair, fibres, soil, foreign material
- In newborns - determine if dead-born or live-born, and cause of death
- Reconstruct the crime scene from injury patterns, their nature and duration
- Provide medicolegal documentation - admissible evidence in court
The forensic pathologist must also consider: crime scene, clothing, toxicological samples - aspects the general pathologist does not address.
4. PERMISSION FOR AUTOPSY
- A written request (inquest papers + "Request for Postmortem" form) must come from the police officer (minimum rank: ASI - Assistant Sub-Inspector)
- In murder cases, an Inspector is the investigating officer
- In certain cases (e.g. dowry deaths, custodial deaths), request comes from the Magistrate (who holds the inquest)
- Consent of relatives is NOT required for a medicolegal autopsy
- The history of the case must be obtained from the investigating officer or Sub-Divisional Magistrate (SDM); at times relatives or eyewitnesses may provide history
5. RULES / GUIDELINES FOR MEDICOLEGAL AUTOPSY
5.1 Labelling and Identification
- Body must be labelled as soon as it arrives in the mortuary
- Must be identified by the police constable accompanying it and by relatives
- Names of those who identify the body must be recorded
- For unidentified bodies: marks of identification, photographs, and fingerprints must be taken
5.2 Location of Autopsy
- Must be conducted in a mortuary - never in a private room
- Exceptions (autopsy at site):
- Body in advanced state of putrefaction and transportation is difficult
- Immediate examination needed without removal of the body
5.3 Time of Autopsy
- Should be done in daylight (artificial light may distort colour of bruises, wounds)
- Should not be conducted at night except in exceptional circumstances
5.4 Presence of Others
- A qualified Registered Medical Practitioner must conduct the autopsy
- Doctor must himself dissect and examine organs - not delegate to attendants
- Postmortem attendants (sweepers) assist in preparation and reconstruction only
- Police officer and sometimes relatives may be present
6. MORTUARY SETUP AND MINIMUM REQUIREMENTS
As per Bureau of Police Research and Development, Ministry of Home Affairs, Government of India:
- Located within hospital campus on a main road
- Minimum area: 400 square meters
- Autopsy room must be:
- Well-ventilated with illumination equivalent to sunlight
- Clean with plenty of running water
- Disinfected daily (phenol / savlon / glutaraldehyde 2%), weekly fumigation
- Universal work precautions followed
- Staff immunized: tetanus, TB, Hepatitis B
- Biomedical waste disposed per Biomedical Waste Management Rules, 2016
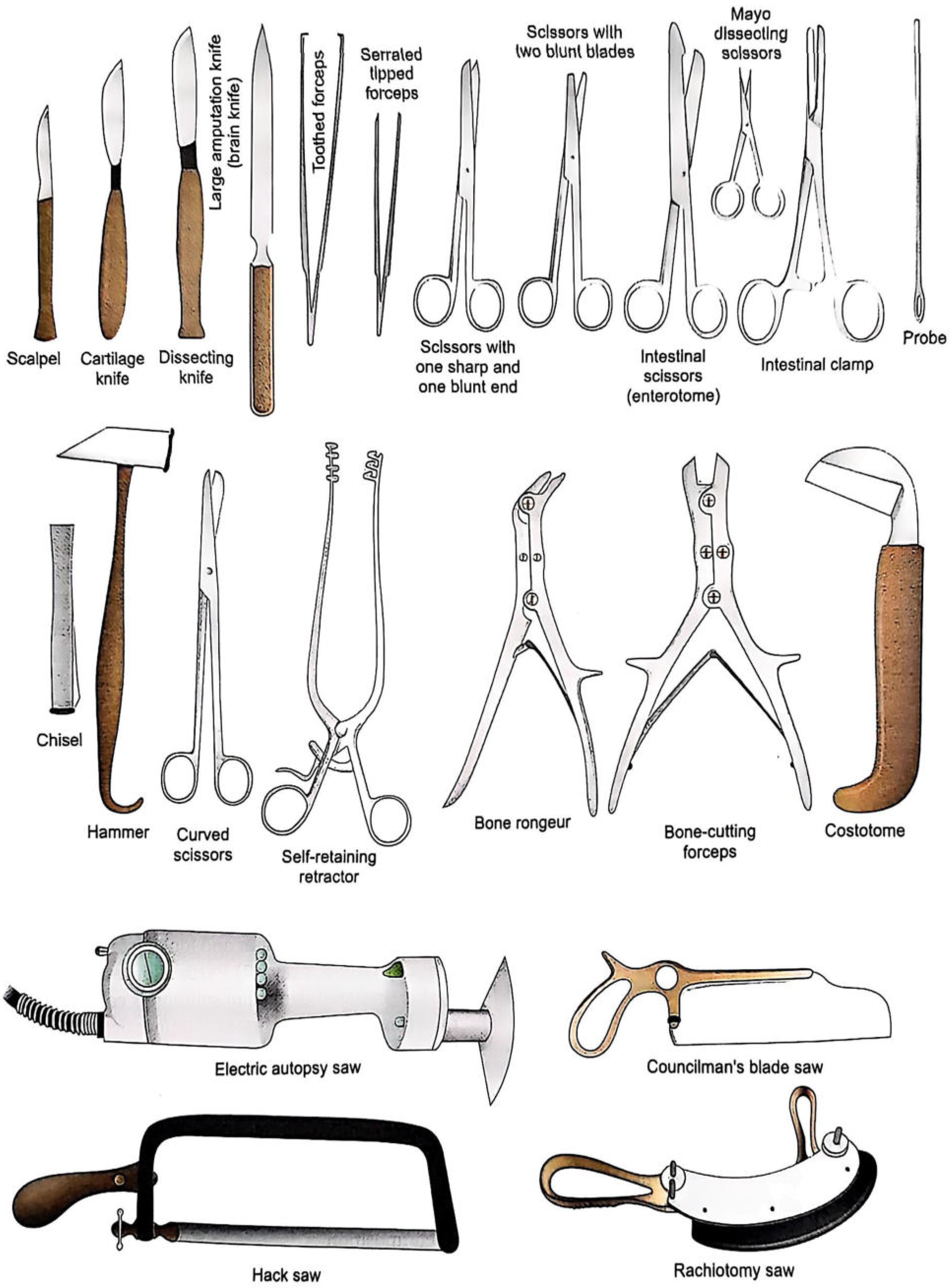
7. AUTOPSY INSTRUMENTS
Key instruments include: scalpels (post-mortem knife, cartilage knife), scissors (enterotome, rib shears), bone saw (vibrating saw / handsaw for skull), brain knife (large flat knife), forceps, hooks, chisels, hammer, weighing scale, organ basin, viscera jars (wide-mouthed airtight), measuring tape.
8. AUTOPSY PHOTOGRAPHY
Objectives:
- Visual record for pathologist to refer later
- Allow other professionals to review findings and form opinions
- Shown to judge at trial
- Teaching purposes
Techniques:
- Photos taken from above, at right angles to body (to avoid perspective distortion)
- Case number placed in corner of each photograph
- Violent deaths: front and back views of uncleaned body (with clothes), after removal of clothes, then washed naked body
- Unknown body: photograph of face
- Ligatures and bindings photographed before removal
- Close-up shots of major wounds with scale/ruler for dimensions
- Isolated organs: cleaned with sponge, placed on green cloth, photographed vertically
9. PROCEDURE OF MEDICOLEGAL AUTOPSY
Step 1: Pre-Autopsy Steps
- Receive inquest papers and postmortem request form
- Note the case number, date, time the body was received
- Body preserved in cold room (not wrapped in plastic bags - causes condensation and loss of trace evidence); wraps in clean white sheet
- Review history from investigating officer
- X-rays taken in all gunshot deaths and severely burnt bodies before autopsy
Step 2: External Examination (Examination Before Dissection)
The body is examined before any incision:
A. Clothing Examination:
- Examined for blood stains, trace evidence
- Tears/cuts in clothing correlated with bodily injuries
- Fingerprints taken only after examination of the hands
B. General Description:
- Age, sex, race, physique, height, weight, nutrition
- Congenital malformations
- Postmortem changes: rigor mortis (degree and distribution), postmortem staining/livor mortis (colour, distribution, blanchability)
C. Head and Face:
- Colour of eyes and hair
- Unusual appearance of ears, nose, face
- Teeth and dental plates
- Vomitus in nostrils and mouth
- Froth about mouth/nostrils (suggests drowning or pulmonary oedema)
- Smell: alcohol, phenol, bitter almonds (cyanide), garlic (arsenic/organophosphates)
D. Identification Marks:
- Scars, tattoos, moles - for identification purposes
E. Injuries:
- All recent external injuries (minor and major) described with: nature, site, length, breadth, depth, direction, position, margins, base and extremities
- Old injuries noted separately
- Evidence of recent medical/surgical intervention noted
- Determine: antemortem vs postmortem injury; time of infliction
F. Specific Areas:
- Hands: defense wounds, electric marks, needle marks; if clenched - examine contents (flexor tendons cut at wrist to open)
- Fingernails: blood, dust, foreign matter indicating struggle
- Limbs: oedema, needle puncture marks, fractures, dislocations
- Natural orifices (mouth, nostrils, ears, vagina): injuries, foreign matter, blood
- External genitalia: sexual abuse, injuries
- Tongue: position relative to teeth, bruising, bite marks
- Back: bedsores, spinal deformity
G. Wound Description System:
For each wound note: location (distance from anatomical landmarks), dimensions (length x breadth x depth), shape, margins (regular/irregular, inverted/everted), floor/base, direction, any foreign matter, associated findings
H. Gunshot Wounds (Special):
- Described in cm in relation to top of head or sole of foot, and relative to midline
- Features of entry wound: abrasion collar, soot, tattooing (range indicators)
- Course of bullet through body
- All organs perforated/penetrated noted
- If bullet exits: exit wound described in relation to entrance
- If bullet found: location, intact/deformed/fragmented, jacketed/unjacketed
10. INCISIONS FOR AUTOPSY
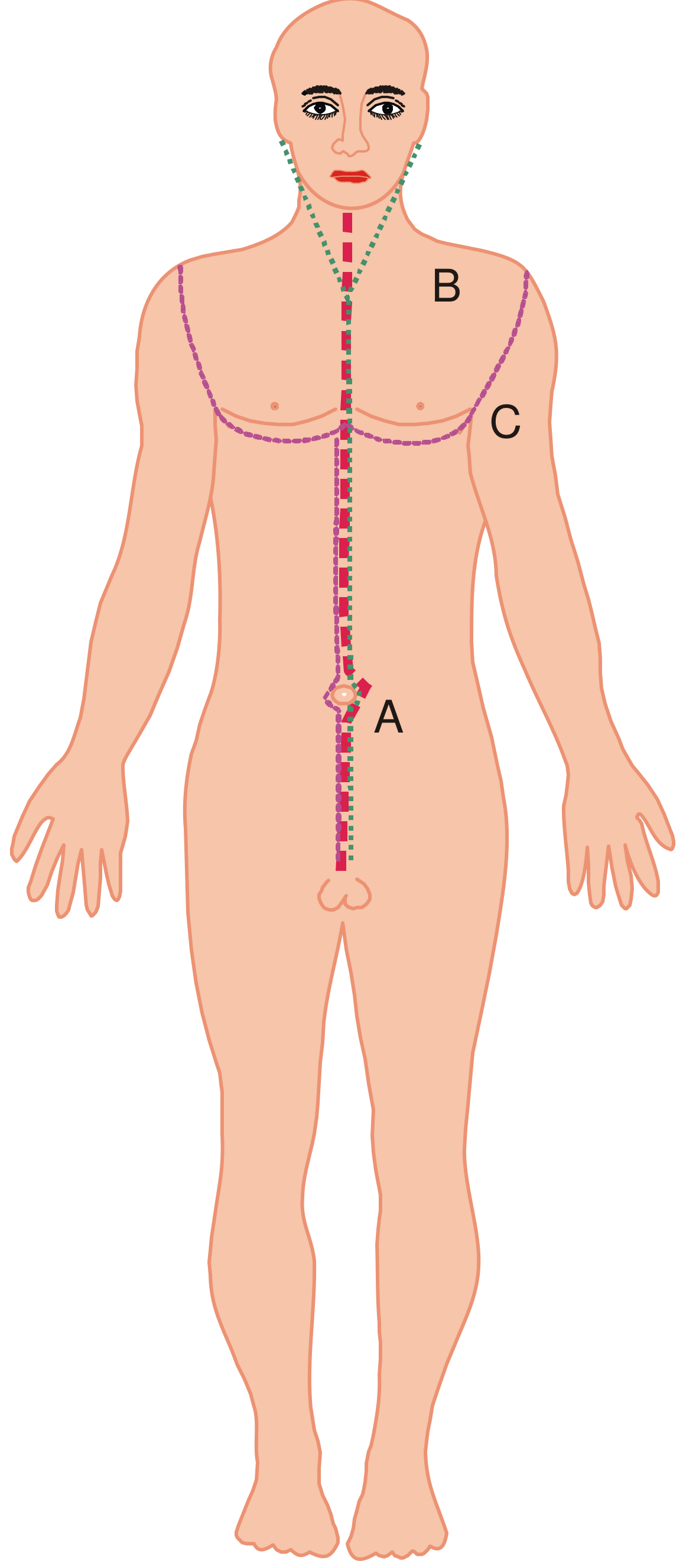
Three standard incisions are used:
-
'I' shaped incision: Extends from chin straight down to symphysis pubis, passing either side of umbilicus (umbilicus spared - dense fibrous tissue, difficult to stitch)
-
'Y' shaped incision: Starts near acromial process on both sides → extends below mammary line → up to xiphoid process → down to symphysis pubis on either side of umbilicus
-
Modified 'Y' shaped incision: From suprasternal notch to symphysis pubis (along midline by side of umbilicus) + extends from suprasternal notch to middle of clavicle on both sides → up to side of neck behind ear till mastoid process
11. DISSECTION TECHNIQUES (Methods of Evisceration)
Four classical techniques:
| Technique | Method | Advantage | Disadvantage |
|---|---|---|---|
| Virchow's | Organs removed one by one (cranial → spinal → thoracic → cervical → abdominal) | Each organ studied in detail | Anatomico-pathological relationships not preserved |
| Rokitansky's | In situ dissection + en bloc removal in part | Limits spread of infection (HIV, Hepatitis B) | Organs cannot be studied individually in detail |
| Letulle's | All thoracic, cervical, abdominal, pelvic organs removed en masse, then dissected as organ blocks | Best for routine inspection; preserves inter-organ connections; body available to undertaker in <30 min | Organ mass awkward to handle |
| Ghon's | Thoracic, cervical, abdominal organs and urogenital system removed as separate organ blocks | Preserves connections within system | - |
Most widely used: Virchow's technique. Preferred for HIV/Hepatitis risk: Rokitansky's.
12. INTERNAL EXAMINATION (Systematic Approach)
12.1 Cranial Cavity (Head)
- Scalp incision: coronal incision (ear to ear) behind the hairline
- Scalp reflected forward and backward; examine for subgaleal haemorrhage
- Skull cap removed with bone saw; examine calvaria for fractures (eggshell fractures, linear, depressed, comminuted)
- Dura examined; dural sinuses opened; subdural and extradural haemorrhage
- Brain removed: weighed (normal ~1400 g), examined for contusions, lacerations, herniation, cerebral oedema
- Brain sectioned (coronal sections) for deep lesions (basal ganglia, ventricles)
12.2 Neck
- Sternomastoid freed from clavicular/sternal attachments and reflected
- Omohyoid, sternothyroid, thyrohyoid muscles exposed
- Thyroid gland, carotid sheaths examined
- Larynx, trachea, pharynx, oesophagus mobilized
- Hyoid bone carefully examined (fracture = strangulation indicator)
- Deep neck dissection for petechiae, haemorrhage (important in asphyxia deaths)
12.3 Thoracic Cavity
- Ribs: examine for fractures (CPR injuries vs trauma)
- Pneumothorax test: Before opening chest - pocket dissected under skin on affected side, filled with water, wall punctured under water - if air bubbles out = pneumothorax confirmed
- Lungs examined: weight (normal ~500 g each), colour, consistency, cut surface, petechiae (Tardieu spots), froth (drowning/pulmonary oedema)
- Pericardial sac: amount and character of fluid; haemopericardium
- Heart: weight (normal ~300 g), chambers examined, valves, coronary arteries (LAD, RCA, LCx) sectioned transversely for stenosis/thrombosis
- Air embolism test: Heart opened under water - if air bubbles out = venous air embolism
12.4 Abdominal Cavity
- Assess peritoneal fluid (blood, bile, pus, chyle)
- Bowel: ligate duodenum and rectum with two ligatures each; intestine removed
- Stomach: ligated at gastro-oesophageal junction and pylorus; contents preserved for toxicology
- Spleen: weight (normal ~150 g), pulp reaction
- Liver: weight (normal ~1500 g), surface, cut section - congestion, fatty change, cirrhosis
- Kidneys: weight (~150 g each), cortex/medulla distinction
- Adrenals: look for haemorrhage (Waterhouse-Friderichsen syndrome)
- Urinary bladder: contents, mucosa
- Uterus and ovaries (in females): pregnancy, fibroid, malignancy
12.5 Pelvic Cavity
- Bladder, rectum, uterus/prostate examined
13. SPECIMENS COLLECTED AT AUTOPSY
| Specimen | Amount | Container | Preservative | Purpose |
|---|---|---|---|---|
| Stomach contents | Entire contents | Wide-mouthed jar | Saturated NaCl (common salt) | Toxicology |
| Blood | 20 mL | Plain tube | None (or fluoride for alcohol) | Toxicology, serology |
| Urine | Available amount | Sterile container | Nil (or sodium fluoride) | Toxicology |
| Liver | 500 g | Wide-mouthed jar | Saturated NaCl | Toxicology |
| Kidney | 500 g | Wide-mouthed jar | Saturated NaCl | Toxicology |
| Brain | 500 g | Wide-mouthed jar | Saturated NaCl | Toxicology |
| Vitreous humour | Both eyes | Syringe/tube | None | Toxicology, electrolytes |
| Hair | 10-15 strands (with roots) | Paper envelope | None | Heavy metals, DNA |
| Nails | Clippings | Paper envelope | None | Heavy metals |
| Bile | Available | Jar | Saturated NaCl | Drug analysis |
| Histology tissue | Formalin-fixed | Labelled jars | 10% formalin | Microscopy |
| Vaginal/anal swabs | - | Swabs | None | Sexual assault |
| CSF | Available | Sterile tube | None | Infection, toxicology |
Important: Preservative used is saturated solution of common salt (NaCl) for viscera - NOT formalin (destroys chemical composition needed for toxicology). Formalin is only for histological samples.
14. ORGAN WEIGHTS (Normal Reference Values - MBBS Important)
| Organ | Normal Weight |
|---|---|
| Brain (adult) | ~1400 g (M), ~1250 g (F) |
| Heart (adult) | ~300-350 g |
| Liver | ~1400-1500 g |
| Spleen | ~150 g |
| Kidney (each) | ~150 g |
| Lung (each) | ~500-600 g |
| Thyroid | ~20-25 g |
| Adrenal (each) | ~5-7 g |
15. SPECIAL AUTOPSIES
15.1 Negative Autopsy
- Autopsy in which no gross cause of death is found
- Causes: poisoning (requires toxicology), cardiac arrhythmia, epilepsy, hypoglycaemia, some drug deaths
- Complete toxicological analysis mandatory
- Histological examination of all organs required
- Also called "obscure autopsy" when cause cannot be established despite complete examination
15.2 Obscure Autopsy
- Extended version of negative autopsy
- Requires additional tests: toxicology, histology, microbiology, biochemistry
- Death may be due to: reflex cardiac arrest (vagal inhibition), hypersensitivity, functional disorders
15.3 Second Autopsy
- Conducted when the first autopsy is inadequate/incomplete
- May be requested by defence counsel, court, or deceased's relatives
- Second doctor must review first autopsy report before conducting the second
- Any discrepancies between the two reports may lead to issues in court
15.4 Pediatric Autopsy (Special Considerations)
- External: weight, height, head circumference, nutritional state
- Look for: diaper rash, insect bites, evidence of abuse (cigarette burns, bruises in various stages of healing)
- Eyes: subconjunctival haemorrhages, detached retina, displaced lens
- Genitalia: sexual abuse markers (pinching of scrotum, ligature to penis; puncture wounds in females)
- X-ray entire body: for skeletal changes from battering vs natural disease (scurvy, osteogenesis imperfecta)
- Brain: coup and contre-coup lesions (moving head vs fixed head)
16. CAUSE, MANNER, AND MECHANISM OF DEATH
| Term | Definition | Example |
|---|---|---|
| Cause of death | The disease/injury that initiated the chain of events leading to death | Gunshot wound to chest |
| Manner of death | Circumstances in which cause arose (NASH) | Homicidal |
| Mechanism of death | The physiological/biochemical derangement producing death | Haemorrhage → haemovolemic shock |
NASH Classification of Manner of Death:
- N - Natural
- A - Accidental
- S - Suicidal
- H - Homicidal
- (+Undetermined/Unknown as a 5th category)
17. AUTOPSY PROTOCOL (REPORT)
The autopsy protocol is a signed legal document serving as proof of findings. Two forms:
- Narrative form - story form, descriptive
- Numerical form - by numbers/points
Contents of Postmortem Report:
- Preamble: date, time, place of autopsy; name of doctor; case number; police station; name of deceased (if known)
- History of the case
- External examination findings
- Internal examination findings (organ by organ)
- Specimens/viscera preserved (with details)
- Opinion on: cause of death, manner of death, time since death
- Signature of conducting doctor
The postmortem report is a medicolegal document - it may be used as evidence in court. The doctor may be called as an expert witness.
18. SAFETY PRECAUTIONS AT AUTOPSY
- Universal precautions must always be followed
- Double gloves, mask, eye protection, gown, boots
- Staff immunized: Tetanus, Hepatitis B, tuberculosis
- All instruments washed with disinfectants after use
- Biomedical waste disposed per BMW Rules, 2016
- For high-risk cases (HIV, Hepatitis B, Hepatitis C, TB): Rokitansky's technique preferred (en bloc removal limits aerosolization and spread)
19. MEDICOLEGAL AUTOPSY IN FATAL DROWNING (Special Note)
Key findings to look for:
- Frothy fluid from nose/mouth (fine persistent froth)
- Waterlogged lungs (emphysema aquosum)
- Fine froth in airways and alveoli
- Diatoms in lungs, liver, bone marrow (specific for drowning)
- Haemoconcentration in salt-water drowning; haemodilution in fresh-water drowning
- Washerwoman's hands (cutis anserina - goose skin)
20. KEY EXAM POINTS (High-Yield MBBS Summary)
| Point | Fact |
|---|---|
| Medicolegal autopsy - consent needed? | No - requested by police/magistrate |
| Rank of officer requesting autopsy | Minimum ASI (murder = Inspector) |
| Preservative for viscera (toxicology) | Saturated NaCl (common salt solution) |
| Preservative for histology | 10% formalin |
| Most widely used dissection technique | Virchow's (organ by organ) |
| Technique for infectious risk cases | Rokitansky's (en bloc) |
| Best technique for organ relationships | Letulle's (en masse) |
| Standard incision used in India | Modified 'Y' or 'I' shaped |
| Autopsy photography: colour for bruise age | Colour photographs show age differences |
| Gunshot deaths: pre-autopsy step | X-ray before beginning dissection |
| Hyoid bone fracture suggests | Strangulation |
| Pneumothorax test at autopsy | Pocket under skin + water + puncture |
| Air embolism test | Heart opened under water |
| "Negative autopsy" means | No gross cause found - toxicology mandatory |
| NASH classification | Natural, Accidental, Suicidal, Homicidal |
These notes are compiled from: P C Dikshit Textbook of Forensic Medicine and Toxicology, The Essentials of Forensic Medicine and Toxicology (36th ed., 2026), and Parikh's Textbook of Medical Jurisprudence, Forensic Medicine and Toxicology.
Detailed note on postmortem artefacts
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have thorough content from all three major forensic textbooks. Let me compile the comprehensive note.
Postmortem Artefacts - Comprehensive MBBS Notes
Sources: P C Dikshit Textbook of Forensic Medicine and Toxicology; The Essentials of Forensic Medicine and Toxicology (36th ed., 2026); Parikh's Textbook of Medical Jurisprudence, Forensic Medicine and Toxicology
1. DEFINITION
An artefact (or artifact) is:
"Any change caused or a feature introduced into a body after death that is likely to lead to misinterpretation of medicolegally significant antemortem findings."
- P C Dikshit Textbook of Forensic Medicine and Toxicology
Dorland's Illustrated Medical Dictionary defines it as: "Any artificial product; any structure or feature that is not natural, but has been altered by processing."
In forensic pathology: an artefact is any unrelated change or feature introduced in the body after death - either accidentally or due to physiologically irrelevant factors - that can mislead interpretation of significant antemortem findings. It is a structure or substance not normally present but produced by an external or internal agent or action.
2. IMPORTANCE / MEDICO-LEGAL SIGNIFICANCE
Misinterpretation of artefacts can result in:
- Wrong cause of death
- Wrong manner of death (natural labelled as homicide, or vice versa)
- Undue suspicion of criminal offence against innocent persons
- Halt in investigation of a homicide - a murder goes undetected
- Miscarriage of justice in civil suits
- Unnecessary expenditure of time and effort due to misleading findings
The responsibility of the autopsy pathologist is immense - the doctor is often the primary source of evidence upon which crucial legal decisions are based, including those that may determine the freedom, imprisonment, or even the life or death of an accused person.
3. CLASSIFICATION OF POSTMORTEM ARTEFACTS
POSTMORTEM ARTEFACTS
│
├── A. ARTEFACTS INTRODUCED BETWEEN DEATH AND AUTOPSY
│ ├── (I) Agonal artefacts
│ ├── (II) Resuscitation artefacts
│ ├── (III) Handling/Transportation artefacts
│ ├── (IV) Artefacts related to Rigor Mortis
│ ├── (V) Artefacts related to Postmortem Lividity (Hypostasis)
│ ├── (VI) Decomposition artefacts
│ ├── (VII) Animal/Fauna artefacts
│ ├── (VIII)Embalming artefacts
│ └── (IX) Internment and Exhumation artefacts
│
└── B. ARTEFACTS INTRODUCED DURING AUTOPSY
├── (I) Anatomical/dissection artefacts
├── (II) Cranial/brain artefacts
├── (III) Neck dissection artefacts
├── (IV) Toxicological artefacts (sampling errors)
└── (V) Gunshot wound artefacts (autopsy-related)
A. ARTEFACTS INTRODUCED BETWEEN DEATH AND AUTOPSY
(I) AGONAL ARTEFACTS
Agonal period = the time between cardiorespiratory arrest and brain death/dysfunction.
1. Regurgitation and Aspiration of Gastric Contents
- The most common agonal artefact
- May occur in:
- Natural deaths as a terminal event
- Body handling after death
- During resuscitation attempts
- Asphyxia (induces vomiting due to medullary suboxia)
- Medico-legal problem: Physicians may wrongly give "aspiration of gastric contents" as the cause of death
- Differentiating true antemortem aspiration (choking): In choking, food particles are drawn into bronchioles. When food rises up the oesophagus and enters the larynx after death, it does not go beyond secondary bronchioles
- Test: Histopathological examination of lung tissue - if food particles are found beyond secondary bronchioles, it indicates antemortem aspiration (genuine cause of death)
- Important in infants: Do not assume gastric contents in airways = cause of asphyxia; it is more likely the result
2. Oesophagogastromalacia
- Rare agonal artefact
- Seen in people dying within hours or days of severe head injury
- Caused by autodigestion (autolysis) of the oesophagus and stomach wall
- Leads to spillage of stomach contents into left chest cavity or left subphrenic area
- Affected tissue appears greyish-white to black and is very friable
- May occur just before or shortly after death
- Simulate antemortem burns or corrosive ingestion
(II) RESUSCITATION ARTEFACTS
Attempts at cardiopulmonary resuscitation (CPR), defibrillation, and drug injection can leave marks that mimic injuries, drug abuse, or natural disease.
1. Injection Marks
- Seen in cardiac region (intracardiac injection) or extremities
- Intracardiac injection may cause:
- Bruising/contusion of the heart
- Blood collection in the pericardium (haemopericardium)
- Must be differentiated from marks of drug abuse or homicidal injection
2. Defibrillator Marks
- Applied paddles produce ring-like contusions over the chest
- Superficial skin burns resembling the shape of the conductive material
- Skeletal muscle necrosis from transthoracic defibrillation
- Must not be confused with contact burns or electrocution marks
3. External Cardiac Massage (CPR)
- Bruising of anterior chest wall
- Haemorrhages in subcutaneous tissues and pectoral muscles
- Symmetrical, parasternal rib fractures (multiple) - most classic CPR artefact
- Sternal fractures (through body and manubrium)
- Tears of the lungs with release of free air into tissues (pneumothorax)
- Haemorrhages in lungs (hexagonal foci of aspirated blood - subpleural)
- Rupture of atria and ventricles (rarely)
- Lacerations of the liver (direct manipulation + push-pull effect on liver ligaments/diaphragm)
- Splenic lacerations (less common)
Key Point for CPR fractures: In CPR-induced rib fractures, bleeding is usually absent at the fracture site and no haemorrhage is seen in intercostal muscles. The lungs may show bone marrow or fat emboli. In such cases, a careful history of resuscitative measures must be obtained.
4. Positive Pressure Ventilation
- Acute emphysema
- Subpleural blebs
- Air in mediastinum
- Tension pneumothorax
- These should not be misinterpreted as spontaneous pneumothorax or blast injury
(III) HANDLING AND TRANSPORTATION ARTEFACTS
Injuries inflicted during transfer of the body from scene of death to mortuary.
- Fractures - rib fractures or fractures of extremities from rough handling, especially in severe osteoporosis; also produced while straightening limbs contracted in rigor mortis - bleeding is usually absent at these fracture sites
- Undertaker's fracture - subluxation of lower cervical spine (C6-C7) due to tearing of the intervertebral disc; caused by rough handling/traction
- Contusion of the occipital region - if head of corpse allowed to fall on hard surface
- Fresh abrasions - from dragging the body during transfer from the scene of crime
(IV) ARTEFACTS RELATED TO RIGOR MORTIS
- Breaking of rigor during handling → false (premature) estimate of time since death
- Altered onset/duration of rigor - by environmental conditions (extreme heat, cold) or antemortem conditions (hyperthermia from infections, muscular exhaustion, wasting diseases)
- Cardiac rigor - rigor of the heart muscles causes stiffening simulating concentric hypertrophy of the heart (mistaken for hypertensive heart disease)
- Gastric rigor - may accentuate rugae or fix a point of contraction → pseudo-hourglass stomach (readily removed by traction - distinguishes from true constriction)
- Pyloric rigor - pylorus appears unduly firm and contracted → simulates pyloric stenosis
(V) ARTEFACTS RELATED TO POSTMORTEM LIVIDITY (HYPOSTASIS)
The typical colour of postmortem lividity is bluish-purple.
1. Colour Changes Mimicking Poisoning:
| Colour of Lividity | Simulates / May be mistaken for | Actual cause |
|---|---|---|
| Cherry-red | Carbon monoxide poisoning | Can also be genuine CO poisoning - must correlate with HbCO levels |
| Bright-red | Cyanide poisoning | Cold exposure also produces red/pink lividity |
| Chocolate-brown | Nitrite, potassium chlorate, aniline poisoning | Methemoglobinaemia |
| Dark-brown | Phosphorus poisoning | - |
| Pink/haemorrhagic patches | Bruising, trauma | Cold exposure, refrigerated body |
2. Posterior Neck Haemorrhage (Cervical Spine Area)
- Patches of haemorrhage, sometimes quite large and confluent, can occur in tissues behind the oesophagus at the level of the larynx (anterior surface of cervical vertebrae)
- Caused by distension and leakage from venous plexuses in this area due to hypostasis
- Can be mistaken for haemorrhage due to strangulation - this is one of the most important artefacts in forensic practice
- Prevention: Neck dissection must be meticulous, avoiding seepage of blood from neck vessels
3. Oesophageal Banding
- "Banding" of the oesophagus = pale bands in the mucosa
- Caused by postmortem hypostasis being prevented from settling by the external pressure of adjacent anatomical structures (larynx, trachea, aortic arch)
- Seen especially when tissues are congested
- Commonly seen in routine non-traumatic autopsies
- Must not be mistaken for strangulation marks or corrosive injury
4. Petechiae / Ecchymoses
- Large petechiae or ecchymoses, sometimes with raised blood blisters, may be seen in the skin of the dependent areas of the body (especially face and neck in prone position)
- These are due to rupture of capillaries due to hypostasis
- Must not be mistaken for mechanical asphyxia petechiae or bruises
5. Scalp "Bruises" / Haemorrhages
- Common autopsy artefact during reflection of scalp flaps in all types of death
- Caused by normal postmortem hypostasis in dependent scalp areas
- Of no significance
- Commonly present in normal postmortem hypostasis, especially where body has been lying
(VI) DECOMPOSITION ARTEFACTS
Decomposition produces numerous changes that may simulate antemortem pathology.
A. External Changes Mimicking Trauma or Disease:
- Swelling of face (lips, nose, eyelids), protrusion of eyes, distension of chest and abdomen, swelling of extremities → false impression of antemortem obesity
- Purge fluid (decomposition fluid from nose, mouth) - dark reddish-brown fluid = frequent finding in decomposed bodies
- Marked especially in pulmonary oedema
- Must NOT be mistaken for haemorrhage from head injury or poisoning
- Accumulation of blood in neck tissues in drowning → simulates antemortem haemorrhage due to strangulation
- A deep groove around the neck in decomposed bodies (also in mummification) if the deceased was wearing a buttoned shirt at time of death → simulates ligature mark of strangulation
- Skin fissures/splits due to putrefaction → simulate antemortem lacerations or incised wounds
- Small round holes from maggots → simulate bullet holes
- Excessive flaccidity of vaginal orifice with effusion of fluid → simulate sexual assault
- Blebs from putrefaction → mistaken for blebs/blisters from burns
- Regurgitated gastric juices causing tanning of skin of face and neck → simulate antemortem burning (chemical burns)
- Separation of sutures of skull in a child (due to gases of decomposition within brain) → NOT trauma
- Bursting of abdomen with protrusion of viscera (advanced decomposition) → NOT traumatic evisceration
B. Internal Changes Mimicking Disease:
- Dark blood (blood becomes darker in decomposition) → brain, lungs, heart appear congested → mistaken for signs of asphyxia
- Gas collection in tissues, cavities, hollow viscera under pressure, and emphysematous subcutaneous tissue → subcutaneous emphysema may simulate antemortem trauma
- Air in right side of heart (decomposition gas) → mistaken for ante-mortem air embolism
- Differentiation: Oxygen in the right heart indicates true air embolism (not present in appreciable quantity in decomposition gas). Volume of air in true embolism is much larger
- Miliary granules/plaques (1-3 mm diameter) on serous surfaces (pleura, peritoneum, pericardium, endocardium) in advanced decomposition:
- Appear grayish-white, resemble bacterial colonies on agar
- Consist of calcium, fat, endothelial cells, and bacteria
- Must NOT be mistaken for inflammatory lesions or effect of a poison
- Pancreatic autolysis - the pancreas is the most vulnerable organ:
- First: softened and haemorrhagic
- Later: resembles haemorrhagic pancreatitis
- Histological changes of necrosis within a few hours after death
- Inflammatory reaction and fat necrosis are absent (distinguishes from true pancreatitis)
- Pulmonary bacterial colonies - lungs show postmortem bacterial colonies
(VII) ANIMAL / FAUNA ARTEFACTS
- Rodent bites - most common in urban environments; characteristic teeth marks; commonly seen in bodies stored in mortuaries/cold rooms
- Bird bites / animal bites - produce confusing marks but bear characteristic features
- Insect activity - maggot holes simulate bullet wounds; insect activity can remove tissue and distort wound patterns
- Fish bites in water bodies - may simulate knife wounds or blunt trauma
- Dog/cat bites - may tear soft tissue, simulating injury patterns
All animal bites must be carefully identified by their characteristic tooth or mark pattern.
(VIII) EMBALMING ARTEFACTS
- Trochar holes from embalming may be confused with gunshot wounds or stab wounds
- The track of a weapon or bullet may be disturbed by trochar insertion, creating false tracks
- Surgical alteration or suturing of gunshot wounds before the autopsy → complicates evaluation (Kennedy phenomenon - named after the JFK autopsy controversy)
- Embalming fluids (formaldehyde, methyl alcohol, other compounds) cause:
- Confusion when analysing viscera for drugs/chemicals
- EDTA, formalin, heparin and methenamine give a positive test for methanol → false-positive methanol poisoning
(IX) INTERNMENT AND EXHUMATION ARTEFACTS
In bodies interred in soil and later exhumed:
- Fungal growth - common at body orifices, eyes, and site of open injuries; underlying skin is discoloured simulating bruising
- Soil contaminants and draining water alter chemical composition of viscera
- All previous artefact types (agonal, resuscitative, embalming, handling) may still be present at the time of exhumation and must be borne in mind
- Toxicological analysis is significantly complicated by leaching and bacterial action
B. ARTEFACTS INTRODUCED DURING AUTOPSY
(I) ANATOMICAL / DISSECTION ARTEFACTS
- Fractures during rough removal of organs - ribs, extremity bones (especially in osteoporosis)
- Artificial damage to pontomedullary region or midbrain-pons junction due to rough removal of the brain
- Uncal grooving - found in normal brains as an artefact due to pressure from tentorial edge; must not be mistaken for herniation from raised intracranial pressure
(II) CRANIAL / BRAIN ARTEFACTS
- Regional flattening of cerebral convolutions - a common postmortem artefact:
- Seen in parts of the brain in contact with the cranium, particularly the dependent (occipital) parts
- Shows flattening; must NOT be mistaken for cerebral oedema or gyral flattening from raised ICP
- Subarachnoid haemorrhage as an artefact - may be produced during removal of the brain due to:
- Damage to cerebral veins
- Tearing of the arachnoid
- Must be distinguished from true traumatic/spontaneous SAH
(III) NECK DISSECTION ARTEFACTS
- During neck dissection, blood may seep from neck vessels into the soft tissues
- This seepage into the perihyoid and perivisceral tissues of the neck simulates antemortem bruises seen in throttling and strangulation
- Prevention: Neck dissection must be meticulous, performed after the body has been drained of blood (ideally after opening the thorax first and draining blood from thoracic vessels)
- Manubriosternal dissection first principle: Thorax should be opened before neck dissection in strangulation cases to prevent this artefact
(IV) TOXICOLOGICAL ARTEFACTS (During Sampling)
1. Faulty Technique in Collecting Blood Samples:
- Drawing blood from the heart with a long needle may result in contamination with gastric contents
- Tests for alcohol then become misleading
- In traumatic deaths (road accidents), the stomach may have ruptured → increased likelihood of contamination
- Alcohol diffusion: Alcohol diffuses in significant amounts from the stomach to pleural and pericardial cavities → unreliable results if blood is drawn from these spaces
2. Faulty Technique in Storage:
- Cutting organs with instruments contaminated by stomach contents
- Using contaminated containers
- Storing portions of several organs in one container (common practice but incorrect) → diffusion/drainage of blood/fluid from one organ to another → altered true concentration of poisons
3. Use of Wrong Preservatives:
| Preservative | Problem |
|---|---|
| EDTA | Gives positive test for methanol |
| Formalin | Gives positive test for methanol; destroys chemical composition |
| Heparin | Gives positive test for methanol |
| Methenamine | Gives positive test for methanol |
| Common salt (NaCl) - saturated | Correct preservative for toxicology viscera |
(V) GUNSHOT WOUND ARTEFACTS (At Autopsy)
- Drainage holes from surgical procedures (chest drains, abdominal tubes) may be confused with gunshot wounds
- Embalmer's trochar holes may be confused with gunshot entry wounds
- Surgical alteration or suturing of the wounds → difficult to evaluate wound characteristics (Kennedy phenomenon)
- In decomposed bodies: gunshot wounds may be greatly modified - lose their characteristic features
DECOMPOSITION TOXICOLOGICAL ARTEFACTS
(Important separate topic that combines decomposition and toxicology)
| Substance | Artefact produced | Significance |
|---|---|---|
| Alcohol (ethanol) | Produced by putrefaction (bacterial fermentation) | Usually <100 mg% postmortem; if >100 mg% → suspicion of antemortem ingestion |
| Carboxyhaemoglobin (CO-Hb) | Decomposition increases COHb levels | Increase of 19-25% reported; may falsely suggest CO poisoning |
| Cyanide | Produced by decomposition in toxicologically significant amounts | Up to 10 mg% found in 3-month-old blood specimens |
| Phenols | Substituted phenols found in decomposing tissues | Cause interference in weak acid fraction analysis |
| Combustion gases (in burned bodies) | Ammonia, CO, HCN, H₂S, nitrogen oxides, SO₂ | Cyanide levels 17-220 mg/100 mL in burn victims; may raise false alarms |
4. SUMMARY TABLE: KEY ARTEFACTS AND WHAT THEY MIMIC
| Artefact | What it Mimics |
|---|---|
| Gastric aspiration (agonal) | Cause of asphyxia / choking |
| CPR rib fractures | Blunt trauma / battery |
| Intracardiac injection mark | Drug abuse; homicidal injection |
| Defibrillator burn | Electrocution; contact burns |
| Cardiac rigor | Concentric hypertrophy (hypertensive heart disease) |
| Gastric rigor (hourglass stomach) | True hourglass deformity / pyloric obstruction |
| Posterior neck hypostasis haemorrhage | Strangulation / throttling bruising |
| Oesophageal banding | Corrosive injury; strangulation mark |
| Cherry-red lividity | Carbon monoxide poisoning |
| Decomposition skin fissures | Incised/lacerated wounds |
| Maggot holes | Bullet wounds |
| Deep neck groove (shirt collar in decomposition) | Ligature strangulation |
| Brain regional flattening | Cerebral oedema / raised ICP |
| Subarachnoid haemorrhage at autopsy | Traumatic or spontaneous SAH |
| Undertaker's fracture (C6-C7) | Antemortem cervical injury |
| Uncal grooving | Cerebral herniation |
| Pancreatic autolysis | Haemorrhagic pancreatitis |
| Fungal growth over eyes (exhumed body) | Bruising |
| Air in right heart (decomposition) | Antemortem air embolism |
| Trochar holes (embalming) | Gunshot wounds |
| Postmortem lividity (dependent areas) | Bruises |
| Oesophagogastromalacia | Corrosive ingestion; antemortem burns |
5. KEY EXAM POINTS (High-Yield Summary)
| Point | Answer |
|---|---|
| Definition of artefact in forensic pathology | Any change introduced in body after death that misinterprets antemortem findings |
| Most common agonal artefact | Regurgitation and aspiration of gastric contents |
| CPR artefact most useful in battered baby cases | Symmetrical parasternal rib fractures (bleeding absent) |
| Preservative causing false-positive methanol | EDTA, formalin, heparin, methenamine |
| Correct preservative for toxicology viscera | Saturated NaCl (common salt) |
| Posterior neck haemorrhage at autopsy mimics | Strangulation bruising |
| Prevention of neck dissection artefact | Drain thoracic blood first; meticulous neck dissection |
| "Kennedy phenomenon" | Surgical suturing/alteration of gunshot wound complicating evaluation |
| Undertaker's fracture | Subluxation at C6-C7 due to rough handling |
| Gastric regurgitation - confirmatory test for antemortem | Food particles beyond secondary bronchioles on histology |
| Alcohol generated by putrefaction | Usually <100 mg%; >100 mg% = suspect antemortem ingestion |
| Cyanide from decomposition (max levels) | Up to 10 mg% in 3-month-old blood |
| Pancreatic artefact in decomposition | Resembles haemorrhagic pancreatitis; no fat necrosis/inflammation |
| Animal bite simulating bullet wound | Maggot holes |
| Artefact from wearing a buttoned shirt at death | Deep groove in neck (decomposed body) - simulates ligature mark |
| Most vulnerable organ to postmortem autolysis | Pancreas |
| Cardiac rigor mimics | Concentric cardiac hypertrophy |
| Uncal grooving significance | Common artefact - NOT cerebral herniation |
Sources: P C Dikshit Textbook of Forensic Medicine and Toxicology (pp. 112-116); The Essentials of Forensic Medicine and Toxicology, 36th edition, 2026 (Chapter 21); Parikh's Textbook of Medical Jurisprudence, Forensic Medicine and Toxicology
Coup vs contre coup injuries
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive, multi-source content. Let me compile the detailed note.
Coup vs Contrecoup Injuries - Comprehensive MBBS Notes
Sources: P C Dikshit Textbook of Forensic Medicine and Toxicology; The Essentials of Forensic Medicine and Toxicology (36th ed., 2026); Parikh's Textbook of Medical Jurisprudence, Forensic Medicine and Toxicology; Robbins Pathology
1. ETYMOLOGY AND DEFINITIONS
| Term | Origin | Definition |
|---|---|---|
| Coup | French: coup = blow | Injury beneath (at) the site of impact - directly caused by the impacting force |
| Contrecoup | French: contre = opposite + coup = blow | Injury opposite to the site of impact - at the far side of the brain from where the blow landed |
| Intermediate coup | - | Injury situated between the coup and contrecoup points - usually in brainstem or deep parenchyma |
The smaller the area of impact, the greater the likelihood of a coup injury.
2. MECHANISM
The Core Biomechanical Concept
The brain is a semi-solid, jelly-like mass suspended inside a rigid skull, cushioned by CSF. When the head is struck or falls, the brain undergoes relative movement within the skull.
Two key scenarios:
SCENARIO A: MOVING OBJECT strikes a FIXED HEAD
→ Larger COUP injury beneath point of impact
→ Small or absent contrecoup injury
→ Example: Being hit with a bat while standing still
SCENARIO B: MOVING HEAD strikes a FIXED SURFACE (falls/deceleration)
→ Small or absent coup injury
→ LARGER CONTRECOUP injury at the opposite pole
→ Example: Falling and hitting the back of the head on the pavement
3. DIAGRAMMATIC ILLUSTRATION
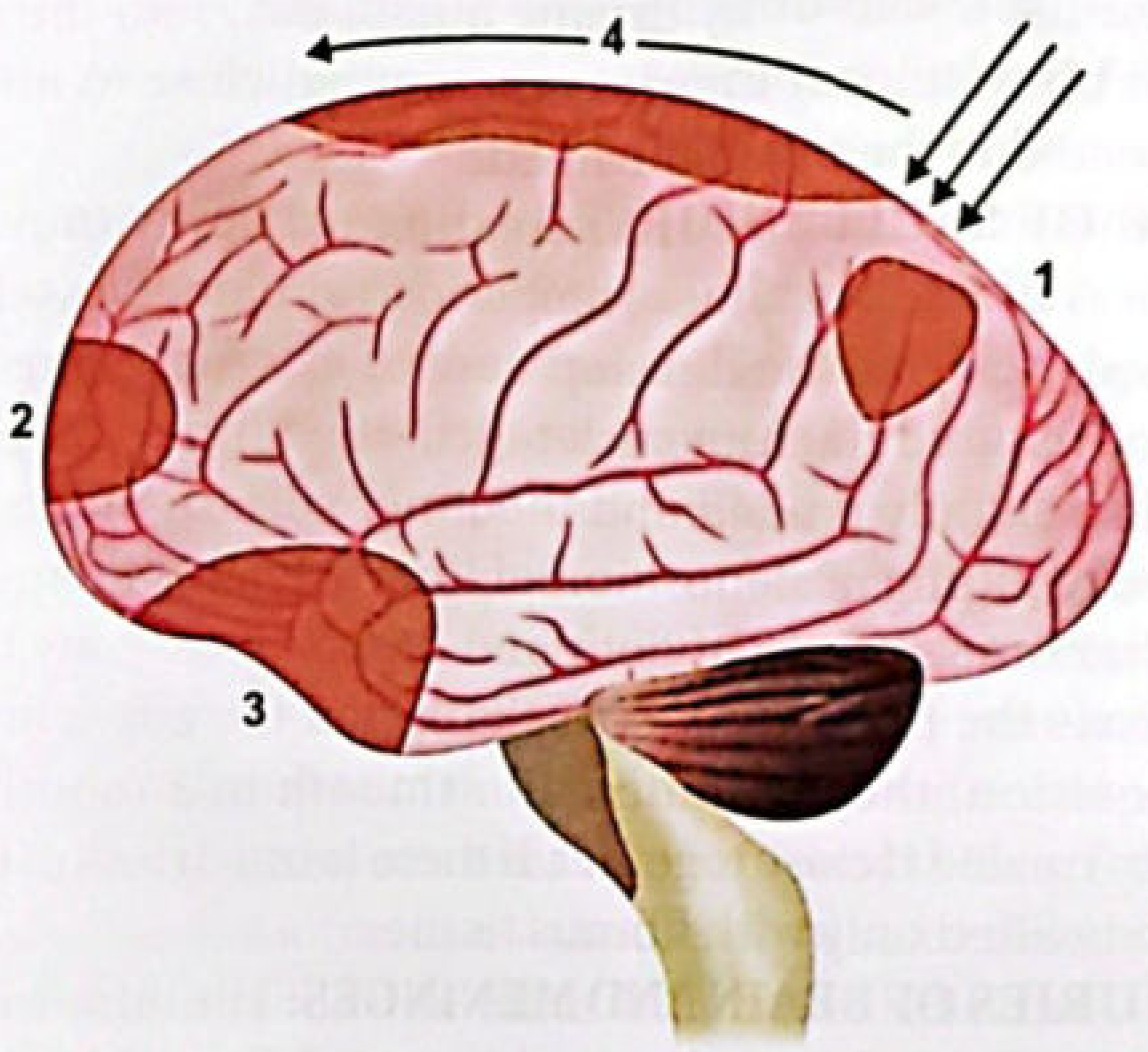
Fig: (1) = Coup injury at site of impact (right); (2) = Contrecoup injury at opposite side (left frontal); (3) = Dashboard injury at sphenoidal ridge; (4) = Avulsion of rotary vein along superior hemisphere border
4. THEORIES OF CONTRECOUP INJURY
Six classical theories explain how injury occurs at the opposite side of impact:
1. Struck Hoop Theory
- Due to the elasticity of the skull, the skull flattens at the point of impact
- The skull momentarily assumes an ovoid shape
- This deformation transmits force and damages the opposite side of the brain
- Analogy: striking a hoop causes it to deform, transmitting force to the opposite arc
2. Russell's Theory (Brain Displacement Theory)
- The brain, acting as a jelly mass, is suddenly displaced towards the impact site
- A potential space (vacuum) develops on the opposite side
- This negative pressure tears vessels and causes subdural and cortical injuries on the contralateral side
3. Gaggio's Pressure Gradient Theory
- At the moment of impact:
- Positive pressure develops at the side of impact (coup side)
- Negative pressure (cavitation) develops on the opposite side
- The sudden negative pressure bursts vessels on the contralateral side
- This is essentially a cavitation phenomenon
4. Holbourn's Shear Strain Theory (Most widely accepted)
- An Oxford physicist (1943)
- Contrecoup lesions are chiefly due to:
- Local distortion of the skull at the point of impact
- Sudden rotation of the head, which causes shear strains - the pulling apart of constituent particles of the brain in directions parallel to their planes of contact
- Because the changes in rotational velocity are greatest at the pole opposite the impact, contrecoup injuries are more extensive
- A line drawn between the centres of coup and contrecoup indicates the direction of impact relative to the head
5. Deceleration Theory
- When the moving head is suddenly decelerated by hitting a firm surface, the brain (still in motion) strikes the inner surface of the now-stationary skull on the opposite side
- The brain's inertia causes it to travel forward and impact the far wall
- Example: falling and striking the occiput - brain continues moving forward and hits the inner frontal skull
6. Rawling's Theory (Bony Irregularities)
- Irregular bony prominences - particularly the cribriform plate, orbital plates, and lesser wings of sphenoid - contuse and lacerate the base of the frontal lobes and tips of the temporal lobes
- A blow to the front of the head may damage the inner and lower parts of the back of the brain by contact with the edges of the tentorium → brainstem injury and pontine haemorrhage
- A blow to one side may cause injury on the opposite side by brain contact with the falx cerebri
7. Cavitation Theory (Fall on Side)
- Fall on the side of the head causes formation of a cavity or vacuum in the cranial cavity on the side of impact
- The brain is suddenly sucked toward this cavity
- A contusion on the opposite side of the brain results from this sudden displacement
5. CLASSICAL EXAMPLE (Medico-Legal Application)
"Just before closing time in a certain public house, a slightly inebriated young man suspected another of having insulted his mother. Some time later, the second young man was found dead in the gutter, with a bruise on the chin, two black eyes, and a cut on the back of the head. The rapidly sobered assailant stoutly maintained that he had struck the victim only one blow on the chin, but a charge of at least manslaughter hung over him - until the autopsy. This displayed that there was a fracture of the back of the head and severe contrecoup injury to the front of the brain, resulting in bleeding into the eye-sockets, giving the impression of black eyes. This substantiated the story of a single blow on the chin, with subsequent cracking of the back of the head on the pavement edge."
- Parikh's Textbook of Medical Jurisprudence, Forensic Medicine and Toxicology
This case illustrates how contrecoup injuries can exonerate or implicate an accused person and determine the number of blows delivered.
6. SITE-SPECIFIC INJURY PATTERNS
| Site of Impact | Coup Injury | Contrecoup Injury |
|---|---|---|
| Back of head (occiput) - fall backwards | Little or no occipital contusion; possible posterior cerebellar contusion | Subfrontal + temporal lobe contusion (most common scenario) |
| Top of head (vertex) | Minimal coup contusion | Prominent subtemporal / uncal contusion; subcerebellar contusion; posterior fossa subdural haemorrhage; corpus callosum laceration in severe impacts |
| Side of head (temporal) | Lateral coup lesion | Contrecoup on lateral aspect of opposite hemisphere; may be on ipsilateral hemisphere against falx cerebri (not necessarily the contralateral side) |
| Front of head (forehead) | Frontal coup laceration in severe injury | Occipital contrecoup is rare/virtually unknown |
Key rule: It is virtually unknown for a fall on the frontal region to produce occipital contrecoup injury. This asymmetry is forensically important.
7. CHARACTERISTIC FEATURES OF EACH
Coup Injury
- Located at the site of impact - beneath the blow
- Results directly from the impacting force
- More prominent when a moving object strikes a fixed/stationary head
- Smaller impact area = greater likelihood of coup injury
- Fracture of skull most likely at the coup site
- Contusions, lacerations, haemorrhage immediately subjacent to impact
Contrecoup Injury
- Located opposite to the site of impact
- Requires the head to be free to move (unless bony irregularity mechanism)
- More prominent in falls and traffic injuries - moving head decelerating suddenly on hitting a hard surface
- Due to sudden deceleration causing linear and (more harmful) rotational strains on the brain
- Most frequent sites: temporal poles, frontal poles, orbital surfaces of frontal lobes
- Skull fracture is NOT required - can occur even without fracture
- May occur with no coup damage at all - only contrecoup
- Contrecoup injuries are rare before age 3 years (brain not fully developed, less inertia)
- Severity may be enough to cause blood-filled cavitations in deep cortex and white matter (especially frontal lobes and temporal pole tips)
Intermediate Coup (Contusion)
- Located neither at nor fully opposite the point of impact
- Between coup and contrecoup positions
- Usually occurs when a moving head impacts at the vertex
- Brainstem contusions are a classic example
- Can mimic spontaneous intracerebral haemorrhage arising in deep cerebral parenchyma
8. FORENSIC SIGNIFICANCE (KEY MEDICO-LEGAL POINTS)
| Observation at Autopsy | Inference |
|---|---|
| Large coup + small contrecoup | Moving object struck a stationary head (assault - blow from a weapon) |
| Small coup + large contrecoup | Moving head hit a stationary surface (fall) |
| Only contrecoup, no coup | Still consistent with a fall or a blow |
| A line connecting coup + contrecoup centers | Indicates the direction of impact relative to the head |
| No skull fracture despite coup + contrecoup | Fracture is NOT required for coup-contrecoup injury |
| Frontal lobe contrecoup after occipital impact | Head was free to move at the time of injury |
| No occipital contrecoup despite frontal blow | Consistent with the rarity of frontal blow → occipital contrecoup rule |
| Bilateral frontal contrecoup | Fall on the occiput (symmetric fall backwards) |
| Temporal contrecoup against falx | Impact may have been ipsilateral (temporal/lateral), not contralateral |
| Black eyes without facial injury | Contrecoup blood tracking into orbit from frontal lobe haemorrhage |
9. CONTRECOUP IN OTHER ORGANS
Contrecoup injuries are not limited to the brain. They also occur in:
- Skull (fracture at a distance from impact)
- Liver (right lobe contrecoup in left-sided impact)
- Heart (myocardial contusion)
- Cervical spine (whiplash mechanism - ligamentous injuries at C5-C6 despite impact elsewhere)
- Spleen
10. PATHOLOGICAL APPEARANCE
Gross:
- Contusions appear as wedge-shaped areas of haemorrhagic necrosis on the cortical surface, with the base toward the surface and apex toward white matter
- At the crests of gyri
- Old contusions appear as shrunken, yellowish-brown areas known as "plaque jaunes" (yellow plaques)
Microscopic:
- Early: haemorrhage + axonal swelling + pyknotic neurons
- Later: reactive gliosis + haemosiderin deposits
- Inflammatory reaction (distinguishes antemortem from postmortem contusion)
11. COMPARISON TABLE
| Feature | Coup Injury | Contrecoup Injury |
|---|---|---|
| Location | At site of impact | Opposite to site of impact |
| French meaning | coup = blow | contre = opposite; coup = blow |
| Head position | Fixed or moving | Must be free to move (usually) |
| Mechanism | Direct impact force | Deceleration + inertia + rotation |
| Typical scenario | Moving weapon hits fixed head | Moving head hits fixed surface (fall) |
| Injury size | Larger with direct blows | Larger with falls/deceleration |
| Skull fracture | Usually present | Not required |
| Common sites | Under impact site | Frontal poles, temporal poles, orbital surface |
| Age restriction | Any age | Rare before 3 years |
| Associated finding | Depressed skull fracture possible | May cause "black eyes" from orbital seepage |
| Medico-legal use | Supports assault/blow | Supports fall; can exonerate accused |
12. HIGH-YIELD EXAM POINTS
| Question | Answer |
|---|---|
| Coup injury = ? | Injury at site of impact |
| Contrecoup injury = ? | Injury opposite to site of impact |
| Contrecoup requires? | Head to be free to move |
| Most common site of contrecoup injury | Frontal poles (from fall on occiput) |
| Most accepted theory | Holbourn's shear strain theory |
| Fall on back of head → contrecoup where? | Frontal lobes (subfrontal + temporal poles) |
| Fall on occiput - bilateral contrecoup? | Yes - bilateral frontal lobes |
| Frontal blow → occipital contrecoup? | Virtually never |
| Fracture required for contrecoup? | No |
| Contrecoup rare below age? | 3 years |
| Large coup + small contrecoup → | Moving weapon/blow on fixed head (assault) |
| Small coup + large contrecoup → | Fall (moving head, fixed surface) |
| Intermediate coup → | Moving head hitting vertex; brainstem contusions |
| "Black eyes" without facial trauma | Contrecoup frontal haemorrhage tracking into orbit |
| Theory involving CSF pressure | Gaggio's pressure gradient (cavitation) theory |
| Rawling's theory involves | Bony irregularities (cribriform plate, orbital plate, sphenoid) |
| "Line between coup and contrecoup" tells you | Direction of impact |
| Old contusions are called | Plaque jaunes (yellow plaques) |
Sources: P C Dikshit Textbook of Forensic Medicine and Toxicology (p. 205); The Essentials of Forensic Medicine and Toxicology, 36th ed. 2026 (pp. 251-252); Parikh's Textbook of Medical Jurisprudence, Forensic Medicine and Toxicology (pp. 327-328); Robbins Pathology
Defense of medical negligence
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from three authoritative forensic medicine textbooks. Let me compile the detailed note.
Defense of Medical Negligence - Comprehensive MBBS Notes
Sources: P C Dikshit Textbook of Forensic Medicine and Toxicology; The Essentials of Forensic Medicine and Toxicology (36th ed., 2026); Parikh's Textbook of Medical Jurisprudence, Forensic Medicine and Toxicology
1. DEFINITION OF MEDICAL NEGLIGENCE (Context)
Before understanding the defenses, it is essential to recall what must be proved for negligence to be established.
Negligence was defined by Justice Baron Alderson (1856) as:
"The omission to do something which a reasonable man could do, or doing something which a prudent and reasonable man could not do."
Lord Wright (1934) laid down 4 elements - all four must be present:
- A duty was owed to the patient
- Breach of that duty (by omission or commission)
- Direct causation - the breach caused harm
- Damage resulted
Professional Negligence = "Want of reasonable care and skill, or wilful negligence on the part of the medical practitioner while treating a patient resulting in bodily injury, ill health or death."
Key: If ANY of the four elements is absent, the doctor is NOT negligent. Each defense below attacks one or more of these elements.
2. DEFENSES AVAILABLE IN CASES OF MEDICAL NEGLIGENCE
The recognized defenses are:
DEFENSES AGAINST MEDICAL NEGLIGENCE
│
├── 1. No duty owed to the plaintiff
├── 2. Duty discharged according to prevailing standards
├── 3. Therapeutic misadventure
├── 4. Error of judgment
├── 5. Contributory negligence
├── 6. Res judicata
└── 7. Limitation (period of limitation expired)
DEFENSE 1: NO DUTY OWED TO THE PLAINTIFF
Principle: If no doctor-patient relationship was established, there is no duty of care, and therefore no negligence.
A duty of care arises when:
- The doctor accepts a patient for treatment
- The doctor voluntarily undertakes to treat someone
- The patient relies on the doctor's skill
Application:
- If a doctor is merely present as a bystander and is asked for advice informally, a duty may not have been formally established
- A doctor driving past an accident scene does not automatically owe a legal duty (though ethically compelled)
- However, once a doctor begins to treat, duty attaches immediately
Note: The following are NOT good defenses:
- "There was no contractual relationship between the doctor and patient" - the duty exists in law independent of contract
- "Service was rendered free of charge" - gratuitous service does not exempt from negligence
- "The medical man had no bad motive" - negligence does not require bad intent; it is objective
DEFENSE 2: DUTY DISCHARGED ACCORDING TO PREVAILING STANDARDS
Principle: If the doctor acted in accordance with general accepted practice of reasonable medical professionals in the relevant field, there is no breach of duty.
The Bolam Test (most important legal standard):
A doctor is not negligent if he acts in accordance with general approved/accepted practice - i.e., the practice of a responsible body of competent professionals in that field.
Key points:
- The court will rely upon evidence of competent practitioners in the relevant field
- "Approved practice" is the criterion for reasonable care
- A doctor is not negligent if he acts in accordance with what a reasonable body of professionals in his field would do
- However, the court pronounces a practice negligent if there are inherent defects in it
- "It is not enough to repute negligence by merely saying that he did what everybody does" - a risky practice may still be held negligent even if widely followed
- A practice that "no professional man of ordinary skill would adopt" cannot be defended
Deviation from normal practice:
- A practitioner may deviate from standard practice only if:
- He is free to exercise his own judgment and discretion
- The new procedure was done with the consent of the patient
- It was done for the benefit of the patient
- Success is the best justification for deviation
The Supreme Court of India Guidelines (11 points on medical negligence adjudication):
- Negligence = breach of duty or an act which a prudent and reasonable man will not do
- Negligence must be culpable or gross - not merely an error of judgment
- Doctor must bring reasonable degree of skill - neither the highest nor the lowest
- A doctor is liable only where conduct fell below the standard of a reasonably competent practitioner
- Difference of opinion cannot be cited as negligence
- Taking a higher element of risk to save a gravely ill patient which did not yield desired results - may not amount to negligence
- Choosing one course of action from among available alternatives does not constitute negligence if the chosen action was acceptable to the profession
- It would not be conducive to the efficiency of the medical profession if no doctor could administer medicine without a "halter round his neck"
- Duty not to harass or humiliate medical professionals unnecessarily
- Doctors must be protected from complaints used as tools to pressurize them or extract unwarranted compensation
- Doctors are entitled to protection so long as they perform duties with reasonable skill and competence
DEFENSE 3: THERAPEUTIC MISADVENTURE
Definition: A misadventure is a mischance, accident, or unexpected disaster occurring during treatment, diagnosis, or experiment that was not due to negligence.
Three types of misadventure:
- Therapeutic - when treatment is being given
- Diagnostic - where diagnosis only is the objective
- Experimental - where the patient has agreed to serve as a subject in an experimental study
Principle: Unexpected complications or adverse outcomes that occur despite proper care and skill are not negligence - they are misadventures.
Key legal points:
- A physician is not liable for injuries resulting from adverse drug reactions, unless some negligence on his part contributed to causing the injury
- However, ignorance of the possibility of a known reaction, or continuation of prescribing a drug with a known adverse reaction, amounts to negligence
- A negative drug sensitivity history and a negative sensitivity test do not rule out the rare possibility of an anaphylactoid reaction
Examples where misadventure is a valid defense:
- Patient develops anaphylaxis to penicillin despite sensitivity test being negative (if history was taken and test was done)
- Unexpected intraoperative bleeding from an anatomical variant
- Death under anaesthesia despite all precautions being followed
- A rare complication that occurs despite standard management
Doctor's obligation in cases of misadventure:
- Must have informed the patient of known and anticipated risks (informed consent)
- Must have chosen the least risky drug when alternatives were available
- Must not have ignored warning signs after the adverse event began
- Must have been equipped with life-saving drugs when administering potentially sensitizing agents
DEFENSE 4: ERROR OF JUDGMENT
Principle: An honest error of clinical judgment made by a competent doctor, exercising reasonable care, is not negligence.
Legal basis:
- Lord Denning in Hatcher v Black & Others (1954): The doctor's professional reputation is as dear to him as his body, and an action for negligence could wound his reputation as severely as a dagger to his body
- A doctor who makes a wrong diagnosis but did so after proper history, examination and investigations - within the limits of ordinary professional competence - is not negligent
- The difference between negligence and error of judgment is the exercise of reasonable care
Conditions for error of judgment to serve as defense:
- The doctor must have exercised reasonable care and skill in reaching the decision
- The decision must have been within the range of acceptable professional opinion
- The doctor must have used all reliable and relevant information (history, physical examination, investigations)
- The error must NOT result from reliance on inadequate data or forming unsupported conclusions
Examples:
- Wrong diagnosis of appendicitis which turns out to be ovarian cyst, if proper examination was done
- Missing a rare presentation of a common disease
- Choosing a drug that later proves less effective than alternatives
What does NOT qualify as error of judgment (still amounts to negligence):
- Failure to use standard diagnostic equipment (e.g., ophthalmoscope to check for raised ICP)
- Failure to refer to a specialist when specialist input was clearly needed
- Relying on inadequate data to reach a diagnosis
DEFENSE 5: CONTRIBUTORY NEGLIGENCE
Definition: Contributory negligence is the absence of reasonable care on the part of the patient or his attendant that combines with the negligent action of the doctor, resulting in damage - damage that would not have occurred without the patient's own fault.
Principle: When the patient's own negligence has contributed to the harm, the doctor's liability is reduced or extinguished.
Important rules:
- Contributory negligence is a good defense in civil cases only
- It is NOT a defense in criminal negligence cases
- The burden of proving contributory negligence rests entirely on the doctor
- The doctor cannot plead contributory negligence unless he had warned the patient of the risk beforehand
- If the doctor and patient are negligent simultaneously → doctor can take a good defense
Common examples of patient contributory negligence:
- Not providing proper/correct history to the doctor (e.g., suppressing pregnancy status)
- Failure to follow prescribed treatment (skipping medicines, dietary non-compliance)
- Refusal to take up suggested advice (e.g., refusing recommended investigations)
- Leaving the hospital against doctor's advice (LAMA)
- Failure to seek further medical treatment when symptoms persist
- Sudden movement during a procedure (e.g., moving arm during injection, causing needle breakage)
Case examples:
- Doctor warned patient to keep arm steady during injection; patient moved suddenly - needle broke; court dismissed patient's claim (contributory negligence proven)
- Gynaecologist failed to test for pregnancy; patient suppressed history of intercourse - court did not award damages to the patient because her suppression of history contributed to the wrong diagnosis
Limitations of Contributory Negligence:
-
Last Clear Chance Doctrine: If the doctor discovered the patient's injury while there was still time to avoid it but failed to do so, the patient may still recover damages - despite the patient's own negligence
-
Avoidable Consequences Rule: If the doctor was found negligent first, and the patient's negligence occurred only after the doctor's negligence, the patient is NOT guilty of contributory negligence - the doctor bears full responsibility
DEFENSE 6: RES JUDICATA
Definition: Res judicata (Latin: "the matter has been decided") = once a case has been decided by a court, it cannot be taken to another court on the same issue between the same parties.
Section reference: Section 337, BNSS (Bharatiya Nagarik Suraksha Sanhita)
Principle: If a question of negligence against a doctor has already been decided by a court in a dispute between the doctor and the patient, the patient cannot contest the same question in another proceeding between himself and the doctor on the same set of facts in a different court.
Application:
- Protects doctors from being dragged to multiple courts for the same alleged act of negligence
- Appeal is the only remedy available to the aggrieved party
- The doctor can plead res judicata if a second suit is filed on the same facts as an already-decided case
DEFENSE 7: LIMITATION (Period of Limitation)
Principle: A suit for damages for negligence against a doctor must be filed within the prescribed time period. A suit filed beyond this period is dismissed.
Time limits:
| Type of Suit | Limitation Period |
|---|---|
| Suit for damages for negligence | 2 years from the date of alleged negligence |
| Suit based on breach of duty under a specific contract (doctor-patient contract) | 3 years from the date of breach |
Application:
- If the patient files suit after 2 years of the alleged negligent act - the suit will be dismissed as being time-barred
- This protects doctors from stale claims where evidence has become uncertain and memories have faded
- The limitation period begins from the date of the alleged negligence (not from the date when the patient discovers the harm in all cases)
3. THINGS THAT ARE NOT GOOD DEFENSES
The following statements/facts do NOT constitute a valid defense:
| Not a Good Defense | Reason |
|---|---|
| "There was no contractual relationship between doctor and patient" | Duty of care arises in law independent of formal contract |
| "Service was rendered free of charge" | Gratuitous services are still subject to duty of care |
| "The medical man had no bad motive" | Negligence is objective - bad intent is not required |
| "The patient was going to die anyway" | This does not negate the breach of duty or the causation |
| "I followed the same practice as all my colleagues" | A widely followed risky practice can still be held negligent if it has inherent defects |
4. CIVIL vs CRIMINAL NEGLIGENCE - DEFENSE DIFFERENCES
| Feature | Civil Negligence | Criminal Negligence |
|---|---|---|
| Nature of offense | Simple absence of care and skill | Gross negligence, inattention or lack of competency |
| Standard | Compared to generally accepted professional standard | Not compared to any single test |
| Consent as defense | Good defense - cannot recover damages | NOT a defense - can still be prosecuted |
| Contributory negligence | Valid defense (partial or full) | NOT a valid defense |
| Evidence threshold | Strong evidence sufficient | Guilt proved beyond reasonable doubt |
| Punishment | Damages/compensation to be paid | Imprisonment |
| Court | Civil court / Consumer Forum | Criminal court |
5. PRECAUTIONS TO AVOID NEGLIGENCE (Prevention = Best Defense)
The best defense is to have followed these precautions:
The 10 R's (Essentials of FMT):
- Rapport - maintain healthy communication with patient, family, and healthcare team
- Rationale - use all reliable, relevant information for diagnosis and treatment; document diagnostic rationale
- Records - maintain complete, accurate, legible, timely records ("A bad result with bad records = liability")
- Remarks - do not reprimand patient/family; do not criticise colleagues in patient's presence
- Recipe - prescribe only with appropriate indication; warn of side-effects; be aware of contraindications
- Res ipsa Loquitur - if untoward result occurs, admit the problem rather than deny it
- Respect - treat the patient as the physician would wish to be treated himself
- Results - obtain informed consent; give close attention if a bad result occurs
- Risks - inform patient of all anticipated risks (serious risks even if rare; lesser risks of greater probability)
- Review - routinely review cases of morbidity and mortality; review medical malpractice cases
Additional specific precautions:
- Never guarantee a cure
- Obtain informed written consent before surgery and anaesthesia with detailed explanation of risks
- Confirm diagnosis with proper investigations
- Perform sensitivity tests before administering drugs known to cause hypersensitivity (penicillin, streptomycin, antivenins)
- Never criticise a colleague's professional ability (this weakens your own position and invites litigation)
- Do not leave a patient unattended during labour
- Never carry out procedures solely on telephonic consultation
- Arrange a qualified substitute when absent from practice
6. MEDICAL DEFENCE ORGANISATIONS
- The Medical Defence Union (MDU) and Medical Protection Society (MPS) are organizations that provide legal and financial support to doctors facing negligence claims
- When any suggestion of negligence or malpractice is made against an insured doctor, he should refer the matter at once to his medical defence society
- In India, the Medical Indemnity Insurance provides similar protection
7. HIGH-YIELD SUMMARY TABLE
| Question | Answer |
|---|---|
| How many defenses against medical negligence? | 7 |
| Contributory negligence valid in? | Civil negligence only - NOT criminal |
| Who bears the burden of proving contributory negligence? | The doctor |
| Can doctor plead contributory negligence without warning patient? | No |
| Limitation period for negligence suit | 2 years (3 years for contract breach) |
| Res judicata means? | Case already decided - cannot be re-filed in another court |
| Is "no bad motive" a good defense? | No |
| Is "free service" a good defense? | No |
| Is "no contract" a good defense? | No |
| Error of judgment defense requires? | Reasonable care and skill exercised |
| Misadventure defense requires? | Proper care taken; adverse outcome unforeseeable |
| Supreme Court standard for negligence | Reasonably competent practitioner standard |
| Best legal test for "standard of care" | Bolam test |
| "Last clear chance doctrine" limits which defense? | Contributory negligence |
| "Avoidable consequences rule" limits which defense? | Contributory negligence |
| Medical negligence first defined by? | Justice Baron Alderson (1856) |
| Lord Wright's 4 elements of negligence | Duty, Breach, Direct causation, Damage |
Sources: P C Dikshit Textbook of Forensic Medicine and Toxicology (pp. 29-35); The Essentials of Forensic Medicine and Toxicology, 36th edition, 2026 (pp. 59-60); Parikh's Textbook of Medical Jurisprudence, Forensic Medicine and Toxicology (pp. 61-68)
This is a shared conversation. Sign in to Orris to start your own chat.