Hypervascular uterus causes PID treatment
Reading File
Finding Sources
Finding Sources
Searching PubMed
"pelvic inflammatory disease" AND treatment
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here is a comprehensive overview covering the hypervascular uterus sign in PID and its treatment.
Hypervascular Uterus in PID
What Does "Hypervascular Uterus" Mean in This Context?
A hypervascular uterus refers to increased uterine blood flow detected on color Doppler ultrasound (transvaginal ultrasound, TVUS). In the setting of PID, this reflects active inflammation/hyperemia of the myometrium and endometrium, and is one of the sonographic markers of endometritis/PID.
On TVUS, early PID findings in the uterus include:
- Normal or slightly enlarged uterus with ill-defined margins (pelvic exudate)
- Hypoechoic myometrium with poorly defined areas of decreased echogenicity (edema/inflammation)
- Thickened endometrium (≥14 mm), with variable echogenicity and a poorly defined endometrial/myometrial interface
- Fluid within the endometrial cavity
- On color Doppler: increased vascularity (hypervascularity) of the uterine wall — a sign of active inflammation
As disease progresses, the findings extend to the adnexa: thickened fallopian tubes, pyosalpinx (echogenic fluid/debris in tube), hydrosalpinx, and tubo-ovarian abscess (TOA).
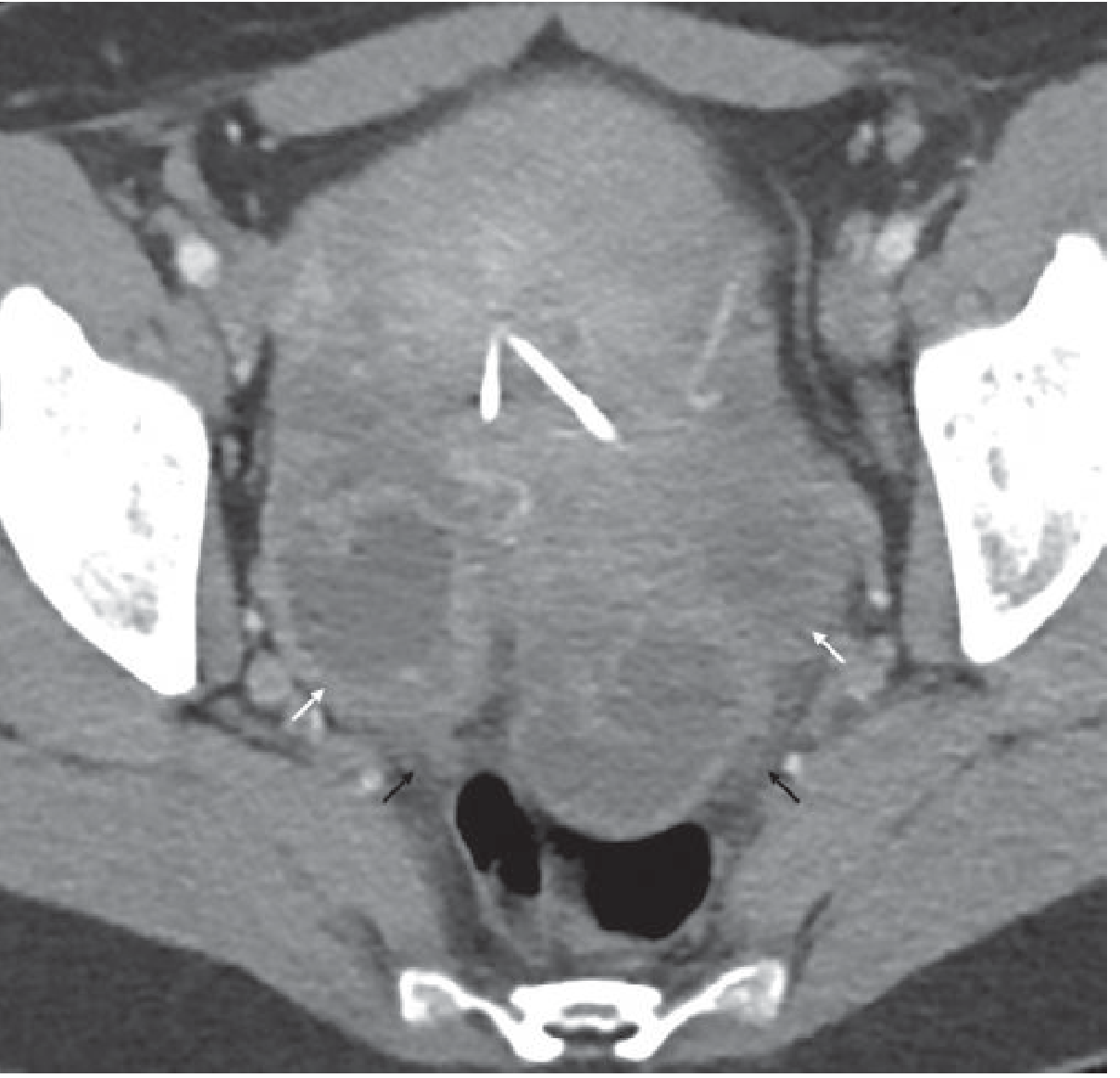
On CT, abnormal endometrial enhancement and fluid within the endometrial cavity indicate endometritis, and a bulky, hypervascularly-enhancing uterus suggests active PID.
Grainger & Allison's Diagnostic Radiology, p. 900
PID: Diagnosis
The CDC criteria (2021 guidelines) recommend initiating empirical treatment in sexually active women at risk for PID if they have pelvic/lower abdominal pain AND at least one of:
- Cervical motion tenderness
- Uterine tenderness
- Adnexal tenderness
A hypervascular uterus on Doppler TVUS supports the diagnosis in equivocal cases, particularly when combined with the above clinical criteria.
Harrison's Principles of Internal Medicine 22E, p. 1148
PID: Treatment
Treatment must provide broad-spectrum coverage for N. gonorrhoeae, C. trachomatis, M. genitalium, and anaerobes (especially in BV-associated cases).
Outpatient (Ambulatory) Regimen — CDC 2021
| Drug | Dose |
|---|---|
| Ceftriaxone | 500 mg IM × 1 dose |
| Doxycycline | 100 mg PO twice daily × 14 days |
| Metronidazole | 500 mg PO twice daily × 14 days |
Metronidazole is recommended particularly when BV or trichomoniasis is present. In a randomized trial, adding metronidazole to ceftriaxone + doxycycline reduced endometrial anaerobes, M. genitalium, and pelvic tenderness.
Parenteral (Inpatient) Regimen — CDC 2021
Continue IV therapy until 48 h after clinical improvement, then switch to oral.
Regimen A:
- Cefotetan 2 g IV q12h or Cefoxitin 2 g IV q6h
- + Doxycycline 100 mg IV or PO q12h
Regimen B:
- Clindamycin 900 mg IV q8h
- + Gentamicin (loading dose 2 mg/kg IV/IM, then 1.5 mg/kg q8h)
Harrison's Principles of Internal Medicine 22E, p. 1149 (Table 141-6)
Indications for Hospitalization
Consider inpatient management when:
- Diagnosis is uncertain and surgical emergencies (appendicitis, ectopic pregnancy) cannot be excluded
- Patient is pregnant
- Pelvic abscess (TOA) is suspected
- Severe illness, nausea/vomiting precludes oral therapy
- Patient has HIV infection
- Patient unable to follow/tolerate outpatient regimen
- Failure to respond to outpatient therapy
Harrison's Principles of Internal Medicine 22E, p. 1149
Cephalosporin Intolerance
Adequate oral coverage for N. gonorrhoeae is not available outside parenteral cephalosporins. For serious cephalosporin intolerance (if penicillins are tolerated): amoxicillin/clavulanic acid + doxycycline is an option.
Percutaneous Drainage
For TOA or pelvic collections that fail antibiotic therapy, US- or CT-guided percutaneous drainage is recommended.
Key Pathogens
| Pathogen | Role |
|---|---|
| Neisseria gonorrhoeae | Primary cause, esp. in high-prevalence settings |
| Chlamydia trachomatis | Common; subclinical endometritis common |
| Mycoplasma genitalium | Associated with endometritis and salpingitis |
| Anaerobes (Prevotella spp., peptostreptococci) | Found in ¼–⅓ of cases (peritoneal/tubal fluid) |
| E. coli, H. influenzae, Group B Strep | Facultative organisms, variable contribution |
Harrison's Principles of Internal Medicine 22E, p. 1148
Summary: A hypervascular uterus on color Doppler TVUS is a sonographic correlate of endometritis within the PID spectrum. Its presence alongside clinical criteria supports initiating empirical antibiotic therapy. The cornerstone of outpatient treatment is ceftriaxone + doxycycline + metronidazole for 14 days; inpatient therapy uses cefotetan/cefoxitin + doxycycline or clindamycin + gentamicin per CDC 2021 guidelines.
This is a shared conversation. Sign in to Orris to start your own chat.