Generate the anatomy and physiology of the 11 human body system l
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have strong foundational material. Let me compile the comprehensive answer on all 11 human body systems from the medical library and my knowledge base.
Anatomy and Physiology of the 11 Human Body Systems
The human body is organized into 11 interacting organ systems. Each system has distinct structural components (anatomy) and specific functions (physiology). All systems are interdependent - the life of the human body requires not only that individual organ systems do their jobs but also that they work hand in hand, sharing information through molecular messengers. - Medical Physiology
1. Integumentary System
Anatomy
- Layers: Epidermis (outer, avascular, 4-5 sublayers: stratum basale, spinosum, granulosum, lucidum, corneum), Dermis (dense irregular connective tissue with blood vessels, nerves, hair follicles, sweat glands), Hypodermis/subcutis (adipose and loose connective tissue)
- Accessory structures: Hair follicles, sebaceous glands, eccrine and apocrine sweat glands, nails, sensory receptors (Meissner's, Pacinian, Merkel, Ruffini corpuscles)
Physiology
The skin serves as the body's primary barrier, protecting against mechanical, chemical, and thermal trauma as well as pathogens. - Color Atlas of Human Anatomy Vol. 2
Key functions:
- Protection: Physical and chemical barrier against the external environment
- Thermoregulation: Sweat evaporation cools the body; cutaneous vasoconstriction/dilation adjusts heat loss
- Sensation: Contains receptors for pain, touch, pressure, vibration, and temperature
- Vitamin D synthesis: UV exposure converts 7-dehydrocholesterol to cholecalciferol (Vitamin D3) in the epidermis
- Immunity: Langerhans cells (dendritic cells) in the epidermis are antigen-presenting cells
- Water balance: Prevents excessive transepidermal water loss
2. Skeletal System
Anatomy
- 206 bones in the adult skeleton, divided into axial skeleton (80 bones: skull, vertebral column, rib cage, sternum) and appendicular skeleton (126 bones: pectoral girdles, upper limbs, pelvic girdle, lower limbs)
- Bone tissue types: Compact (cortical) bone - dense, outer layer; Spongy (cancellous/trabecular) bone - inner honeycomb lattice
- Bone cells: Osteoblasts (bone formation), osteocytes (bone maintenance), osteoclasts (bone resorption), osteogenic/periosteal cells
- Joints: Fibrous (sutures, syndesmoses), cartilaginous (synchondroses, symphyses), synovial (freely movable - ball and socket, hinge, pivot, condyloid, saddle, gliding)
- Cartilage: Hyaline, fibrocartilage, elastic
Physiology
- Support and framework: Provides rigid structure maintaining body shape
- Protection: Skull protects brain; vertebral column protects spinal cord; rib cage protects heart and lungs
- Movement: Serves as levers for muscle action at joints
- Hematopoiesis: Red bone marrow (in flat bones and epiphyses of long bones) produces red blood cells, white blood cells, and platelets
- Mineral storage: Stores and releases calcium (99% of body calcium) and phosphate; regulated by PTH (parathyroid hormone), calcitonin, and calcitriol
- Fat storage: Yellow marrow stores lipids as energy reserve
- Bone remodeling: Continuous process balanced between osteoblast deposition and osteoclast resorption, regulated by mechanical stress (Wolff's Law)
3. Muscular System
Anatomy
- Three muscle types:
- Skeletal muscle: Striated, voluntary; arranged in fiber bundles (fascicles) wrapped by perimysium, surrounded by epimysium
- Cardiac muscle: Striated, involuntary; cells (cardiomyocytes) connected by intercalated discs with gap junctions
- Smooth muscle: Non-striated, involuntary; found in walls of hollow organs, blood vessels, airways
- Gross anatomy: ~600 named skeletal muscles with origins (fixed attachment) and insertions (moving attachment)
- Connective tissue: Endomysium (individual fibers), perimysium (fascicles), epimysium (whole muscle), tendons (muscle to bone), aponeuroses (flat tendons)
- Microstructure: Sarcomere is the functional unit - composed of thick (myosin) and thin (actin) filaments, bounded by Z-lines
Physiology
- Sliding filament mechanism: Contraction occurs when myosin heads bind actin, form cross-bridges, and pull actin toward the center of the sarcomere (power stroke), requiring ATP and Ca²⁺
- Neuromuscular junction: Motor neuron releases acetylcholine (ACh) into the synaptic cleft → ACh binds nicotinic receptors on muscle → action potential → SR releases Ca²⁺ → troponin-tropomyosin shift exposes actin binding sites
- Muscle fiber types: Type I (slow-twitch, aerobic, fatigue-resistant), Type IIa (fast-twitch, oxidative-glycolytic), Type IIx (fast-twitch, glycolytic, fatigable)
- Energy sources: Creatine phosphate (immediate), anaerobic glycolysis (short-term), aerobic oxidative phosphorylation (long-term)
- Cardiac autorhythmicity: SA node pacemaker initiates each beat; intercalated disc gap junctions allow electrical syncytium
- Smooth muscle: Regulated by autonomic nerves, hormones, and local factors; sustained tonic contractions possible due to latch-bridge mechanism
4. Nervous System
Anatomy
The human brain is the most complex tissue in the body, mediating behavior from simple movements to learning, memory, and consciousness. - Medical Physiology
- Central Nervous System (CNS): Brain (cerebrum, cerebellum, brainstem) + Spinal cord
- Cerebrum: Two hemispheres with 4 lobes each (frontal, parietal, temporal, occipital); gray matter (cortex) + white matter
- Cerebellum: Coordinates movement, balance, proprioception
- Brainstem: Midbrain, pons, medulla oblongata - controls vital autonomic functions
- Spinal cord: 31 segments; butterfly-shaped gray matter (dorsal sensory, ventral motor horns) surrounded by white matter tracts
- Peripheral Nervous System (PNS): 12 pairs cranial nerves + 31 pairs spinal nerves
- Somatic: Voluntary sensory and motor
- Autonomic: Sympathetic (thoracolumbar), Parasympathetic (craniosacral), Enteric (GI tract)
- Cells: Neurons (cell body/soma, axon, dendrites) and neuroglia (astrocytes, oligodendrocytes, microglia, ependymal cells in CNS; Schwann cells, satellite cells in PNS)
- Meninges: Dura mater, arachnoid mater, pia mater
- Blood-Brain Barrier (BBB): Tight junctions between cerebral endothelial cells create a highly regulated environment for CNS neurons - Medical Physiology
Physiology
- Resting membrane potential: ~-70 mV in neurons; maintained by Na⁺/K⁺ ATPase and differential permeability
- Action potential: Depolarization (Na⁺ influx) → repolarization (K⁺ efflux) → hyperpolarization; all-or-none, propagated along axon
- Synaptic transmission: Neurotransmitters (glutamate, GABA, dopamine, serotonin, acetylcholine, norepinephrine) released into synaptic cleft, bind postsynaptic receptors
- Reflex arcs: Sensory receptor → afferent neuron → interneuron → efferent neuron → effector
- Autonomic regulation: Sympathetic ("fight or flight") - epinephrine/norepinephrine; Parasympathetic ("rest and digest") - acetylcholine; Enteric - regulates GI motility
- Higher functions: Cerebral cortex mediates consciousness, cognition, language, emotion, planning, and voluntary movement
5. Endocrine System
Anatomy
The endocrine system consists of numerous specialized endocrine glands and glandular cells occurring individually or in groups throughout the organism, whose products (hormones) are released into the bloodstream or lymph. - Color Atlas of Human Anatomy Vol. 2
- Major glands: Hypothalamus, pituitary gland (anterior + posterior), thyroid, parathyroid (4 glands), adrenal glands (cortex + medulla), pancreas (islets of Langerhans), gonads (ovaries/testes), pineal gland, thymus
- Diffuse endocrine cells: GI tract (enteroendocrine cells), kidney (juxtaglomerular cells), heart (atrial natriuretic cells), adipose tissue (adipokine-secreting cells)
- Hypothalamo-pituitary axis: Hypothalamic nuclei secrete releasing/inhibiting hormones into portal circulation → anterior pituitary responds by secreting tropic hormones
Physiology
- Hormone classes: Peptides/proteins (insulin, GH), steroids (cortisol, estrogen, testosterone), amines (thyroid hormones, catecholamines)
- Mechanisms of action: Lipid-soluble hormones (steroids, thyroid) - cross membrane, bind nuclear receptors, alter gene expression; Water-soluble hormones (peptides, catecholamines) - bind cell surface receptors, activate second messengers (cAMP, IP3, DAG)
- Feedback loops: Negative feedback predominates (e.g., high cortisol suppresses CRH and ACTH)
- Key axes: HPA (stress), HPT (metabolism), HPG (reproduction), GH-IGF-1 (growth)
- Thyroid hormones: Act synergistically with growth hormone; increase BMR, heat production, and oxygen consumption; alter cardiovascular and respiratory systems - Costanzo Physiology
- Pancreatic regulation: Insulin (beta cells) - lowers blood glucose; Glucagon (alpha cells) - raises blood glucose
- Adrenal cortex: Mineralocorticoids (aldosterone - Na⁺ retention), Glucocorticoids (cortisol - stress, metabolism, immunity), Androgens (DHEA)
- Adrenal medulla: Epinephrine and norepinephrine - sympathetic stress response
6. Cardiovascular System
Anatomy
The cardiovascular system includes the heart, blood vessels, and lymphatic vessels. - Histology: A Text and Atlas
- Heart: 4 chambers (right atrium, right ventricle, left atrium, left ventricle); 4 valves (tricuspid, pulmonary, mitral/bicuspid, aortic); layers: endocardium, myocardium, pericardium
- Conduction system: SA node (pacemaker, 60-100 bpm) → AV node → Bundle of His → Left/Right bundle branches → Purkinje fibers
- Blood vessels:
- Arteries: Thick-walled, muscular/elastic, carry blood away from heart
- Arterioles: Primary resistance vessels; regulate blood flow distribution
- Capillaries: Single-cell-thick walls; site of gas/nutrient exchange
- Venules and veins: Low-pressure, thin-walled, capacitance vessels; veins have valves
- Circulations: Pulmonary (right heart → lungs → left heart) and Systemic (left heart → body → right heart)
- Coronary arteries: RCA (right coronary), LAD (left anterior descending), LCx (left circumflex) supply myocardium
Physiology
- Cardiac cycle: Systole (ventricular contraction, ejection) and diastole (ventricular relaxation, filling); duration ~0.8 sec at rest
- Cardiac output (CO): CO = Heart Rate × Stroke Volume; normal ~5 L/min at rest
- Regulation: Frank-Starling law (increased preload → increased stroke volume); Contractility (inotropy); Afterload (resistance against which heart pumps)
- Blood pressure: Systolic (~120 mmHg) / Diastolic (~80 mmHg); Mean arterial pressure = diastolic + 1/3 pulse pressure
- Baroreceptor reflex: Carotid sinus and aortic arch baroreceptors detect BP changes → medullary cardiovascular center adjusts HR and vascular tone
- Capillary exchange: Starling forces govern fluid movement - net filtration pressure = (capillary oncotic P + interstitial hydrostatic P) - (capillary hydrostatic P + interstitial oncotic P)
- Hemostasis: Vascular spasm → platelet plug (primary hemostasis) → coagulation cascade (secondary hemostasis) → clot dissolution (fibrinolysis)
7. Respiratory System
Anatomy
The respiratory system is divided into the gas-exchanging surface of the lungs and the structures comprising the upper and lower airways. - Color Atlas of Human Anatomy Vol. 2
- Upper airway: Nasal cavity (turbinates, mucosal lining), nasopharynx, oropharynx, larynx (epiglottis, vocal cords, thyroid/cricoid cartilages)
- Lower airway: Trachea (C-shaped cartilage rings) → Primary bronchi → Secondary (lobar) bronchi → Tertiary (segmental) bronchi → Bronchioles → Terminal bronchioles → Respiratory bronchioles → Alveolar ducts → Alveoli
- Lungs: Right (3 lobes: upper, middle, lower) and Left (2 lobes: upper, lower with lingula); covered by visceral pleura; chest wall has parietal pleura
- Alveoli: ~300-500 million; lined by Type I pneumocytes (gas exchange, ~95% surface), Type II pneumocytes (surfactant production, ~5%), alveolar macrophages
- Respiratory muscles: Diaphragm (primary), external intercostals (inspiration); internal intercostals, abdominal muscles (forced expiration)
Physiology
- Mechanics of breathing: Inspiration - diaphragm contracts, thoracic volume increases, intrapleural pressure becomes more negative (-8 to -10 cmH₂O), alveolar pressure drops below atmospheric, air flows in; Expiration - passive elastic recoil
- Lung volumes: Tidal volume (TV, ~500 mL), Inspiratory Reserve Volume (IRV, ~3100 mL), Expiratory Reserve Volume (ERV, ~1200 mL), Residual Volume (RV, ~1200 mL); Total Lung Capacity = TV + IRV + ERV + RV (~6 L)
- Surfactant: Dipalmitoylphosphatidylcholine (DPPC) from Type II pneumocytes reduces alveolar surface tension, prevents collapse
- Gas exchange: Diffusion driven by partial pressure gradients: O₂ (alveoli P₀₂ ~100 mmHg → blood ~40 mmHg); CO₂ (blood ~45 mmHg → alveoli ~40 mmHg)
- Oxygen transport: 98.5% bound to hemoglobin (cooperative binding, sigmoid O₂-Hb dissociation curve); 1.5% dissolved; Bohr effect - acidosis/hypercapnia right-shifts curve (lower affinity, more O₂ release to tissues)
- CO₂ transport: 70% as bicarbonate (HCO₃⁻); 23% bound to hemoglobin (carbaminohemoglobin); 7% dissolved
- Ventilation-perfusion (V/Q) matching: Normal ratio ~0.8; mismatching is the most common cause of hypoxemia
- Control of breathing: Medullary respiratory center (pre-Bötzinger complex); central chemoreceptors (medulla, respond to CO₂/pH); peripheral chemoreceptors (carotid and aortic bodies, respond to O₂, CO₂, pH)
8. Digestive System
Anatomy
The alimentary system is divided into the part of the gastrointestinal tract contained in the head and the part beginning with the esophagus, including the liver and pancreas as large digestive glands. - Color Atlas of Human Anatomy Vol. 2
- GI tract (mouth to anus, ~9 meters): Oral cavity (teeth, tongue, salivary glands) → Pharynx → Esophagus → Stomach → Small intestine (duodenum, jejunum, ileum) → Large intestine (cecum, ascending/transverse/descending/sigmoid colon, rectum) → Anal canal
- Wall structure (4 layers): Mucosa (epithelium, lamina propria, muscularis mucosae), Submucosa (Meissner's plexus), Muscularis externa (inner circular + outer longitudinal smooth muscle, Auerbach's/myenteric plexus), Serosa/adventitia
- Accessory organs: Liver (largest gland, 4 lobes, hepatic lobules), gallbladder, pancreas (exocrine acini + endocrine islets), salivary glands (parotid, submandibular, sublingual)
- Surface area enhancement: Plicae circulares (folds), villi, microvilli (brush border) multiply small intestinal surface area ~200-fold
Physiology
- Digestion: Mechanical (chewing, churning, peristalsis) and chemical (enzymatic hydrolysis)
- Salivary amylase: Begins starch digestion in mouth
- Stomach: HCl (parietal cells, activated by gastrin, ACh, histamine) maintains pH 1-2; pepsinogen → pepsin breaks proteins; intrinsic factor (vitamin B12 absorption)
- Pancreatic enzymes: Amylase (starch), lipase (fat), proteases (trypsinogen, chymotrypsinogen, elastase) - neutralized by bicarbonate; released by CCK and secretin
- Bile: Produced in liver, stored in gallbladder, released by CCK; emulsifies fat for lipase action; contains bile salts (for micelle formation), cholesterol, phospholipids, bilirubin
- Absorption: Carbohydrates (monosaccharides via SGLT1/GLUT5), proteins (amino acids via Na⁺-dependent cotransport), fats (micelles → free fatty acids + monoglycerides → re-esterified into triglycerides → chylomicrons → lacteals), vitamins and minerals
- Motility: Peristalsis (propulsion), segmentation (mixing); regulated by ENS, vagal, hormonal, and local inputs
- Liver functions: Metabolism of carbohydrates, lipids, proteins; detoxification; bile production; clotting factor synthesis; glycogen storage; albumin synthesis
9. Urinary System
Anatomy
The urinary system is divided into the parts of the kidney responsible for urine formation and the urinary passages. - Color Atlas of Human Anatomy Vol. 2
- Kidneys: Paired, retroperitoneal; outer cortex (glomeruli, proximal/distal tubules), inner medulla (loops of Henle, collecting ducts, renal pyramids), renal pelvis
- Nephron (functional unit, ~1 million per kidney): Glomerulus (fenestrated capillaries + Bowman's capsule) → Proximal convoluted tubule (PCT) → Loop of Henle (descending thin, ascending thin, ascending thick limbs) → Distal convoluted tubule (DCT) → Collecting duct
- Blood supply: Renal artery → interlobar → arcuate → interlobular arteries → afferent arterioles → glomerular capillaries → efferent arterioles → peritubular capillaries/vasa recta
- Juxtaglomerular apparatus: JG cells (renin-producing), macula densa (Na⁺-sensing), extraglomerular mesangial cells
- Urinary passages: Ureters (peristaltic, urothelium-lined) → Bladder (detrusor muscle, trigone, urothelium, capacity ~500 mL) → Urethra
Physiology
- Filtration (GFR ~125 mL/min, ~180 L/day): Driven by glomerular hydrostatic pressure; filtered fluid = plasma minus large proteins
- Tubular reabsorption: PCT reabsorbs ~67% of filtered Na⁺, water, glucose (entirely), amino acids, HCO₃⁻, phosphate; Loop of Henle - NKCC2 in thick ascending limb reabsorbs NaCl without water → creates medullary osmotic gradient (300-1200 mOsm/kg); DCT - fine-tuning Na⁺/K⁺/H⁺ balance
- Tubular secretion: K⁺, H⁺, organic acids/bases, drugs
- Concentration/dilution: ADH (vasopressin) from posterior pituitary inserts aquaporin-2 channels in collecting duct → water reabsorption; no ADH → dilute urine
- RAAS: Renin (JG cells) → Angiotensin I → ACE → Angiotensin II → aldosterone (adrenal cortex) → Na⁺ retention, K⁺ excretion, BP elevation
- Acid-base balance: Kidneys regulate HCO₃⁻ reabsorption and H⁺ excretion; compensate respiratory acid-base disorders over days
- Erythropoietin (EPO): Kidney peritubular cells secrete EPO in response to hypoxia → stimulates RBC production in bone marrow
- Micturition: Detrusor contraction (parasympathetic, S2-S4) + internal urethral sphincter relaxation (inhibition of sympathetic); external sphincter voluntary (somatic)
10. Reproductive System
Anatomy
Male reproductive system: System consisting of the testes, epididymis, ductus deferens, seminal vesicles, penis, and accessory sex glands. - Color Atlas of Human Anatomy Vol. 2
- Testes: In scrotum (3-5°C below body temperature for spermatogenesis); seminiferous tubules (Sertoli cells support spermatogenesis, Leydig cells produce testosterone), rete testis
- Ductal system: Epididymis (sperm maturation, ~20 days) → Vas deferens → Ejaculatory duct → Urethra
- Accessory glands: Seminal vesicles (60% of semen, fructose, prostaglandins), Prostate (20-30%, citric acid, PSA, zinc), Bulbourethral glands (pre-ejaculatory alkaline fluid)
- Penis: Erectile tissue (corpora cavernosa x2 + corpus spongiosum surrounding urethra), glans, prepuce
Female reproductive system: System consisting of the female internal genitalia housed in the lesser pelvis and female external genitalia. - Color Atlas of Human Anatomy Vol. 2
- Ovaries: Cortex (follicles at various stages), medulla; produce ova and sex hormones
- Uterine tubes (Fallopian): Fimbriae (catch ovum) → infundibulum → ampulla (fertilization site) → isthmus → cornua
- Uterus: Perimetrium, myometrium (thick smooth muscle), endometrium (stratum functionalis + basalis); cervix opens into vagina
- Vagina: Fibromuscular canal; stratified squamous epithelium
- External genitalia (vulva): Labia majora, labia minora, clitoris, vestibule, Bartholin's glands
Physiology
Male:
- Spermatogenesis: Spermatogonia (mitosis) → Primary spermatocytes (meiosis I) → Secondary spermatocytes (meiosis II) → Spermatids → Spermatozoa; ~74 days; FSH (tubular function) + LH (testosterone production) regulate
- Testosterone: Virilization, spermatogenesis, libido, anabolic effects; negative feedback on HPG axis
- Erection: Parasympathetic → NO release → cGMP → smooth muscle relaxation → arterial dilation → corpus cavernosum engorgement
Female:
- Oogenesis: Begins in fetal life; meiosis arrested at prophase I until ovulation (completes meiosis I) and again at metaphase II until fertilization
- Menstrual cycle (28 days): Follicular phase (days 1-14, FSH drives follicle growth, rising estrogen) → LH surge (day 14) → Ovulation → Luteal phase (days 14-28, corpus luteum produces progesterone + estrogen) → if no fertilization, corpus luteum degenerates, menstruation
- Pregnancy: hCG maintains corpus luteum; placenta takes over progesterone/estrogen production at ~10 weeks; HPL for fetal nutrition
11. Lymphatic / Immune System
Anatomy
The blood and lymphatic systems consist of blood cells, lymphocytes, and lymphatic organs. - Color Atlas of Human Anatomy Vol. 2
- Primary lymphoid organs: Thymus (T-cell maturation, involutes after puberty), Bone marrow (B-cell and all blood cell development)
- Secondary lymphoid organs: Lymph nodes (bean-shaped, distributed along lymphatic vessels; cortex - B-cells in follicles, paracortex - T-cells, medulla - plasma cells and macrophages), Spleen (white pulp - immune function; red pulp - RBC filtration and storage), Tonsils and adenoids (Waldeyer's ring), Peyer's patches (gut-associated lymphoid tissue, GALT), Appendix
- Lymphatic vessels: Lymph capillaries (interstitium) → collecting lymphatics → lymph trunks → thoracic duct (drains body below diaphragm + left upper body into left subclavian vein) + right lymphatic duct
- Lymph: Filtered interstitial fluid + chylomicrons from gut (chyle)
- Blood cells: Erythrocytes (RBCs, biconcave, ~4.5-5.5 million/µL), Leukocytes (WBCs - neutrophils, eosinophils, basophils, monocytes, lymphocytes), Thrombocytes (platelets)
Physiology
- Lymph drainage: Returns ~2-4 L of interstitial fluid/day to circulation, preventing edema; driven by lymphatic smooth muscle contractions and skeletal muscle pump
- Innate immunity (non-specific, immediate):
- Physical barriers (skin, mucus, cilia)
- Phagocytes (neutrophils, macrophages) engulf pathogens
- Natural killer cells destroy virus-infected and tumor cells
- Complement system (classical, lectin, alternative pathways) → opsonization, membrane attack complex
- Pattern recognition receptors (Toll-like receptors) recognize PAMPs (pathogen-associated molecular patterns)
- Inflammation: Vasodilation, increased permeability, leukocyte recruitment (chemotaxis) driven by IL-1, TNF, IL-6, prostaglandins, histamine
- Adaptive immunity (specific, delayed, with memory):
- Humoral (B-cell mediated): Antigen presentation → B-cell activation + T-helper cell co-stimulation → plasma cells → antibodies (IgG, IgM, IgA, IgE, IgD); memory B-cells
- Cell-mediated (T-cell mediated): CD4⁺ T-helper cells (coordinate immune response via cytokines); CD8⁺ cytotoxic T-cells (kill virus-infected/cancer cells via perforin/granzyme); T-regulatory cells (suppress autoimmunity); memory T-cells
- MHC presentation: MHC class I (on all nucleated cells → presents intracellular antigens to CD8⁺); MHC class II (on APCs → presents extracellular antigens to CD4⁺)
- Clonal selection and expansion: Selected lymphocytes proliferate; produce effector cells and long-lived memory cells (basis of immunological memory and vaccination)
Summary Table
| System | Key Organs | Primary Functions |
|---|---|---|
| Integumentary | Skin, hair, nails, glands | Protection, thermoregulation, sensation, Vitamin D |
| Skeletal | 206 bones, cartilage, joints | Support, protection, movement, hematopoiesis, mineral storage |
| Muscular | Skeletal, cardiac, smooth muscle | Locomotion, posture, heat production, visceral movement |
| Nervous | Brain, spinal cord, nerves | Communication, integration, control, sensation |
| Endocrine | Pituitary, thyroid, adrenals, pancreas, gonads | Hormone-based regulation, metabolism, reproduction, growth |
| Cardiovascular | Heart, arteries, veins, capillaries | Pumps blood, distributes O₂/nutrients, removes CO₂/waste |
| Respiratory | Lungs, airways, respiratory muscles | Gas exchange (O₂ in, CO₂ out), acid-base balance |
| Digestive | Mouth → anus, liver, pancreas | Ingestion, digestion, absorption, elimination |
| Urinary | Kidneys, ureters, bladder, urethra | Filtration, excretion, fluid/electrolyte/acid-base balance |
| Reproductive | Gonads, ducts, accessory organs | Gamete production, fertilization, development |
| Lymphatic/Immune | Thymus, lymph nodes, spleen, lymphatics | Fluid return, immune surveillance, pathogen defense |
Sources: Color Atlas of Human Anatomy Vol. 2 (Thieme) | Medical Physiology (Boron & Boulpaep) | Costanzo Physiology 7th Ed. | Ganong's Review of Medical Physiology | Guyton and Hall Textbook of Medical Physiology
And its disease example
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Excellent - I now have rich textbook material. Here is the full disease examples section for all 11 body systems:
Disease Examples for the 11 Human Body Systems
1. Integumentary System
| Disease | Type | Key Features |
|---|---|---|
| Melanoma | Malignant | Uncontrolled growth of melanocytes; ABCDE criteria (Asymmetry, Border, Color, Diameter, Evolving); linked to UV exposure; can metastasize widely |
| Psoriasis | Autoimmune | T-cell mediated hyperproliferation of keratinocytes; thick, silvery plaques on extensor surfaces; Koebner phenomenon |
| Atopic Dermatitis (Eczema) | Inflammatory/Allergic | Defective filaggrin in stratum corneum → impaired barrier; intense pruritus, erythema, lichenification; strongly associated with asthma and allergic rhinitis |
| Basal Cell Carcinoma | Malignant | Most common skin cancer; arises from basal layer of epidermis; pearly, rolled edges with central ulceration; rarely metastasizes |
| Burns | Traumatic | Loss of barrier, fluid/electrolyte shifts (Parkland formula for resuscitation), infection risk; classified by depth (superficial, partial thickness, full thickness) |
| Cellulitis | Infectious | Bacterial (Staph/Strep) infection of dermis and subcutaneous tissue; erythema, warmth, swelling, pain; risk of sepsis if untreated |
Pathophysiological principle: Breakdown of the skin's barrier function - whether from autoimmunity, infection, or trauma - leads to systemic consequences including fluid loss, infection, and immune dysregulation.
2. Skeletal System
| Disease | Type | Key Features |
|---|---|---|
| Osteoporosis | Metabolic | Decreased bone mineral density (BMD); imbalance between osteoclast resorption and osteoblast formation; T-score ≤ -2.5 on DEXA; risk of fragility fractures (hip, vertebral, wrist) - Goldman-Cecil Medicine |
| Osteoarthritis | Degenerative | Breakdown of articular cartilage (loss of proteoglycans, chondrocyte death); subchondral bone sclerosis, osteophytes, joint space narrowing; affects weight-bearing joints (knees, hips) |
| Rheumatoid Arthritis | Autoimmune | Synovitis driven by anti-CCP and RF antibodies; pannus formation erodes cartilage and bone; symmetric small joint involvement; systemic inflammation |
| Osteosarcoma | Malignant | Most common primary bone malignancy in adolescents; arises in metaphysis of long bones; "sunburst" pattern on X-ray; associated with Rb gene mutations |
| Paget's Disease of Bone | Metabolic | Excessive and disorganized bone remodeling; elevated ALP; can cause deafness, skull enlargement, pathological fractures; treated with bisphosphonates |
| Rickets/Osteomalacia | Nutritional | Vitamin D deficiency → impaired calcium/phosphate deposition in osteoid; soft bones; bowing of legs in children; Looser zones on X-ray in adults |
3. Muscular System
| Disease | Type | Key Features |
|---|---|---|
| Duchenne Muscular Dystrophy (DMD) | Genetic | X-linked recessive; dystrophin gene mutation → absent dystrophin protein → sarcolemmal fragility → progressive muscle necrosis; Gowers' sign; CK markedly elevated; cardiomyopathy |
| Myasthenia Gravis | Autoimmune | Antibodies against nicotinic ACh receptors at NMJ → impaired neuromuscular transmission; fatigable weakness (ptosis, diplopia, bulbar weakness); Tensilon (edrophonium) test positive |
| Rhabdomyolysis | Traumatic/Metabolic | Massive skeletal muscle breakdown → myoglobin release → acute kidney injury; elevated CK >10,000 U/L; dark (tea-colored) urine |
| Polymyositis/Dermatomyositis | Autoimmune/Inflammatory | CD8⁺ T-cell attack on muscle fibers (polymyositis); Gottron's papules, heliotrope rash (dermatomyositis); proximal muscle weakness; elevated CK and aldolase |
| Compartment Syndrome | Traumatic | Increased pressure within a fascial compartment → ischemia; 5 P's: Pain (with passive stretch), Pallor, Paresthesia, Paralysis, Pulselessness; surgical emergency |
4. Nervous System
| Disease | Type | Key Features |
|---|---|---|
| Ischemic Stroke | Vascular | Thromboembolic or lacunar occlusion of cerebral arteries → neuronal death within minutes (ischemic penumbra); FAST acronym; tPA within 4.5 hours; thrombectomy up to 24 hours |
| Alzheimer's Disease | Neurodegenerative | Amyloid-beta plaques and neurofibrillary tangles (tau protein); progressive episodic memory loss, aphasia, apraxia; medial temporal lobe (hippocampus) affected first |
| Multiple Sclerosis (MS) | Autoimmune | Demyelination of CNS white matter by autoreactive T-cells; relapsing-remitting most common; oligoclonal bands in CSF; MRI - periventricular plaques |
| Parkinson's Disease | Neurodegenerative | Loss of dopaminergic neurons in substantia nigra → dopamine depletion in striatum; TRAP: Tremor (resting, pill-rolling), Rigidity (cogwheel), Akinesia, Postural instability; Lewy bodies |
| Epilepsy | Neurological | Recurrent seizures from abnormal synchronized neuronal discharge; focal or generalized; EEG abnormalities; treated with antiepileptics targeting Na⁺/Ca²⁺ channels or GABA |
| Meningitis | Infectious | Bacterial (N. meningitidis, S. pneumoniae) or viral (enteroviruses) inflammation of meninges; classic triad: fever, neck stiffness, photophobia; CSF analysis is diagnostic |
| Guillain-Barré Syndrome | Autoimmune | Post-infectious ascending demyelinating polyneuropathy; areflexia, ascending weakness; cytoalbuminous dissociation in CSF (high protein, normal cells); IVIG or plasmapheresis |
5. Endocrine System
| Disease | Type | Key Features |
|---|---|---|
| Type 1 Diabetes Mellitus | Autoimmune | Autoimmune destruction of beta cells (HLA-DR3/DR4 linked) → absolute insulin deficiency → hyperglycemia, DKA risk; requires lifelong insulin; onset typically in childhood/young adults - Guyton & Hall |
| Type 2 Diabetes Mellitus | Metabolic | Peripheral insulin resistance + progressive beta-cell failure; hyperglycemia, dyslipidemia, hypertension (metabolic syndrome); HbA1c used for monitoring; can lead to nephropathy, retinopathy, neuropathy, vasculopathy - Guyton & Hall |
| Hypothyroidism | Deficiency | Low T3/T4 → decreased BMR; weight gain, cold intolerance, bradycardia, constipation, myxedema; most common cause: Hashimoto's thyroiditis (autoimmune); treated with levothyroxine |
| Hyperthyroidism (Graves' Disease) | Autoimmune | TSH-receptor stimulating antibodies → excess T3/T4; weight loss, heat intolerance, tachycardia, exophthalmos, pretibial myxedema; treated with antithyroids, radioiodine, or thyroidectomy |
| Cushing's Syndrome | Hormonal excess | Excess glucocorticoids (most common cause: exogenous steroids; endogenous: ACTH-secreting pituitary adenoma = Cushing's disease); central obesity, moon face, buffalo hump, striae, hypertension, diabetes, osteoporosis |
| Addison's Disease | Deficiency | Primary adrenal insufficiency; cortisol and aldosterone deficiency; hypotension, hyponatremia, hyperkalemia, hyperpigmentation (elevated ACTH); can precipitate life-threatening adrenal crisis |
| Acromegaly | Hormonal excess | Excess GH in adults (usually pituitary adenoma) → excess IGF-1; coarsening of facial features, enlarged hands/feet, macroglossia, sleep apnea, diabetes, cardiomegaly |
6. Cardiovascular System
| Disease | Type | Key Features |
|---|---|---|
| Acute Myocardial Infarction (MI) | Ischemic | Rupture of atherosclerotic plaque → coronary thrombosis → myocardial necrosis; STEMI vs NSTEMI (based on ECG and troponin); "time is muscle" - reperfusion via PCI or thrombolysis - Braunwald's Heart Disease |
| Heart Failure | Functional | Reduced cardiac output to meet metabolic demands; systolic (reduced EF) or diastolic (preserved EF) dysfunction; Framingham criteria; Starling law derangement; RAAS activation perpetuates fluid retention - Brenner and Rector's Kidney |
| Hypertension | Vascular | Sustained BP >130/80 mmHg; silent killer; damages target organs (heart, kidney, brain, eyes, vessels); essential (95%) vs secondary; treated with lifestyle + antihypertensives (ACEi, ARBs, CCBs, thiazides) |
| Atrial Fibrillation | Arrhythmia | Chaotic atrial electrical activity; irregularly irregular pulse; stroke risk (Virchow's triad in left atrial appendage); CHA₂DS₂-VASc score for anticoagulation; rate vs rhythm control |
| Infective Endocarditis | Infectious | Bacterial (Streptococcus, Staphylococcus) infection of cardiac valves; vegetation formation → valve destruction, emboli; Osler's nodes, Janeway lesions, Roth spots; Duke criteria for diagnosis |
| Deep Vein Thrombosis / PE | Thromboembolic | Virchow's triad (stasis, hypercoagulability, endothelial damage); DVT → pulmonary embolism; Wells score, D-dimer, CT pulmonary angiography; anticoagulation treatment |
7. Respiratory System
Respiratory diseases fall into three main categories: obstructive, restrictive, and vascular pathophysiology. - Harrison's Principles of Internal Medicine
| Disease | Type | Key Features |
|---|---|---|
| Asthma | Obstructive/Inflammatory | Reversible airway bronchoconstriction, inflammation, hyperresponsiveness; triggered by allergens, exercise, cold, infections; eosinophilic inflammation; β₂-agonists (acute relief), inhaled corticosteroids (maintenance) |
| COPD | Obstructive (irreversible) | Emphysema (alveolar wall destruction, loss of elastic recoil) + chronic bronchitis ("blue bloater" - excess mucus, cough ≥3 months/2 years); FEV₁/FVC <0.70; caused by smoking; managed with bronchodilators, pulmonary rehab |
| Pneumonia | Infectious | Alveolar consolidation by bacteria (S. pneumoniae most common), viruses, or fungi; lobar, broncho-, or interstitial patterns; productive cough, fever, crackles; CXR consolidation |
| Pulmonary Embolism (PE) | Vascular | DVT fragment lodges in pulmonary vasculature → V/Q mismatch, right heart strain; sudden dyspnea, pleuritic chest pain, hemoptysis; Wells score + CTPA for diagnosis |
| Idiopathic Pulmonary Fibrosis (IPF) | Restrictive/Fibrotic | Progressive fibrosis of alveolar walls → reduced compliance, reduced DLCO; "honeycomb" pattern on HRCT; UIP pattern on biopsy; no cure, nintedanib/pirfenidone slow progression |
| Lung Cancer | Malignant | Non-small cell (adenocarcinoma, squamous cell) vs small-cell (SCLC); strongly linked to smoking; para-neoplastic syndromes; EGFR/ALK mutations guide targeted therapy |
| Tuberculosis (TB) | Infectious | Mycobacterium tuberculosis; latent vs active; Ghon complex (primary); cavitary lesions (secondary reactivation); acid-fast bacilli on smear; RIPE therapy |
8. Digestive System
| Disease | Type | Key Features |
|---|---|---|
| Inflammatory Bowel Disease (IBD) | Autoimmune/Inflammatory | Two major forms: Crohn's disease (transmural inflammation, any GI segment, skip lesions, granulomas, cobblestoning) and Ulcerative colitis (mucosal inflammation, rectum to colon, continuous, pseudopolyps); complex polygenic disorders with peak incidence in 2nd-4th decade - Goldman-Cecil Medicine |
| Peptic Ulcer Disease (PUD) | Inflammatory | Mucosal erosion into submucosa/muscularis; H. pylori infection (70% of duodenal, 90% of gastric) + NSAIDs disrupt mucosal defense; epigastric pain, GI bleeding (hematemesis, melena) |
| Cirrhosis | Fibrotic/End-stage | Hepatocyte death → fibrosis → nodular regeneration; causes: alcohol, NAFLD, viral hepatitis (B, C); portal hypertension (varices, splenomegaly, ascites), hepatic encephalopathy, coagulopathy, jaundice |
| Colorectal Cancer | Malignant | Adenoma → carcinoma sequence (APC gene mutation); FAP (familial polyposis); Lynch syndrome (MSI); screening by colonoscopy; change in bowel habits, rectal bleeding |
| Acute Pancreatitis | Inflammatory | Premature activation of pancreatic enzymes → auto-digestion; causes: gallstones (most common), alcohol; epigastric pain radiating to back, elevated lipase/amylase; Ranson criteria for severity |
| Gastroesophageal Reflux Disease (GERD) | Functional/Inflammatory | Lower esophageal sphincter dysfunction → acid reflux; heartburn, regurgitation; Barrett's esophagus (columnar metaplasia) → adenocarcinoma risk; treated with PPIs |
9. Urinary System
| Disease | Type | Key Features |
|---|---|---|
| Chronic Kidney Disease (CKD) | Degenerative | Progressive irreversible loss of renal function; causes: hypertension, diabetes (nephrosclerosis), chronic glomerulonephritis, polycystic kidney disease; GFR <60 mL/min for >3 months = CKD; stages 1-5 (ESRD at stage 5) - Henry's Clinical Diagnosis |
| Acute Kidney Injury (AKI) | Functional | Sudden decline in GFR; prerenal (hypovolemia, shock), intrinsic (ATN, glomerulonephritis), postrenal (obstruction); KDIGO criteria; oliguria, rising creatinine, electrolyte disturbances |
| Nephrotic Syndrome | Glomerular | Massive proteinuria (>3.5 g/day) → hypoalbuminemia → edema, hyperlipidemia, lipiduria; causes: minimal change disease (children), focal segmental glomerulosclerosis, membranous nephropathy |
| Nephritic Syndrome | Glomerular | Hematuria (RBC casts), hypertension, oliguria, mild proteinuria; causes: post-streptococcal GN, IgA nephropathy (most common worldwide), lupus nephritis, Goodpasture's |
| Urinary Tract Infection (UTI) | Infectious | E. coli most common; cystitis (lower): dysuria, frequency, urgency; pyelonephritis (upper): flank pain, fever, costovertebral tenderness; urine culture guides antibiotic therapy |
| Renal Cell Carcinoma (RCC) | Malignant | Clear cell (most common, VHL gene); classic triad: hematuria, flank pain, palpable mass; paraneoplastic syndromes (erythrocytosis, hypercalcemia); treated with nephrectomy + targeted therapy (sunitinib) |
| Polycystic Kidney Disease (PKD) | Genetic | Autosomal dominant (PKD1/PKD2 mutations); progressive cyst enlargement → CKD; hypertension, hematuria; associated with berry aneurysms, mitral valve prolapse, liver cysts |
10. Reproductive System
| Disease | Type | Key Features |
|---|---|---|
| Polycystic Ovary Syndrome (PCOS) | Endocrine/Reproductive | Androgen excess, oligoanovulation, polycystic ovaries; insulin resistance; irregular periods, hirsutism, acne, infertility; Rotterdam criteria (2 of 3 features); managed with OCPs, metformin, clomiphene |
| Endometriosis | Inflammatory | Ectopic endometrial tissue outside uterus (ovaries, pelvic peritoneum); cyclical pain, dysmenorrhea, dyspareunia, infertility; chocolate cysts (endometriomas); laparoscopy is gold standard for diagnosis |
| Benign Prostatic Hyperplasia (BPH) | Hyperplastic | DHT-driven stromal and glandular hyperplasia of transitional zone; lower urinary tract symptoms (LUTS): hesitancy, weak stream, nocturia; PSA may be elevated; α-blockers and 5α-reductase inhibitors |
| Prostate Cancer | Malignant | Most common male cancer (after skin); adenocarcinoma of peripheral zone; PSA screening; Gleason score; BRCA2 mutations increase risk; androgen deprivation therapy for advanced disease |
| Cervical Cancer | Malignant | HPV 16/18 infection → squamous cell carcinoma or adenocarcinoma; preventable with HPV vaccine; screened with Pap smear + HPV co-testing; radical hysterectomy or radiation/chemotherapy |
| Ectopic Pregnancy | Obstetric | Implantation outside uterus (usually fallopian tube ampulla); rupture → hemorrhage, shock; hCG rises abnormally slowly; transvaginal ultrasound diagnostic; methotrexate (early) or surgery |
| Testicular Cancer | Malignant | Most common solid cancer in young men (15-35 yrs); germ cell tumors (seminoma, non-seminoma); painless testicular mass; elevated AFP, β-hCG, LDH; highly curable with chemotherapy (BEP regimen) |
11. Lymphatic / Immune System
| Disease | Type | Key Features |
|---|---|---|
| Hodgkin Lymphoma | Malignant | Reed-Sternberg cells (B-cell origin, CD15⁺/CD30⁺); bimodal age distribution; painless lymphadenopathy, B symptoms (fever, night sweats, weight loss); highly curable with ABVD chemotherapy |
| Non-Hodgkin Lymphoma (NHL) | Malignant | Heterogeneous group; B-cell (diffuse large B-cell, follicular, Burkitt's) or T-cell; Burkitt's - c-Myc translocation t(8;14); associated with HIV, EBV, immunosuppression - Harrison's Principles |
| Leukemia | Malignant | Malignant proliferation of hematopoietic cells; ALL (childhood, B or T-cell), AML (adults), CLL (B-cell, elderly - most common adult leukemia), CML (BCR-ABL t(9;22) Philadelphia chromosome → imatinib) - Harrison's Principles |
| HIV/AIDS | Infectious/Immune | HIV destroys CD4⁺ T-helper cells → progressive immunodeficiency; AIDS: CD4 <200/µL or AIDS-defining illness; opportunistic infections (PCP, CMV, toxoplasmosis, Cryptococcus); ART (antiretroviral therapy) |
| Systemic Lupus Erythematosus (SLE) | Autoimmune | Multi-system autoimmune disease; anti-dsDNA and anti-Smith antibodies; malar rash, photosensitivity, oral ulcers, serositis, glomerulonephritis, cytopenias; SLICC criteria |
| Lymphedema | Lymphatic obstruction | Impaired lymph drainage → protein-rich interstitial fluid accumulation; primary (Milroy's disease) or secondary (post-mastectomy, filariasis); non-pitting edema; irreversible fibrosis if untreated |
| Anaphylaxis | Immune/Allergic | IgE-mediated mast cell and basophil degranulation → massive histamine, leukotrienes, prostaglandins release; urticaria, angioedema, bronchospasm, hypotension; epinephrine IM is first-line treatment |
| Common Variable Immunodeficiency (CVID) | Primary Immunodeficiency | Low immunoglobulins, poor vaccine responses; recurrent sinopulmonary infections; increased risk of autoimmunity and lymphoma; treated with IVIG replacement |
Master Summary Table
| Body System | Key Diseases (Examples) | Core Mechanism |
|---|---|---|
| Integumentary | Melanoma, Psoriasis, Eczema, Cellulitis | Barrier disruption, aberrant inflammation, malignant transformation |
| Skeletal | Osteoporosis, Osteoarthritis, RA, Osteosarcoma | Remodeling imbalance, cartilage degeneration, autoimmunity, malignancy |
| Muscular | DMD, Myasthenia Gravis, Rhabdomyolysis | Structural protein defect, NMJ dysfunction, muscle breakdown |
| Nervous | Stroke, Alzheimer's, MS, Parkinson's, Epilepsy | Ischemia, neurodegeneration, demyelination, dopamine loss, dysrhythmia |
| Endocrine | DM Type 1 & 2, Hypothyroidism, Cushing's, Addison's | Hormone deficiency or excess, receptor resistance, gland destruction |
| Cardiovascular | MI, Heart Failure, Hypertension, AF | Atherosclerosis, pump failure, increased vascular resistance, arrhythmia |
| Respiratory | Asthma, COPD, Pneumonia, IPF, Lung Cancer | Airway obstruction, inflammation, fibrosis, infection, malignancy |
| Digestive | IBD, PUD, Cirrhosis, Colorectal Cancer, Pancreatitis | Mucosal damage, autoimmunity, fibrosis, malignant transformation |
| Urinary | CKD, AKI, Nephrotic Syndrome, UTI, PKD | Nephron loss, filtration failure, glomerular damage, obstruction, infection |
| Reproductive | PCOS, Endometriosis, Prostate/Cervical Cancer, Ectopic | Hormonal imbalance, ectopic tissue, HPV/oncogene-driven malignancy |
| Lymphatic/Immune | HIV/AIDS, SLE, Leukemia, Lymphoma, Anaphylaxis | Immunodeficiency, autoimmunity, malignant lymphoproliferation, dysregulated IgE |
Sources: Harrison's Principles of Internal Medicine 22E | Guyton and Hall Textbook of Medical Physiology | Goldman-Cecil Medicine | Braunwald's Heart Disease | Brenner and Rector's The Kidney | Henry's Clinical Diagnosis and Management
Difference between in dm 1 and dm 2 with explanation lije a story And body blood flow of oxygenated blood and deoxygenated blood exchange explain
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have everything needed - rich textbook content and a real diagram. Let me deliver both answers in full.
Part 1: DM Type 1 vs DM Type 2 - Told as a Story
The Town of Sugarville and Two Very Different Problems
Imagine your body is a busy town called Sugarville. The streets are your blood vessels. Sugar molecules (glucose) are the fuel trucks driving through the streets, delivering energy to every house (cell) in town.
For the fuel trucks to unload their cargo into any house, they need a special key - and that key is called INSULIN. Without the key, the trucks just pile up on the streets, the houses starve, and the streets become dangerously congested.
Now, Sugarville has TWO very different stories...
🔑 Story 1: Type 1 Diabetes - "The Key Factory Burns Down"
Meet Tommy, age 9.
Tommy's body has a small but very important factory in the basement of a place called the Pancreas Building. This factory is the Beta Cell Workshop - and it manufactures those special insulin keys all day, every day.
One day, something goes terribly wrong. Tommy's own immune army - the soldiers meant to fight germs - gets confused. Perhaps a virus visited Sugarville and looked too similar to the Beta Cell Workshop. The immune soldiers could not tell them apart.
"In type 1 diabetes, a complex interplay of genetic, environmental, and autoimmune factors selectively targets insulin-producing pancreatic islet β cells and ultimately destroys them... β-cell destruction is largely mediated by CD8+ and CD4+ T cells, macrophages - causing apoptosis or cellular destruction." - Goldman-Cecil Medicine
The immune army attacks the Beta Cell Workshop. CD8+ T-cell soldiers storm in, CD4+ soldiers coordinate the attack, macrophages clean up the rubble. The building burns completely to the ground. Every key maker is gone.
Result? No more insulin keys. Ever. The fuel trucks (glucose) pile up in the streets. Blood sugar skyrockets. The houses (cells) scream for energy but nobody can get in. The body, desperate for fuel, starts breaking down fat reserves - releasing ketone bodies, turning the blood acidic. This is Diabetic Ketoacidosis (DKA) - a life-threatening emergency.
Tommy is rushed to the hospital. He is thin, weak, urinating constantly (the kidneys frantically try to flush out the excess sugar - polyuria), drinking water non-stop (polydipsia), and losing weight fast.
The only fix? Give Tommy artificial keys every single day - insulin injections. The factory is permanently gone, so the keys must come from outside. Tommy will need insulin for the rest of his life.
| DM Type 1 Quick Facts | |
|---|---|
| Who | Children, teenagers, young adults (but can occur at any age) |
| What happened | Beta cells completely destroyed by autoimmunity |
| Insulin level | Zero (absolute deficiency) |
| Antibodies | Anti-GAD65, anti-IA-2, anti-ZnT8, anti-insulin |
| Genes | HLA DR3-DQ2 / DR4-DQ8 on chromosome 6 (~50% of risk) |
| Onset | Sudden, dramatic - often presents in DKA |
| Body type | Usually thin/normal weight |
| Treatment | Insulin - always, no exceptions |
🏚️ Story 2: Type 2 Diabetes - "The Locks Get Rusty"
Now meet Margaret, age 54.
Margaret's Beta Cell Workshop is still standing. It is still making insulin keys. The problem is somewhere else entirely.
Over many years - from a diet rich in processed food, reduced activity, and gradual weight gain - the locks on the doors of every house (cell receptor) have become rusty and jammed. The keys still exist, but they no longer fit properly.
This is called insulin resistance.
"Type 2 diabetes: a combination of insulin resistance and defective insulin secretion." - Henry's Clinical Diagnosis
The key factory (beta cells) notices the locks are not working. So it tries harder - pumping out more and more keys to compensate. For years, even decades, this works. Blood sugar stays somewhat normal. Margaret doesn't feel it. This is the silent phase - prediabetes.
But after years of overworking, the key factory starts to wear out. Production slows. The combination of rusty locks AND a tired factory means sugar starts building up in the streets again. Blood glucose creeps up slowly. Unlike Tommy's dramatic collapse, Margaret's sugar rises silently over years.
She gains weight around her abdomen. Visceral fat cells release inflammatory signals (free fatty acids, TNF-α, IL-6) that jam the insulin signaling pathway inside cells. Eventually her doctor notices her fasting glucose is 140 mg/dL and her HbA1c is 8.2%. She is diagnosed with Type 2 Diabetes.
The good news: The locks are not permanently broken. With weight loss, exercise, and medication, many can be oiled and repaired. Metformin reduces glucose production in the liver. GLP-1 agonists restore some key-factory function. Lifestyle changes can even reverse early Type 2 diabetes.
| DM Type 2 Quick Facts | |
|---|---|
| Who | Middle-aged and older adults; increasingly younger due to obesity |
| What happened | Insulin resistance + gradual beta-cell exhaustion |
| Insulin level | Normal or HIGH early on; low later as beta cells fail |
| Antibodies | Usually none |
| Risk factors | Obesity (especially visceral), inactivity, family history, ethnicity |
| Onset | Slow, silent - often found incidentally on routine testing |
| Body type | Usually overweight/obese |
| Treatment | Lifestyle, metformin, GLP-1 agonists, SGLT2 inhibitors, eventually insulin |
Head-to-Head Comparison Table
| Feature | Type 1 DM | Type 2 DM |
|---|---|---|
| The story | Key factory destroyed | Locks became rusty |
| Core defect | Absolute insulin deficiency | Insulin resistance + relative insulin deficiency |
| Cause | Autoimmune (T-cell mediated) | Metabolic/lifestyle + genetic |
| Age of onset | Usually <30 years | Usually >40 years (but rising in younger people) |
| Body weight | Usually normal/thin | Usually overweight/obese |
| Speed of onset | Rapid (days to weeks) | Slow (years to decades) |
| DKA | Common, can be first presentation | Rare (possible in severe illness - "ketosis-prone T2D") |
| C-peptide | Very low/undetectable | Normal or elevated early; reduced later |
| Autoantibodies | Positive (GAD65, IA-2, ZnT8) | Negative |
| HLA association | DR3-DQ2, DR4-DQ8 | Not HLA-linked; TCF7L2, KCNJ11, PPARG genes |
| Twin concordance | 30-40% (identical twins) | ~70-90% (identical twins) |
| Insulin needed? | Always, from diagnosis | Only after beta-cell failure; many manage without |
| Reversible? | No - beta cells permanently gone | Partially - early T2D can remit with weight loss |
| Complications | Both share: retinopathy, nephropathy, neuropathy, cardiovascular disease |
Part 2: The Journey of Blood Around the Body - Oxygenated and Deoxygenated Exchange
Think of the circulatory system as a figure-of-eight highway with the heart at the crossroads. - Color Atlas of Human Anatomy Vol. 2
Here is the diagram from Costanzo Physiology:
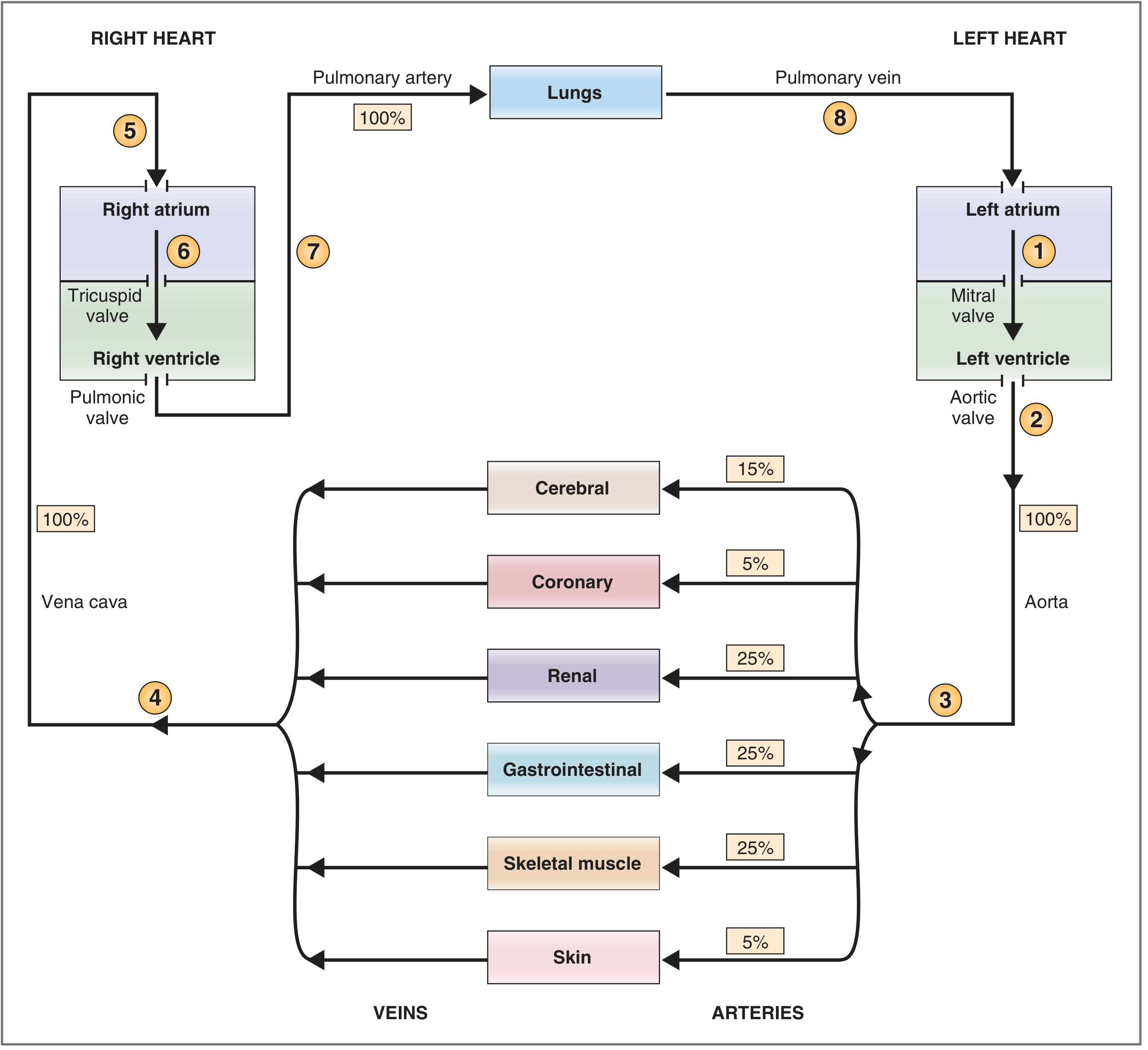
The Two Loops
The circulation is divided into two consecutive circuits that work in series - one loop for the lungs, one loop for the entire body.
🔵 Loop 1: The Pulmonary Circulation (Right Heart → Lungs → Left Heart)
Deoxygenated blood gets recharged
Body tissues
↓ (used up O₂, full of CO₂)
Superior Vena Cava + Inferior Vena Cava
↓
Right Atrium → [Tricuspid Valve] → Right Ventricle
↓ [Pulmonic Valve]
Pulmonary Trunk → Right + Left Pulmonary ARTERIES
↓ (the ONLY arteries carrying deoxygenated blood!)
Pulmonary Capillaries surrounding Alveoli
↓ GAS EXCHANGE HAPPENS HERE:
O₂ diffuses IN (alveolar PO₂ ~100 mmHg → blood ~40 mmHg)
CO₂ diffuses OUT (blood PCO₂ ~45 mmHg → alveoli ~40 mmHg)
↓ (now fresh, oxygenated, bright red blood)
Pulmonary VEINS (the ONLY veins carrying oxygenated blood!)
↓
Left Atrium
"Deoxygenated blood from the systemic circulation flows from the right atrium into the right ventricle and from there into the pulmonary circulation... the blood is enriched with oxygen and carbon dioxide is released into the airways. The oxygenated blood leaves the lungs by the pulmonary veins and flows to the left atrium." - Color Atlas of Human Anatomy Vol. 2
Key point: Arteries normally carry oxygenated blood - but the pulmonary arteries are the exception - they carry deoxygenated blood to the lungs. Veins normally carry deoxygenated blood - but the pulmonary veins are the exception - they carry oxygenated blood back to the heart.
🔴 Loop 2: The Systemic Circulation (Left Heart → Entire Body → Right Heart)
Oxygenated blood gets distributed to every organ
Left Atrium → [Mitral Valve] → Left Ventricle
↓ [Aortic Valve]
AORTA (pumped at 120 mmHg systolic - high pressure)
↓ branches into organ-specific arteries
├── Cerebral arteries → Brain (15% of cardiac output)
├── Coronary arteries → Heart muscle (5%)
├── Renal arteries → Kidneys (25%)
├── Mesenteric/celiac arteries → GI tract (25%)
├── Skeletal muscle arteries → Muscles (25% at rest, up to 80% during exercise)
└── Cutaneous arteries → Skin (5%)
↓ (at each organ: capillaries)
GAS EXCHANGE:
O₂ leaves blood → enters cells
CO₂ leaves cells → enters blood
Nutrients (glucose, amino acids) delivered
Waste products (CO₂, urea, lactic acid) collected
↓ (now deoxygenated, dark red blood)
├── Veins from legs/abdomen → Inferior Vena Cava
└── Veins from head/arms → Superior Vena Cava
↓
Right Atrium (cycle restarts)
"Oxygenated blood from the lung flows from the left atrium of the heart into the left ventricle. From there it is pumped through the aorta into the systemic circulation, which consists of numerous separate circuits supplying individual organs... At the capillary plexus, exchange of gases and metabolic products occurs." - Color Atlas of Human Anatomy Vol. 2
🌿 The Portal Circulation - A Special Detour
After absorbing nutrients from food, blood from the gut, pancreas, and spleen does NOT go straight to the vena cava. It makes a detour:
GI capillaries (nutrient-rich after eating)
↓
Portal Vein
↓
Liver sinusoids (hepatocytes process glucose, amino acids, toxins)
↓
Hepatic Veins
↓
Inferior Vena Cava → Right Atrium
This is why the liver is called the metabolic gatekeeper - everything absorbed from food passes through it first. - Color Atlas of Human Anatomy Vol. 2
Where Exactly Does Gas Exchange Happen?
In the Lungs (Pulmonary)
| Gas | Direction | Driving Force |
|---|---|---|
| O₂ | Alveolus → Blood | PO₂ alveolus ~100 mmHg vs. blood ~40 mmHg |
| CO₂ | Blood → Alveolus | PCO₂ blood ~45 mmHg vs. alveolus ~40 mmHg |
In the Tissues (Systemic Capillaries)
| Gas | Direction | Driving Force |
|---|---|---|
| O₂ | Blood → Cell | PO₂ arterial blood ~95 mmHg vs. tissue ~40 mmHg |
| CO₂ | Cell → Blood | PCO₂ tissue ~46 mmHg vs. arterial blood ~40 mmHg |
The Bohr effect helps: when tissues are metabolically active (acidic, high CO₂), hemoglobin's grip on oxygen loosens - releasing more O₂ exactly where it is needed most.
The Complete Journey - One Breath's Worth of Oxygen
- You breathe in → O₂ enters alveoli
- O₂ diffuses across the thin alveolar-capillary membrane (0.5 µm thick) into blood
- O₂ binds hemoglobin in red blood cells (98.5%) → blood turns bright red
- Pulmonary veins carry it to the left atrium
- Left ventricle pumps it into the aorta at high pressure
- Blood distributes to every organ through branches of the aorta
- At tissue capillaries: O₂ unloads into cells; CO₂ loads onto blood
- Dark, deoxygenated blood travels back through veins → vena cava → right atrium
- Right ventricle pumps it through the pulmonary artery back to the lungs
- CO₂ is exhaled → you breathe out
- The cycle repeats ~70 times per minute, every minute of your life
Sources: Goldman-Cecil Medicine International Edition | Henry's Clinical Diagnosis and Management | Color Atlas of Human Anatomy Vol. 2 (Thieme) | Costanzo Physiology 7th Ed. | Harrison's Principles of Internal Medicine 22E
This is a shared conversation. Sign in to Orris to start your own chat.