Here are all 17 questions with full 7-mark university exam answers:
ANATOMY - FIRST YEAR MBBS
COMPLETE 7-MARK UNIVERSITY EXAM ANSWERS
Q.1 - Describe the Attachments of Rotator Cuff Muscles [7 Marks]
Introduction
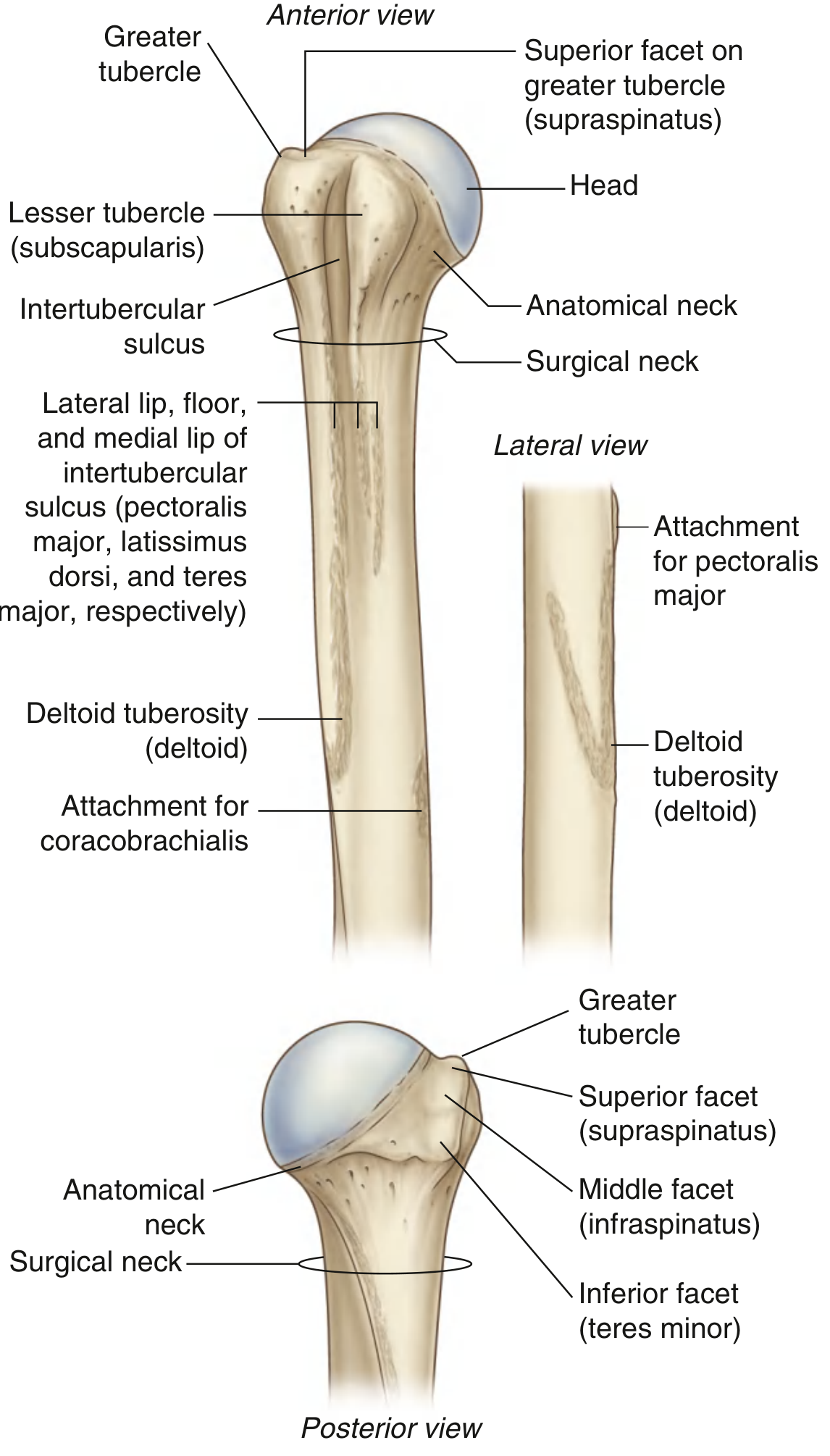
The rotator cuff is a group of four muscles arising from the scapula whose tendons blend with the fibrous capsule of the glenohumeral joint to form a musculotendinous cuff. This cuff stabilizes the humeral head within the shallow glenoid fossa, preventing dislocation during shoulder movements.
The Four Rotator Cuff Muscles (Mnemonic: SITS)
1. Supraspinatus
| Feature | Details |
|---|
| Origin | Supraspinous fossa of the scapula (medial 2/3 of the fossa) and the overlying supraspinous fascia |
| Course | Passes laterally under the acromion and the coracoacromial ligament (subacromial space) |
| Insertion | Superior facet of the greater tubercle of the humerus; also blends with the superior capsule |
| Nerve supply | Suprascapular nerve (C5, C6) |
| Action | Initiates abduction (first 0-15°); stabilizes humeral head |
2. Infraspinatus
| Feature | Details |
|---|
| Origin | Infraspinous fossa of the scapula (medial 2/3) and overlying infraspinous fascia |
| Course | Passes laterally across the posterior aspect of the glenohumeral joint |
| Insertion | Middle facet of the greater tubercle of the humerus; blends with the posterior joint capsule |
| Nerve supply | Suprascapular nerve (C5, C6) |
| Action | Lateral (external) rotation of the arm; stabilizes posterior capsule |
3. Teres Minor
| Feature | Details |
|---|
| Origin | Upper 2/3 of the dorsal surface of the lateral border of the scapula |
| Course | Passes obliquely upward and laterally |
| Insertion | Inferior facet of the greater tubercle of the humerus; also blends with the inferior posterior joint capsule |
| Nerve supply | Posterior branch of the axillary nerve (C5, C6) |
| Action | Lateral rotation and weak adduction of the arm |
4. Subscapularis
| Feature | Details |
|---|
| Origin | Medial 2/3 of the subscapular fossa (costal/anterior surface of scapula) |
| Course | Passes anteriorly, crossing in front of the glenohumeral joint capsule |
| Insertion | Lesser tubercle of the humerus; also blends with the anterior joint capsule and transverse humeral ligament |
| Nerve supply | Upper subscapular nerve (C5, C6) and lower subscapular nerve (C5, C6, C7) |
| Action | Medial (internal) rotation of the arm; stabilizes anterior capsule |
Diagram
Fig. 1: Proximal end of right humerus (anterior and posterior views) showing all four rotator cuff attachment sites (Gray's Anatomy for Students)
How the Rotator Cuff Stabilizes the Shoulder Joint
The glenohumeral joint is inherently unstable (shallow glenoid, large humeral head). The rotator cuff provides dynamic stability by:
- Compressing the humeral head into the glenoid
- Counteracting the upward pull of the deltoid during abduction (supraspinatus creates a force couple with deltoid)
- Creating a "compressive sling" around the joint
Summary Table
| Muscle | Origin | Insertion | Nerve | Action |
|---|
| Supraspinatus | Supraspinous fossa | Superior facet - greater tubercle | Suprascapular (C5, C6) | Abduction (initiates), stabilizes |
| Infraspinatus | Infraspinous fossa | Middle facet - greater tubercle | Suprascapular (C5, C6) | Lateral rotation |
| Teres minor | Lateral border of scapula | Inferior facet - greater tubercle | Axillary (C5, C6) | Lateral rotation, adduction |
| Subscapularis | Subscapular fossa | Lesser tubercle | Upper + Lower subscapular (C5, C6, C7) | Medial rotation |
Applied Anatomy (Clinical Importance)
- Rotator cuff tears: Most common in supraspinatus tendon (at its "critical zone" - 1 cm proximal to insertion, avascular watershed area). Caused by impingement under the acromion, degeneration, or trauma.
- Painful arc syndrome: Pain at 60-120° of abduction due to supraspinatus impingement.
- Supraspinatus test (empty can test): Arm at 90° abduction, 30° forward flexion, thumb pointing down - weakness suggests supraspinatus tear.
- Subacromial bursitis: Inflammation of the bursa between the cuff and acromion commonly accompanies rotator cuff pathology.
- Calcific tendinitis: Calcium deposits commonly form in the supraspinatus tendon.
Q.2 - Attachments, Actions and Nerve Supply of Deltoid [7 Marks]
Introduction
The deltoid is a large, multipennate, triangular-shaped muscle that forms the rounded contour of the shoulder. It is the most powerful abductor of the arm and the principal muscle acting on the glenohumeral joint.
Attachments
Origin (broad, from three parts - the "DCA" arch: Deltoid, Clavicle, Acromion)
The origin of the deltoid is a continuous line corresponding to the insertion of the trapezius:
| Part | Origin |
|---|
| Anterior (clavicular) part | Anterior border and superior surface of the lateral 1/3 of the clavicle |
| Middle (acromial) part | Lateral margin and superior surface of the acromion process of the scapula |
| Posterior (spinal) part | Lower lip of the crest of the spine of the scapula |
Insertion (all three parts converge)
All three parts converge into a V-shaped tendon that inserts into the deltoid tuberosity - a V-shaped roughening on the middle of the lateral surface of the humerus.
Actions
| Part | Primary Action | Secondary Actions |
|---|
| Anterior | Flexion of arm | Medial rotation; horizontal adduction |
| Middle | Abduction (main muscle for 15°-90°) | - |
| Posterior | Extension of arm | Lateral rotation; horizontal abduction |
| All together | Abduction of arm (against resistance) | Stabilization of shoulder |
Important: Deltoid takes over abduction from supraspinatus at 15° and maintains it to 90°. After 90°, trapezius and serratus anterior rotate the scapula to allow further elevation.
Nerve Supply
- Axillary nerve (C5, C6) - from the posterior cord of the brachial plexus
- The axillary nerve winds around the surgical neck of the humerus within the quadrangular space
- The anterior branch of the axillary nerve supplies the anterior and middle parts; the posterior branch supplies the posterior part
- The posterior branch also gives rise to the superior lateral cutaneous nerve of the arm (sensory to the "regimental badge area")
Relations
- Deep to deltoid: Rotator cuff muscles, glenohumeral joint, subdeltoid/subacromial bursa, axillary nerve, posterior circumflex humeral vessels
- Superficial: Only skin and subcutaneous fascia
- Medial boundary: Pectoralis major (anterior axillary fold)
Applied Anatomy
1. IM Injections
The deltoid is the preferred site for intramuscular injections (vaccines, drugs). The safe zone is the middle of the muscle, at least 2 cm below the acromion.
2. Axillary Nerve Injury
Injury to the axillary nerve is the most important clinical complication of:
- Fracture of the surgical neck of humerus (most common cause)
- Anterior dislocation of the shoulder (nerve is stretched)
- Compression from crutches (rarely)
Effects of axillary nerve injury:
- Paralysis of deltoid → loss of abduction of arm (patient cannot initiate abduction)
- Paralysis of teres minor
- Loss of sensation over the "Regimental badge" area (skin over the lower half of the deltoid)
- Deltoid wasting over time (flat shoulder contour)
3. Testing the Axillary Nerve
Always test axillary nerve BEFORE and AFTER reduction of a shoulder dislocation:
- Ask patient to abduct the arm against resistance
- Test sensation over the regimental badge area
4. Deltoid Tuberosity
The deltoid inserts at the lateral mid-shaft of the humerus. Fractures at this level may cause the proximal fragment to be abducted (pulled by deltoid) and the distal fragment to be adducted.
Q.3 - Enumerate Structures Under Cover of Deltoid Muscle [7 Marks]
Introduction
The deltoid muscle acts as a protective covering over the shoulder region. Several anatomically important structures lie deep to it, and knowledge of these is essential for understanding surgical approaches to the shoulder and for interpreting clinical signs.
Structures Deep to the Deltoid
A. Bones and Joints
-
Proximal end of the humerus:
- Head of humerus (covered by joint capsule)
- Greater tubercle (with the three facets for rotator cuff insertions)
- Lesser tubercle
- Surgical neck of humerus
- Deltoid tuberosity (where deltoid inserts)
-
Glenohumeral (shoulder) joint - the synovial joint between the head of humerus and glenoid fossa of scapula
-
Lateral end of the clavicle and acromioclavicular joint (partially)
B. Muscles (Rotator Cuff and Others)
| Muscle | Position |
|---|
| Supraspinatus | Passes under the acromion and deltoid to insert on greater tubercle |
| Infraspinatus | Covers posterior aspect of glenohumeral joint |
| Teres minor | Inferior to infraspinatus |
| Subscapularis tendon | Anteriorly under the deltoid and pectoralis major |
| Coracobrachialis (proximal part) | Below coracoid process |
| Short head of biceps brachii | Alongside coracobrachialis |
| Long head of biceps brachii | In the bicipital groove |
C. Nerves
| Nerve | Root | Path under Deltoid |
|---|
| Axillary nerve (most important) | C5, C6 | Exits quadrangular space, winds around surgical neck; divides into anterior (motor to deltoid and teres minor) and posterior branches (cutaneous) |
| Suprascapular nerve | C5, C6 | Passes through suprascapular notch to supply supraspinatus and infraspinatus |
| Radial nerve (partially) | C5-T1 | Exits through triangular interval to enter posterior compartment of arm |
| Lateral pectoral nerve | C5, C6, C7 | Passes through the clavipectoral fascia |
D. Blood Vessels
| Vessel | Course |
|---|
| Posterior circumflex humeral artery (from axillary a.) | Passes through quadrangular space with the axillary nerve; supplies deltoid, shoulder joint, and teres minor |
| Anterior circumflex humeral artery | Passes anterior to surgical neck |
| Deltoid branch of thoracoacromial artery | Passes in the deltopectoral groove between deltoid and pectoralis major |
| Suprascapular artery and vein | Passes under the coracoacromial ligament |
| Profunda brachii artery (partially) | Exits with radial nerve through triangular interval |
E. Bursae
| Bursa | Position | Significance |
|---|
| Subacromial (subdeltoid) bursa | Between the deltoid/acromion above and the supraspinatus tendon/joint capsule below | Reduces friction; the most clinically important bursa of the shoulder |
The subacromial bursa does not normally communicate with the joint cavity. When a full-thickness rotator cuff tear occurs, the bursa communicates with the joint space.
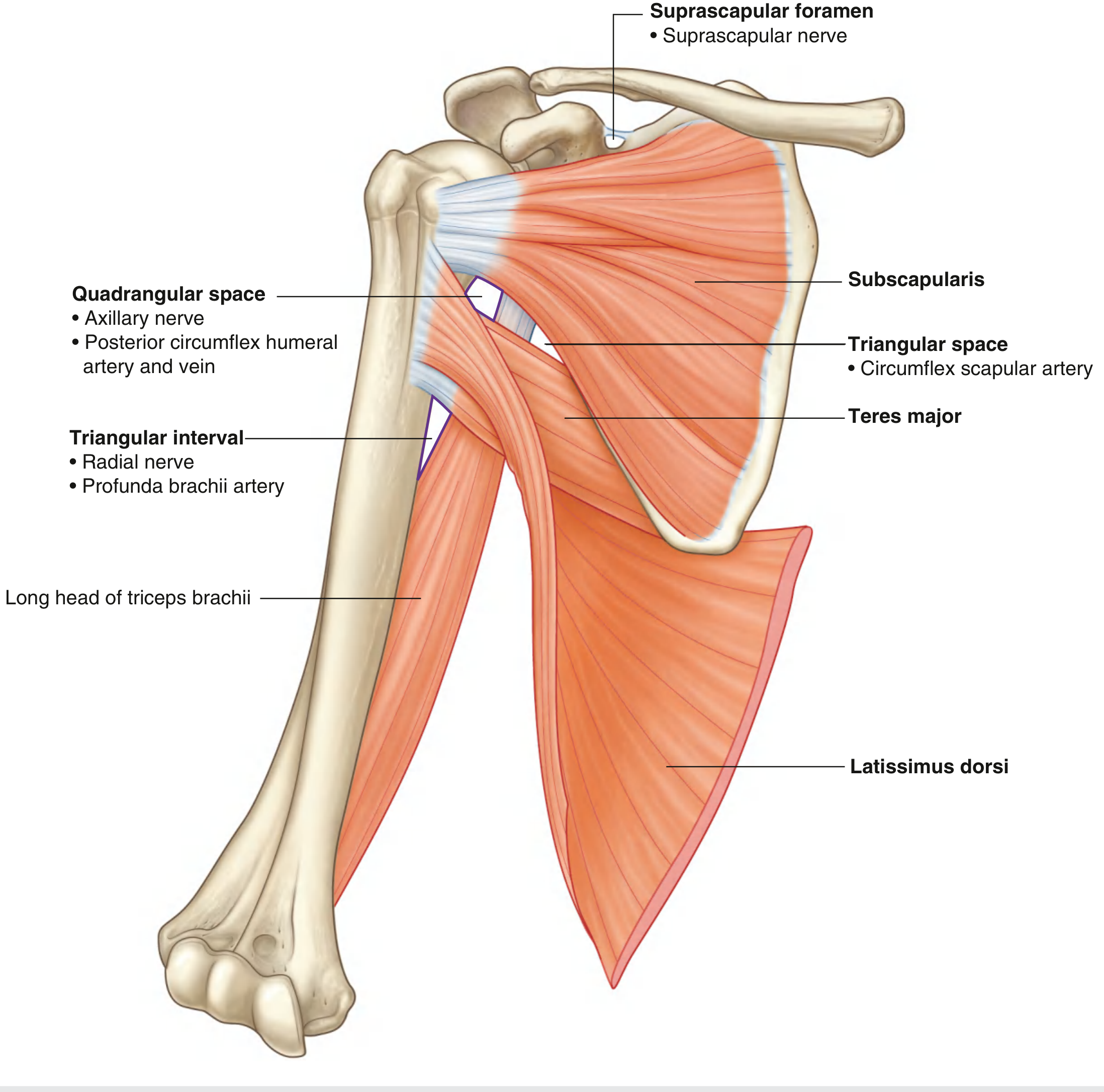
F. The Three Spaces in the Posterior Wall
These lie under the posterior part of the deltoid:
1. Quadrangular Space
- Boundaries: Teres minor (above), teres major (below), surgical neck of humerus (lateral), long head of triceps (medial)
- Contents: Axillary nerve + posterior circumflex humeral artery and vein
2. Triangular Space
- Boundaries: Teres minor (above), teres major (below), long head of triceps (lateral)
- Contents: Circumflex scapular artery and vein
3. Triangular Interval
- Boundaries: Teres major (above), long head of triceps (medial), shaft of humerus (lateral)
- Contents: Radial nerve + profunda brachii artery
Fig. 2: Posterior wall of axilla showing the three spaces and their contents
Applied Anatomy
- Anterior approach to shoulder surgery (deltopectoral approach): Incision along the deltopectoral groove (where cephalic vein runs); the deltoid is retracted to expose the rotator cuff and joint
- Quadrangular space syndrome: Compression of axillary nerve in the space causing weakness of deltoid and teres minor
- Subacromial injection: Steroid injections given into the subacromial space for rotator cuff impingement and bursitis
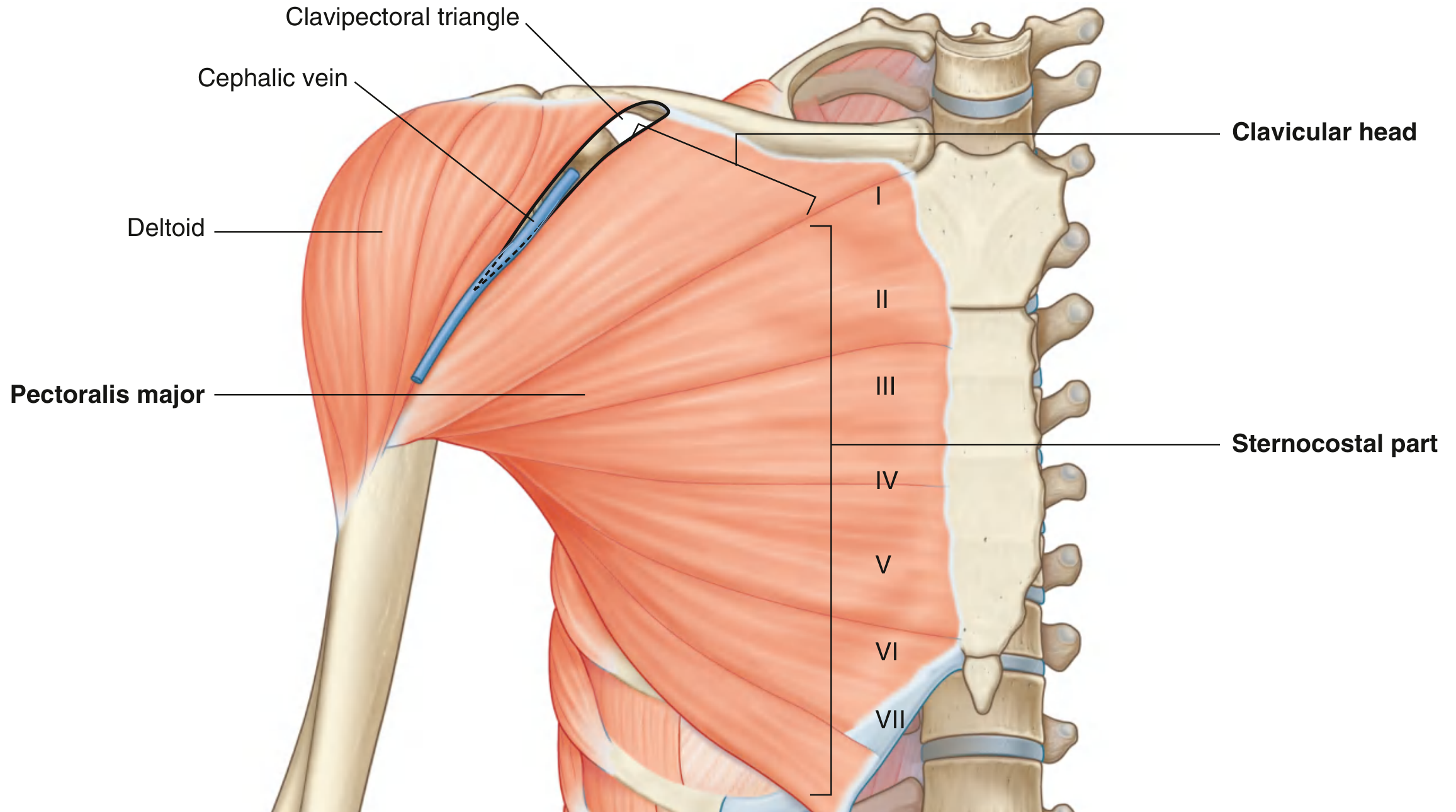
Q.4 - Attachment of Pectoralis Major Muscle [7 Marks]
Introduction
Pectoralis major is the largest and most superficial muscle of the anterior chest wall and the anterior axillary wall. It is a fan-shaped, multipennate muscle that plays major roles in shoulder movements and is also an important landmark in surgical anatomy.
Attachments
Origin - TWO Heads
1. Clavicular Head
- Anterior surface of the medial half of the clavicle
- Originates as a flat, thin fleshy sheet
2. Sternocostal (Sternal) Head
- Anterior surface of the sternum (manubrium + body) down to the level of the 6th or 7th costal cartilage
- Costal cartilages of ribs 1 to 6 (or 7)
- Aponeurosis of the external oblique muscle of the abdomen (the lower fibers form an "abdominal part")
Insertion
- Both heads converge on the humerus but form a bilaminar (two-layered) tendon:
- The tendon inserts into the lateral lip of the intertubercular sulcus (bicipital groove) of the humerus
- The clavicular head passes forward to form the anterior lamina and inserts into the lower part of the lateral lip
- The sternocostal head twists 180° upon itself so its lower fibers become the posterior lamina and insert higher on the lateral lip
- This twist means the muscle has a wide origin but a narrow, concentrated insertion
Diagram
Fig. 3: Pectoralis Major - showing clavicular and sternocostal heads and relationship to deltoid (Gray's Anatomy for Students)
Nerve Supply
| Nerve | Root | Part Supplied |
|---|
| Lateral pectoral nerve | C5, C6, C7 (from lateral cord) | Mainly clavicular head and upper sternocostal head |
| Medial pectoral nerve | C8, T1 (from medial cord) | Mainly lower sternocostal head |
Both nerves pierce the clavipectoral fascia to reach the muscle from its deep (posterior) surface.
Actions
| Action | Mechanism |
|---|
| Adduction of arm | Both heads pull the humerus toward the trunk |
| Medial rotation of arm | Pulls the lesser tubercle side forward |
| Flexion of arm | Clavicular head - raises arm from side |
| Extension of flexed arm | Sternocostal head - lowers arm from overhead position (e.g., swimming breaststroke) |
| Accessory muscle of respiration | When the arms are fixed, the sternum can be elevated to assist forced inspiration |
Test: Ask patient to adduct arm against resistance (press palm against hip) - the anterior axillary fold becomes prominent.
Relations
- Superficially: Skin, subcutaneous fat, and deep fascia; nipple lies over the 4th intercostal space
- Deep to pectoralis major: Pectoralis minor, subclavius, clavipectoral fascia, axillary vessels, and brachial plexus
- Medially: Sternum and costal cartilages
- Laterally: Deltoid muscle (the deltopectoral groove contains the cephalic vein)
Applied Anatomy
1. Anterior Axillary Fold
The lower border of pectoralis major forms the anterior axillary fold - a landmark used in examination and surgical planning.
2. Breast Anatomy and Cancer
- The breast overlies pectoralis major
- In breast cancer, the tumor may fix to the pectoralis major fascia (dimpling of skin) or the muscle itself
- Modified radical mastectomy preserves pectoralis major
3. Pectoralis Major Flap (Myocutaneous Flap)
- The pectoralis major is used as a workhorse flap in reconstructive surgery of the neck, oral cavity, and face
- Blood supply: Pectoral branch of thoracoacromial artery (dominant) + lateral thoracic artery (minor)
4. Pectoralis Major Rupture
- Rare injury; seen in weight lifters (bench press)
- The muscle tears at its humeral insertion
- The anterior axillary fold disappears and a gap is palpable
5. Nipple and Areola
The nipple lies at the level of the 4th intercostal space (in males); this is a clinical landmark for chest tube insertion.
Q.5 - Attachments, Actions and Nerve Supply of Serratus Anterior Muscle [7 Marks]
Introduction
Serratus anterior is a large, fan-shaped muscle forming the medial wall of the axilla. It is sometimes called "the boxer's muscle" because it is active in forward punching movements. It is also called the "big swing" muscle. Its nerve supply - the long thoracic nerve - is one of the most clinically important nerves to understand.
Attachments
Origin
- Lateral surfaces and upper borders of the upper 8 or 9 ribs (ribs I to IX) by separate muscular slips
- Each slip arises from a separate rib
- The slips also arise from the fascia over the intercostal spaces
- The upper two slips interdigitate with slips of origin of pectoralis minor (ribs 3, 4, 5) and the lower slips interdigitate with external oblique
Insertion
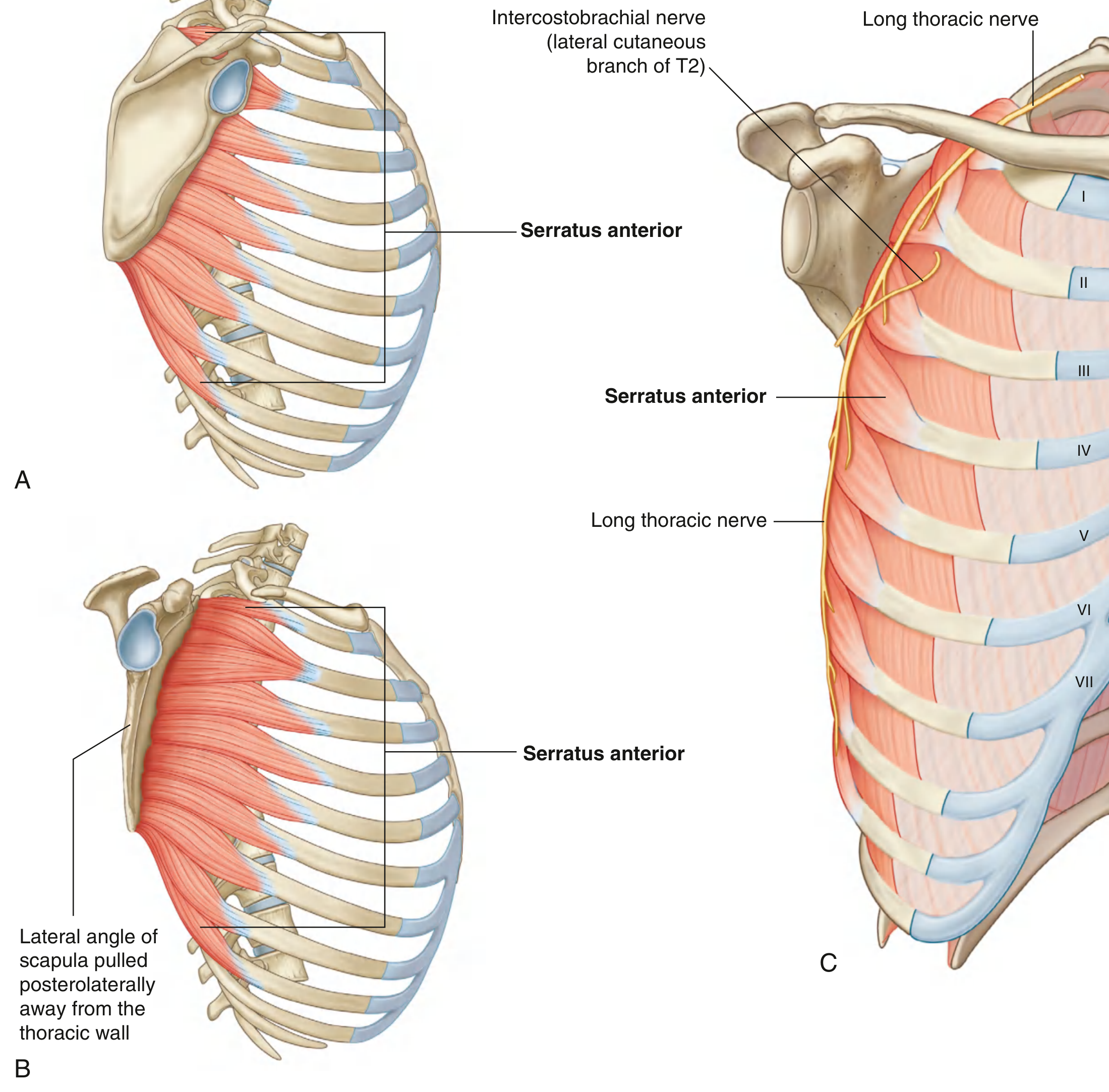
The muscle forms a flat sheet that passes posteriorly around the thoracic wall to insert on the costal (anterior) surface of the medial border of the scapula:
- Upper 2 slips (from ribs I and II): Insert on the costal surface near the superior angle of the scapula
- Middle slips (from ribs II to IV): Insert along the costal surface of the medial border
- Lower 4-5 slips (from ribs V to IX): Insert on the costal surface of the inferior angle (the largest and most important part)
Diagram
Fig. 4: Serratus Anterior. A - Lateral view. B - Scapula retracted to show muscle. C - Long thoracic nerve on external surface
Actions
| Action | Mechanism | Importance |
|---|
| Protraction (forward pulling) of scapula | Pulls the scapula around the chest wall laterally and anteriorly | Enables pushing/reaching/punching |
| Rotation of scapula (lateral rotation) | Lower fibers pull the inferior angle anterolaterally, tilting the glenoid fossa upward | Essential for arm elevation above 90° |
| Holds scapula against the chest wall | All fibers act together | Prevents winging |
| Assists in deep inspiration | When scapula is fixed (arms elevated), elevates ribs | Accessory muscle of respiration |
The lower fibers are most important - they rotate the scapula to allow full elevation of the arm above the head. Without this rotation, arm elevation is limited to 90°.
Nerve Supply
The Long Thoracic Nerve (Nerve of Bell)
| Feature | Detail |
|---|
| Root value | C5, C6, C7 (occasionally C4 contributes) |
| Origin | From the anterior rami of C5, C6, C7 (roots of brachial plexus in the neck, before trunk formation) |
| Course | Descends through the posterior triangle of neck; passes through the axillary inlet; runs vertically down the lateral thoracic wall on the external (superficial) surface of serratus anterior, just deep to the skin and superficial fascia |
| End | Reaches the 9th rib level |
| Distribution | Supplies all slips of serratus anterior |
Important: The long thoracic nerve is entirely superficial as it descends on serratus anterior - there is no deep protection. This makes it vulnerable.
Applied Anatomy
Winging of Scapula (Winged Scapula)
Cause: Paralysis of serratus anterior due to long thoracic nerve injury
Mechanism of injury to long thoracic nerve:
- Stabbing/penetrating wounds to the lateral chest wall
- Radical mastectomy (nerve lies in the axillary fat and is vulnerable)
- Carrying heavy bags on the shoulder
- First rib resection for thoracic outlet syndrome
- Viral neuritis (Parsonage-Turner syndrome)
- Poorly positioned axiillary crutches
Deformity:
- At rest: The medial border of the scapula lifts off the chest wall, giving the appearance of a "wing"
- On pushing against a wall: The medial border and inferior angle protrude prominently backward
- On attempting to elevate the arm: Patient cannot raise arm above 90° (the scapula fails to rotate)
Test for winged scapula: Ask the patient to press both hands against a wall with arms extended - the affected scapula will "wing out" prominently.
Q.6 - Boundaries and Contents of Carpal Tunnel. Explain Carpal Tunnel Syndrome [7 Marks]
Introduction
The carpal tunnel is an osseofibrous tunnel situated at the wrist, through which the median nerve and most of the long flexor tendons of the fingers pass. It is the most common site of nerve entrapment in the body.
Boundaries of the Carpal Tunnel
Roof (Anterior)
- Flexor retinaculum (transverse carpal ligament) - a thick fibrous band, approximately 2-3 cm wide and 1-2 mm thick
- It is attached:
- Medially: Pisiform and hook of hamate
- Laterally: Scaphoid tubercle and ridge of trapezium
Floor and Sides (Posterior/Lateral/Medial)
- The concave arch formed by the carpal bones:
- Lateral side: Scaphoid (tubercle) and Trapezium (ridge)
- Medial side: Pisiform and Hook of hamate
- Floor (deep): Capitate and Lunate
Contents of the Carpal Tunnel
10 structures pass through the carpal tunnel:
| Structure | Notes |
|---|
| Median nerve | Most superficial; lies just deep to flexor retinaculum; most vulnerable |
| Flexor pollicis longus tendon (1) | In its own synovial sheath (radial bursa) |
| Flexor digitorum superficialis tendons (4) | Superficial: middle finger (anterior), ring finger (posterior); index (anterior), little (posterior) |
| Flexor digitorum profundus tendons (4) | Deep, in a row |
The 8 tendons of FDS and FDP share a common synovial sheath (ulnar bursa). The FPL has a separate sheath (radial bursa). The total = 9 tendons + 1 nerve = 10 structures.
Important note: The tendon of flexor carpi radialis passes in a separate split of the retinaculum. The ulnar nerve and artery pass superficial to the retinaculum through Guyon's canal (NOT through the carpal tunnel).
Carpal Tunnel Syndrome (CTS)
Definition
CTS is a condition caused by compression of the median nerve as it passes through the carpal tunnel, producing characteristic symptoms in the median nerve distribution of the hand.
Etiology (Causes of Increased Pressure)
| Category | Examples |
|---|
| Idiopathic (most common - 50%) | Unknown; degeneration of flexor tendons synovium |
| Hormonal | Pregnancy (fluid retention), hypothyroidism, menopause |
| Inflammatory | Rheumatoid arthritis (synovial thickening), gout |
| Metabolic | Diabetes mellitus, amyloidosis, acromegaly |
| Anatomical | Abnormal muscles (palmaris profundus), ganglion in tunnel |
| Occupational | Repetitive wrist flexion/extension (keyboard use, mechanics) |
| Trauma | Colles' fracture (malunion), wrist edema post injury |
Pathophysiology
- Any condition that reduces the capacity of the tunnel or increases the volume of contents → increased pressure within the tunnel
- Pressure impairs venous return → intraneural edema → further pressure
- Ischemia of the median nerve → demyelination → sensory then motor changes
- Chronic cases → axonal degeneration → wasting (irreversible)
Clinical Features
Symptoms (Sensory - earliest)
- Pain, tingling (paresthesia), and numbness in the thumb, index finger, middle finger, and lateral half of ring finger (median nerve territory)
- Nocturnal symptoms (waking at night with hand pain/tingling) - classic presenting symptom; due to venous stasis when lying flat
- Relief of symptoms by hanging the arm out of bed or shaking the wrist
Signs (Motor - later)
- Weakness of thenar muscles: Difficulty opposing thumb (pinching/gripping objects)
- Wasting of thenar eminence - in chronic/severe cases
- Ape thumb (simian) deformity: Thumb lies in the plane of the palm due to loss of opposition/abduction
Distribution of Sensory Loss
- The palmar cutaneous branch of the median nerve (which arises before entering the carpal tunnel and passes over the retinaculum) → sensation of the lateral part of the palm is PRESERVED in CTS
Special Clinical Tests
| Test | Method | Positive Result |
|---|
| Tinel's sign | Tap over the carpal tunnel at the wrist | Tingling in median nerve distribution |
| Phalen's test | Both wrists fully flexed for 60 seconds | Reproduction of symptoms |
| Reverse Phalen's | Wrists fully extended for 60 seconds | Symptoms reproduced |
| Compression test | Direct pressure over the carpal tunnel | Symptoms in < 30 seconds |
Investigations
- Nerve conduction studies (NCS): Gold standard - shows slowing of conduction velocity at wrist
- Electromyography (EMG): Shows denervation in thenar muscles in severe cases
- Ultrasound: Shows enlarged median nerve at tunnel entrance
Treatment
| Stage | Treatment |
|---|
| Mild/Moderate | Splinting (cock-up splint, neutral position - especially at night); NSAIDs; activity modification |
| Moderate | Corticosteroid injection into the carpal tunnel (relief in 80%, but may recur) |
| Severe / Unresponsive | Surgical decompression - division of the flexor retinaculum (either open or endoscopic); most effective, 90% success rate |
Q.7 - Specify the Nerve Supply and Actions of Interossei of the Hand [7 Marks]
Introduction
The interossei are short muscles of the hand located between the metacarpals. They form two groups - palmar (volar) and dorsal - and are key to fine motor movements of the fingers. Along with the lumbricals, they are the principal intrinsic muscles controlling the "intrinsic plus" position of the fingers.
Classification
| Feature | Palmar Interossei | Dorsal Interossei |
|---|
| Number | 4 (some texts say 3, excluding 1st) | 4 |
| Location | On the palmar aspect of metacarpals | Between metacarpals |
| Morphology | Unipennate (one head) | Bipennate (two heads = from adjacent sides of two metacarpals) |
| Main action | PAD - Palmar ADduct toward middle finger | DAB - Dorsal ABduct away from middle finger |
Nerve Supply
ALL interossei (both palmar and dorsal) are supplied by the deep branch of the ulnar nerve (C8, T1)
- The deep branch of the ulnar nerve enters the hand by passing lateral to the pisiform, through the hypothenar muscles, and sweeps across the palm deep to the long flexor tendons to supply all interossei
- Root value: C8, T1
Palmar Interossei (4 muscles - PAD)
The axis for abduction/adduction of fingers is through the middle finger (3rd digit).
| Muscle | Origin | Insertion | Action |
|---|
| 1st Palmar | Ulnar (medial) side of 1st metacarpal | Ulnar side of proximal phalanx of thumb | Adducts thumb toward middle |
| 2nd Palmar | Ulnar (medial) side of 2nd metacarpal | Ulnar side of proximal phalanx of index | Adducts index toward middle |
| 3rd Palmar | Radial (lateral) side of 4th metacarpal | Radial side of proximal phalanx of ring | Adducts ring toward middle |
| 4th Palmar | Radial (lateral) side of 5th metacarpal | Radial side of proximal phalanx of little | Adducts little toward middle |
Note: The middle finger has NO palmar interosseous because it is the axis itself
Dorsal Interossei (4 muscles - DAB)
| Muscle | Origin (bipennate) | Insertion | Action |
|---|
| 1st Dorsal | Adjacent sides of 1st & 2nd metacarpals | Radial side of index finger | Abducts index to radial side |
| 2nd Dorsal | Adjacent sides of 2nd & 3rd metacarpals | Radial side of middle finger | Abducts middle to radial side |
| 3rd Dorsal | Adjacent sides of 3rd & 4th metacarpals | Ulnar side of middle finger | Abducts middle to ulnar side |
| 4th Dorsal | Adjacent sides of 4th & 5th metacarpals | Ulnar side of ring finger | Abducts ring to ulnar side |
Note: The middle finger has TWO dorsal interossei (can abduct in two directions)
Common Actions of ALL Interossei
In addition to abduction/adduction:
- Flexion of the metacarpophalangeal (MCP) joints - by their proximal attachment on the bases of proximal phalanges
- Extension of the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints - by their distal attachment into the extensor (dorsal) expansion/hood
This combined action (MCP flexion + IP extension) is the "intrinsic plus" position - critical for precision grip.
Insertion into Extensor Hood
All interossei insert into the dorsal (extensor) digital expansion (extensor hood) of the corresponding finger. This expansion is a complex tendinous hood that covers the dorsum of the proximal phalanx. When the interossei contract, they:
- Pull the proximal phalanx into flexion at the MCP
- Through the hood, extend the IP joints
- This is the basis of the Bouchard test and the clinical hand position
Applied Anatomy
1. Froment's Sign (tests 1st dorsal interosseous / adductor pollicis)
- Ask the patient to hold a piece of paper between the thumb and index finger
- Normally, the adductor pollicis (ulnar nerve) holds it with the IP joints straight
- In ulnar nerve palsy: the patient compensates by flexing the IP joint of the thumb (using FPL - median nerve) = positive Froment's sign
2. Ulnar Nerve Palsy - Effects on Interossei
When the ulnar nerve (deep branch) is injured, all interossei are paralyzed, causing:
| Effect | Mechanism |
|---|
| Claw hand (ring and little primarily) | MCP hyperextension (unbalanced extensors) + IP flexion (unbalanced FDP) |
| Loss of finger abduction/adduction | No interossei or hypothenar function |
| Positive card test | Cannot hold a card between adjacent fingers |
| Wasting of first dorsal interosseous | Most visible between thumb and index finger webspace |
| Weak grip | Loss of MCP flexor (intrinsic) component |
3. Rheumatoid Arthritis (RA)
- Synovitis causes stretching of the extensor hood
- Interossei may sublux, leading to boutonniere deformity (PIP flexion + DIP extension) or swan neck deformity (PIP hyperextension)
Q.8 - Draw and Explain the Diagram of Brachial Plexus [7 Marks]
Introduction
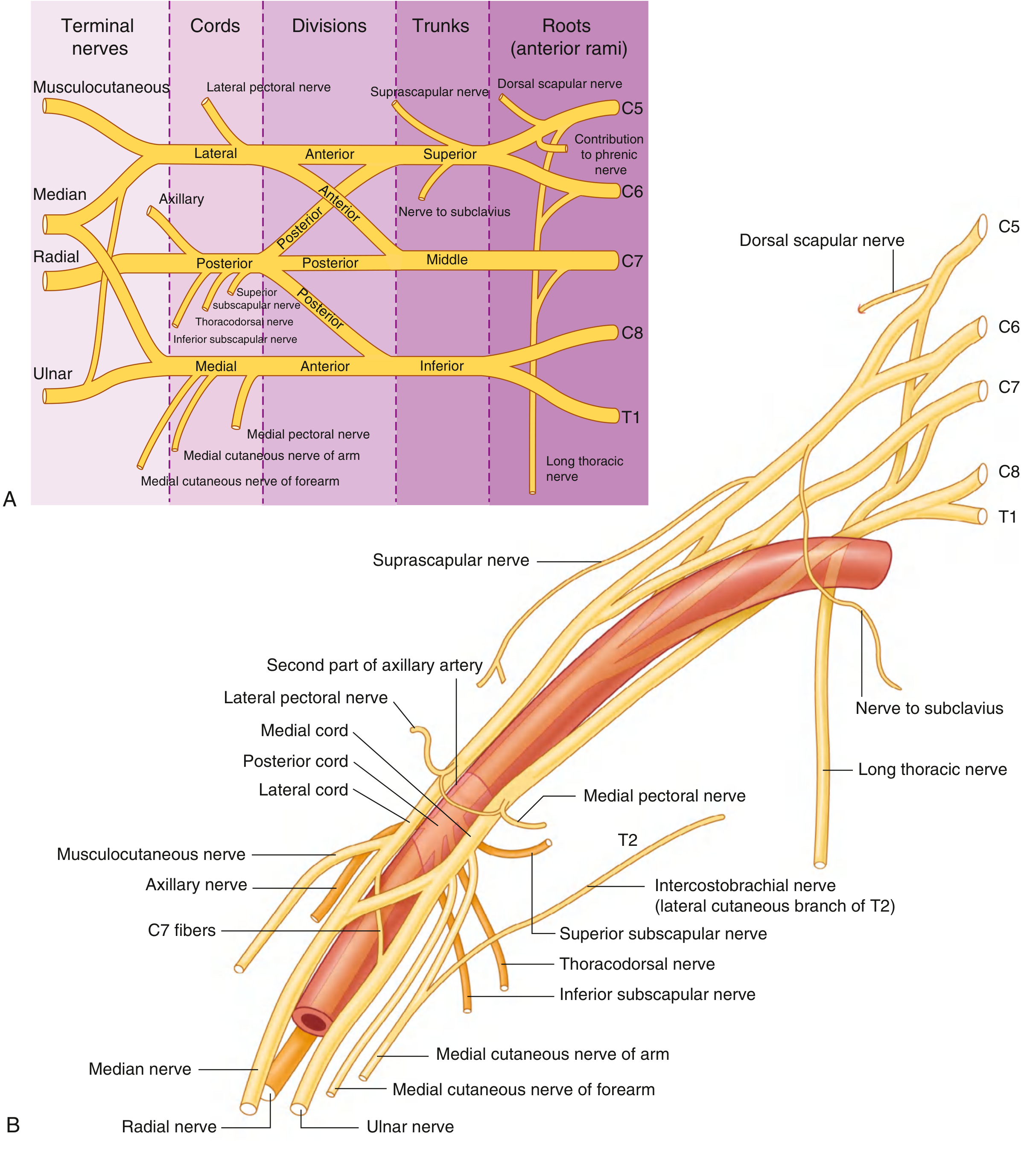
The brachial plexus is a somatic nerve network formed by the anterior rami of spinal nerves C5, C6, C7, C8, and T1 (with variable contributions from C4 and T2). It is the sole neural supply to the entire upper limb (except the T2 intercostobrachial nerve contribution to skin). All major upper limb nerves arise from it.
Diagrams
Fig. 5A: Brachial Plexus - anatomy in the neck and axilla
Fig. 5B: Complete schematic of brachial plexus with all branches (Gray's Anatomy for Students)
Components (Mnemonic: "Really Tired? Drink Cold Beer" = Roots, Trunks, Divisions, Cords, Branches)
1. ROOTS (5 Roots: C5, C6, C7, C8, T1)
- Located: Between the anterior scalene and middle scalene muscles in the neck (scalene triangle)
- Receive gray rami communicantes from the sympathetic trunk
Branches from Roots:
| Branch | Root | Supplies |
|---|
| Dorsal scapular nerve | C5 | Rhomboid major, rhomboid minor, levator scapulae |
| Long thoracic nerve | C5, C6, C7 | Serratus anterior |
| Phrenic nerve contribution | C5 | Diaphragm (partially) |
2. TRUNKS (3 Trunks)
Formed as the roots emerge from between the scalene muscles and cross the posterior triangle of the neck:
| Trunk | Formation | Position |
|---|
| Superior (upper) trunk | C5 + C6 join | Above the subclavian artery |
| Middle trunk | C7 alone continues | Posterior to subclavian artery |
| Inferior (lower) trunk | C8 + T1 join | On rib I, behind subclavian artery |
Branches from Superior Trunk:
| Branch | Supplies |
|---|
| Suprascapular nerve (C5, C6) | Supraspinatus + infraspinatus |
| Nerve to subclavius (C5, C6) | Subclavius muscle |
3. DIVISIONS (6 Divisions - NO branches arise)
Each trunk splits into an anterior division and a posterior division:
- Anterior divisions = will ultimately supply FLEXOR compartments
- Posterior divisions = will supply EXTENSOR compartments
4. CORDS (3 Cords, named by relationship to the 2nd part of axillary artery)
| Cord | Formation | Position | Root Values |
|---|
| Lateral cord | Anterior divisions of superior + middle trunks | Lateral to axillary artery | C5, C6, C7 |
| Medial cord | Anterior division of inferior trunk alone | Medial to axillary artery | C8, T1 |
| Posterior cord | All 3 posterior divisions together | Posterior to axillary artery | C5 to T1 |
Branches from Cords:
From Lateral Cord (C5-C7):
| Branch | Supplies |
|---|
| Lateral pectoral nerve | Pectoralis major (clavicular head) |
| Musculocutaneous nerve | Coracobrachialis, biceps, brachialis; lateral forearm skin |
| Lateral root of median nerve | (combines with medial root) |
From Medial Cord (C8, T1):
| Branch | Supplies |
|---|
| Medial pectoral nerve | Pectoralis major (sternocostal) + minor |
| Medial cutaneous nerve of arm | Medial skin of arm |
| Medial cutaneous nerve of forearm | Medial skin of forearm |
| Ulnar nerve | Most intrinsic hand muscles; 1.5 fingers sensation |
| Medial root of median nerve | (combines with lateral root) |
From Posterior Cord (C5-T1):
| Branch | Supplies |
|---|
| Upper subscapular nerve | Subscapularis (upper) |
| Thoracodorsal nerve | Latissimus dorsi |
| Lower subscapular nerve | Subscapularis (lower) + teres major |
| Axillary nerve (C5, C6) | Deltoid, teres minor; shoulder capsule sensation |
| Radial nerve (C5-T1) | All extensors of arm and forearm; skin of posterior arm/forearm/hand |
Median nerve = Lateral root (C5, C6, C7) + Medial root (C8, T1)
5. TERMINAL BRANCHES (5 Main Nerves)
| Nerve | Origin | Main Distribution |
|---|
| Musculocutaneous | Lateral cord | Anterior arm muscles; lateral forearm skin |
| Median | Both lateral and medial cords | Anterior forearm; thenar eminence; lateral 3½ digits |
| Ulnar | Medial cord | Intrinsic hand muscles; medial 1½ digits |
| Radial | Posterior cord | All extensors; posterior arm/forearm/hand skin |
| Axillary | Posterior cord | Deltoid, teres minor; shoulder skin |
Applied Anatomy - Brachial Plexus Injuries
| Level | Injury | Cause | Deformity |
|---|
| Upper (C5, C6) | Erb-Duchenne palsy | Shoulder depression in labor/trauma | "Waiter's tip" |
| Lower (C8, T1) | Klumpke's palsy | Hyperabduction of shoulder | Claw hand + Horner's |
| Complete plexus | Entire limb flail | Avulsion in high-speed trauma | Total paralysis |
Q.9 - Explain the Anatomical Basis of Deformity of Erb's Paralysis [7 Marks]
Introduction
Erb's (Erb-Duchenne) paralysis is an upper brachial plexus injury involving the C5 and C6 nerve roots (and occasionally C7). It is the most common type of brachial plexus injury (approximately 90% of cases). The injury occurs at "Erb's point" - the site where the C5 and C6 roots join to form the upper trunk of the brachial plexus, located 2-3 cm above the clavicle in the neck.
Mechanism of Injury
The injury occurs due to excessive widening of the angle between the neck and the shoulder:
In Neonates (Obstetric Erb's palsy):
- Difficult labor with shoulder dystocia
- Forceps traction on the head during shoulder presentation
- The shoulder is pushed down and the head pulled away - tearing C5, C6 roots
In Adults:
- Motorcycle accidents (fall on outstretched arm with head forced away)
- Fall from a horse (shoulder hits the ground, head forced sideways)
- Carrying heavy loads on shoulders
- Direct blow depressing the shoulder
Muscles Affected (C5 and C6 supplied muscles)
| Muscle | Action Lost |
|---|
| Deltoid (axillary nerve C5, C6) | Abduction of arm |
| Supraspinatus (suprascapular C5, C6) | Initiation of abduction |
| Infraspinatus (suprascapular C5, C6) | Lateral rotation of arm |
| Teres minor (axillary C5, C6) | Lateral rotation |
| Biceps brachii (musculocutaneous C5, C6) | Flexion at elbow; supination |
| Brachialis (musculocutaneous C5, C6) | Flexion at elbow |
| Brachioradialis (radial C5, C6) | Flexion in mid-prone position |
| Supinator (radial C6) | Supination of forearm |
The Classic Deformity: "Waiter's Tip" / "Policeman Receiving a Tip"
The deformity results from paralysis of certain muscles and unopposed action of their antagonists:
| Action Lost (Muscle Paralyzed) | Unopposed Antagonist Action | Resulting Position |
|---|
| Abduction (deltoid + supraspinatus) | Adductors: pectoralis major, latissimus dorsi | Arm adducted against side |
| Lateral rotation (infraspinatus + teres minor) | Medial rotators: subscapularis, pectoralis major, latissimus | Arm medially rotated |
| Flexion at elbow (biceps + brachialis) | Extensors: triceps | Elbow extended |
| Supination (biceps + supinator) | Pronators: pronator teres, pronator quadratus | Forearm pronated |
| Wrist extension (brachioradialis impaired) | Wrist flexors (intact) | Wrist in slight flexion |
The result: The limb hangs at the side, adducted, medially rotated, elbow extended, forearm pronated, wrist flexed - "waiter's tip" or "policeman receiving a tip" posture.
Sensory Loss
- Over the lateral aspect of the upper arm (axillary nerve territory - C5)
- Over the lateral forearm (musculocutaneous nerve territory - C6)
- A strip along the radial side of the forearm and dorsum of hand
Reflexes Affected
- Biceps reflex (C5, C6): Absent
- Brachioradialis (supinator) reflex (C5, C6): Absent
- Triceps reflex (C7) and finger reflexes (C8) intact
Erb's Point
- The junction of C5 and C6 roots to form the upper trunk
- Located ~2-3 cm above the clavicle, posterior to the sternocleidomastoid
- Stimulation of this point (electrical or surgical) causes all the muscles listed above to respond
Differentiation from Klumpke's Palsy
| Feature | Erb's Palsy (C5, C6) | Klumpke's Palsy (C8, T1) |
|---|
| Mechanism | Shoulder depression / head tilt | Hyperabduction of shoulder |
| Obstetric cause | Shoulder dystocia | Breech with arms overhead |
| Deformity | "Waiter's tip" | Claw hand |
| Sensory loss | Lateral arm + forearm | Medial forearm + ulnar hand |
| Horner's syndrome | Absent | Present (T1 sympathetic fibers) |
| Reflexes lost | Biceps, brachioradialis | Finger reflexes |
Prognosis and Treatment
- Obstetric Erb's palsy: Most cases recover spontaneously within 3-6 months if nerve is neuropraxic (not avulsed)
- Physiotherapy to prevent contractures during recovery
- Surgical treatment (nerve grafting, neurolysis) if no improvement by 3-6 months
- Avulsion injuries (nerve pulled from spinal cord) are irreparable
Q.10 - Pronation and Supination [7 Marks]
Definitions
- Supination: Rotation of the forearm so the palm faces anteriorly (in anatomical position) or upward. The radius lies parallel to the ulna. The word "supination" comes from "supine" (lying on back).
- Pronation: Rotation of the forearm so the palm faces posteriorly or downward. The radius crosses obliquely over the ulna. "Prone" = face down.
Joints Involved
Pronation and supination involve two joints acting simultaneously:
1. Proximal Radio-Ulnar Joint
- Type: Pivot (trochoidal) synovial joint
- Articulation: The head of radius rotates within the fibro-osseous ring formed by the radial notch of the ulna and the anular ligament
- The head of radius spins within this ring
2. Distal Radio-Ulnar Joint
- Type: Pivot synovial joint
- Articulation: The concave surface of the ulnar notch of the radius rotates around the head of the ulna
- The radius swings around the stationary ulna
The interosseous membrane (fibroelastic membrane between the shafts of radius and ulna) transmits forces between the two bones and maintains their relationship.
Movement Summary
- Supination: Radius rotates laterally → becomes parallel to ulna
- Pronation: Lower end of radius rotates medially → crosses over the ulna
Muscles of Supination
| Muscle | Nerve | Root | Additional Notes |
|---|
| Supinator (principal) | Deep branch of radial nerve (posterior interosseous) | C6 | Acts in all positions; more efficient when elbow extended |
| Biceps brachii (most powerful when elbow flexed at 90°) | Musculocutaneous nerve | C5, C6 | Most powerful supinator when resistance is needed; the tendon wraps around the radial tuberosity during supination |
Test: Screwing a screw into wood (clockwise for right-handed person) uses powerful supination (biceps). Compare with the power of turning a corkscrew.
Muscles of Pronation
| Muscle | Nerve | Root | Action |
|---|
| Pronator teres (principal) | Median nerve | C6, C7 | Pronates and assists in elbow flexion; two heads: humeral and ulnar |
| Pronator quadratus (distal; acts throughout) | Anterior interosseous nerve (median nerve branch) | C7, C8 | Initiates and maintains pronation; at distal forearm |
| Brachioradialis (assists, returns from full supination or full pronation to midprone) | Radial nerve | C5, C6 | Weak pronation from full supination position only |
Range of Movement
- Supination: 0° to approximately 85-90°
- Pronation: 0° to approximately 75-80°
- Combined range of ~170° at the radioulnar joints
The "Combined Movement" at the Elbow
The elbow and forearm work together:
- When making a fist and supinating against resistance (like using a screwdriver), the biceps does most of the work
- When gravity-assisted pronation is needed (putting a plate down), pronator quadratus acts
Applied Anatomy
1. Fractures and Deformity
| Fracture Level | Deformity |
|---|
| Fracture of radius above pronator teres insertion | Proximal fragment is supinated (by biceps and supinator); distal fragment is pronated (by pronator teres) |
| Fracture of radius below pronator teres | Less deformity as pronators and supinators balance each other |
| Monteggia fracture-dislocation | Fracture of the ulnar shaft + dislocation of the radial head; the interosseous membrane is disrupted; radial nerve may be injured |
2. Pronator Teres Syndrome
- Compression of the median nerve between the two heads of pronator teres
- Presents similarly to carpal tunnel syndrome but with forearm pain on resisted pronation
- Differentiated from CTS by the presence of forearm pain and absence of nocturnal symptoms
3. Posterior Interosseous Nerve (PIN) Compression
- The deep branch of the radial nerve passes through the two heads of the supinator (the "arcade of Frohse")
- Compression here causes weakness of finger extension without wrist drop (ECRL intact)
4. Clinical Test for Pronation/Supination
- Test with elbow fixed at 90° to eliminate shoulder rotation
- Note that the humerus must not rotate during the test (fix by pressing elbow against body)
5. Isolated Radial Head Fracture
- The most common elbow fracture in adults
- Causes painful limitation of pronation and supination
- Treated conservatively if undisplaced; radial head excision if comminuted
Q.11 - Median Nerve in the Hand and Forearm [7 Marks]
Root Value and Formation
- Root value: C6, C7, C8, T1 (sometimes C5)
- Formation: From the union of two roots:
- Lateral root (C6, C7) from the lateral cord
- Medial root (C8, T1) from the medial cord
- These unite in front of (anterior to) the 3rd part of the axillary artery to form the median nerve
Course in the Arm
- Enters the arm at the inferior margin of teres major
- Initially lies lateral to the brachial artery in the proximal arm
- Crosses the brachial artery at mid-arm to lie medial to it in the distal arm
- No motor branches in the arm
- Enters the cubital fossa lying medial to the brachial artery
Course in the Forearm
- Passes between the two heads of pronator teres (humeral head and ulnar head) - the first muscular branch here
- Passes deep to the fibrous arch of flexor digitorum superficialis (FDS bridge)
- Descends between FDS (superficially) and FDP + FPL (deep)
- Gives off the anterior interosseous nerve (AIN) just below the elbow
- About 5 cm above the wrist, the palmar cutaneous branch arises (passes superficial to the retinaculum - this branch is NOT compressed in CTS)
- Crosses the wrist lying between the tendon of FDS (medially) and FCR (laterally), just lateral to palmaris longus
Branches in the Forearm
Direct Muscular Branches (all "surface" flexors except FCU and medial FDP):
| Muscle | Supply |
|---|
| Pronator teres | C6, C7 |
| Flexor carpi radialis | C6, C7 |
| Palmaris longus | C7, C8 |
| Flexor digitorum superficialis | C7, C8, T1 |
Anterior Interosseous Nerve (AIN)
The AIN arises from the posterior aspect of the median nerve 5-8 cm below the lateral epicondyle. It runs with the anterior interosseous artery on the interosseous membrane:
| Muscle | Action |
|---|
| Flexor pollicis longus | Flexes thumb IP joint |
| Lateral half of flexor digitorum profundus (index + middle) | Flexes DIP of index and middle fingers |
| Pronator quadratus | Pronates forearm |
Palmar Cutaneous Branch
- Arises 5 cm above the wrist from the radial side of the median nerve
- Passes superficial (not through) the flexor retinaculum
- Supplies skin over the thenar eminence and lateral palm
- This branch is NOT compressed in carpal tunnel syndrome → sensory over lateral palm is preserved in CTS
Course in the Hand
- Passes through the carpal tunnel (deep to the flexor retinaculum)
- Immediately distal to the retinaculum it divides into:
Recurrent (Thenar) Branch (Motor - most important)
- Arises from the radial side of the median nerve just distal to the retinaculum
- Recurves back and enters the thenar eminence
- Supplies the three thenar muscles
| Thenar Muscle | Function |
|---|
| Abductor pollicis brevis | Abducts thumb in a plane perpendicular to palm |
| Opponens pollicis | Rotates first metacarpal medially; most important for pinch/grip |
| Flexor pollicis brevis (lateral/superficial head) | Flexes thumb MCP |
Palmar Digital Nerves (Sensory + Motor to lumbricals)
| Distribution | Notes |
|---|
| Thumb (both sides) | Via two proper digital nerves |
| Index finger (both sides) | Via common palmar digital nerve |
| Middle finger (both sides) | Via common palmar digital nerve |
| Ring finger (lateral half) | Via common palmar digital nerve |
| 1st lumbrical | Branch from digital nerve to index |
| 2nd lumbrical | Branch from digital nerve to middle |
Diagram (Course and Branches)
Fig. 6: Nerves of the arm showing median nerve course alongside brachial artery
Summary: Complete Muscles Supplied
| Region | Muscles Innervated |
|---|
| Forearm | Pronator teres, FCR, palmaris longus, FDS, FPL, lateral FDP (index + middle), pronator quadratus |
| Hand (thenar) | Abductor pollicis brevis, Opponens pollicis, Lateral FPB |
| Hand (lumbricals) | 1st and 2nd lumbricals |
Applied Anatomy - Effects of Median Nerve Injury
High Lesion (at the elbow - e.g., supracondylar fracture in children):
- All forearm muscles (above) paralyzed
- "Pronator sign": Unable to pronate against resistance
- "Pen test": Cannot flex the DIP of index finger (FDP lateral half paralyzed) or IP of thumb (FPL paralyzed) - demonstrates AIN injury
- Loss of opposition of thumb
- Sensory loss over lateral 3½ digits and lateral palm
- "Pointing index" when making a fist (due to FDP lateral half paralysis)
Low Lesion (at the wrist - Carpal Tunnel Syndrome):
- Thenar wasting
- Loss of opposition of thumb
- "Ape thumb" or "simian thumb" deformity
- Sensory loss over lateral 3½ digits (NOT the lateral palm - palmar cutaneous branch is spared)
- Power of forearm flexors preserved
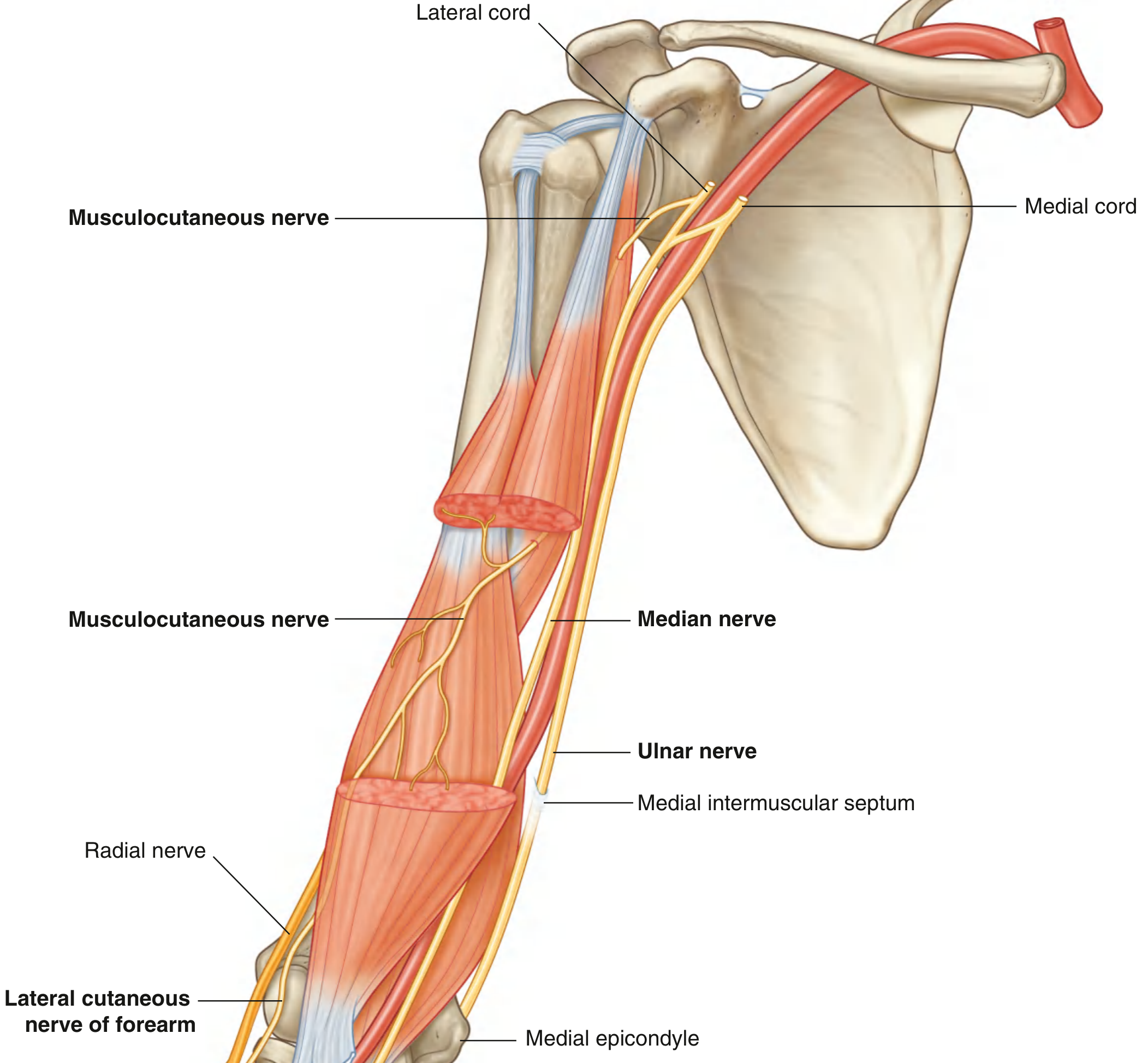
Q.12 - Musculocutaneous Nerve [7 Marks]
Introduction
The musculocutaneous nerve is the principal nerve of the anterior compartment of the arm. It supplies all three muscles of the anterior arm and provides sensation to the lateral forearm. It is relatively rarely injured in isolation due to its deep location.
Root Value
C5, C6 (and frequently C7)
Origin
- Arises as the terminal branch of the lateral cord of the brachial plexus
- Originates in the axilla, at the level of the lower border of the pectoralis minor
Course
In the Axilla:
- Arises from the lateral cord of the brachial plexus
- Passes laterally, lying anterior to the axillary artery
In the Arm:
- Pierces the coracobrachialis muscle (which it innervates as it passes through)
- Passes obliquely downward between the biceps brachii (anteriorly) and the brachialis (posteriorly)
- Supplies motor branches to biceps brachii and brachialis as it passes between them
- Emerges at the lateral border of the biceps brachii tendon, just proximal to the elbow
Terminal Branch:
- Passes through the deep fascia and continues as the lateral cutaneous nerve of the forearm
Diagram
Fig. 7: Musculocutaneous nerve in the arm (Gray's Anatomy for Students)
Branches and Distribution
1. Branch to Coracobrachialis (C5, C6, C7)
- Arises as the nerve enters or pierces coracobrachialis
- Supplies the coracobrachialis muscle
2. Branches to Biceps Brachii (C5, C6)
- Several branches given off as the nerve passes between biceps and brachialis
- Supplies both heads of biceps brachii
3. Branches to Brachialis (C5, C6)
- Branches given to the bulk of the brachialis as the nerve descends
- Note: The lateral part of brachialis is also supplied by the radial nerve (C6) - the only flexor supplied by the radial nerve
4. Articular Branch
- Small branches to the elbow joint
5. Lateral Cutaneous Nerve of the Forearm (sensory terminal)
- Passes through the deep fascia lateral to the biceps tendon at the elbow
- Divides into anterior and posterior branches:
- Anterior branch: Supplies the anterior (volar) surface of the lateral forearm as far as the thenar eminence
- Posterior branch: Supplies the posterior (dorsal) surface of the lateral forearm
Summary of Muscles Supplied
| Muscle | Action Produced | Notes |
|---|
| Coracobrachialis | Flexion and adduction of arm at shoulder | Arises from coracoid process; inserts on mid-medial humerus |
| Biceps brachii | Flexion at elbow (most powerful when supinated); Supination of forearm; Weak flexion at shoulder | Two heads (long = supraglenoid tubercle; short = coracoid process); inserts on radial tuberosity |
| Brachialis | Pure flexion at elbow (cannot supinate or pronate) - the "workhorse flexor" | Inserts on ulnar tuberosity; always working regardless of forearm rotation |
Sensory Distribution
The lateral cutaneous nerve of the forearm supplies skin on the lateral aspect of the forearm - both anterior and posterior surfaces - from the elbow to the wrist and extending to the thenar eminence.
Applied Anatomy
1. Injury to Musculocutaneous Nerve
Causes:
- Penetrating injuries to the arm
- Dislocation of the shoulder (rare)
- Violent arm movement in sports (arm wrestling injury)
- Compression from prolonged hyperabduction (surgery)
Effects:
- Weakness of elbow flexion (brachialis, biceps) - particularly with the forearm supinated
- Loss of supination (biceps is the main supinator)
- Loss of biceps reflex (C5, C6) - important clinical sign
- Sensory loss over the lateral forearm (lateral cutaneous nerve of forearm)
- The coracobrachialis is paralyzed (but clinically not noticed much)
2. Clinical Testing
- Motor: Flex elbow against resistance with forearm supinated (biceps); flex elbow in mid-prone position (brachialis)
- Reflex: Biceps jerk (C5, C6) will be absent
- Sensory: Test the lateral forearm
3. Distinction from C5-C6 Root Lesion
| Feature | Musculocutaneous injury | C5-C6 root lesion |
|---|
| Deltoid | Normal | Paralyzed |
| Rhomboids | Normal | Paralyzed |
| Infraspinatus | Normal | Paralyzed |
| Elbow flexion | Paralyzed | Paralyzed |
| Biceps reflex | Absent | Absent |
| Sensory loss | Lateral forearm only | More extensive |
4. Coracobrachialis as a Landmark
The musculocutaneous nerve must be identified and protected during anterior approaches to the shoulder, as it pierces coracobrachialis - dividing this muscle without protecting the nerve causes biceps/brachialis weakness.
Q.13 - Specify the Origin, Insertion and Distribution of Radial Nerve [7 Marks]
(See also Q.14 for clinical anatomy - these two questions overlap significantly)
Root Value and Origin
- Root value: C5, C6, C7, C8, T1
- Origin: Arises as the terminal branch of the posterior cord of the brachial plexus
- It is the largest branch of the brachial plexus and the principal nerve of the extensor compartments
Course and Distribution
1. In the Axilla
- Lies posterior to the axillary artery
- Passes with the profunda brachii artery toward the triangular interval
2. In the Arm - Posterior Compartment
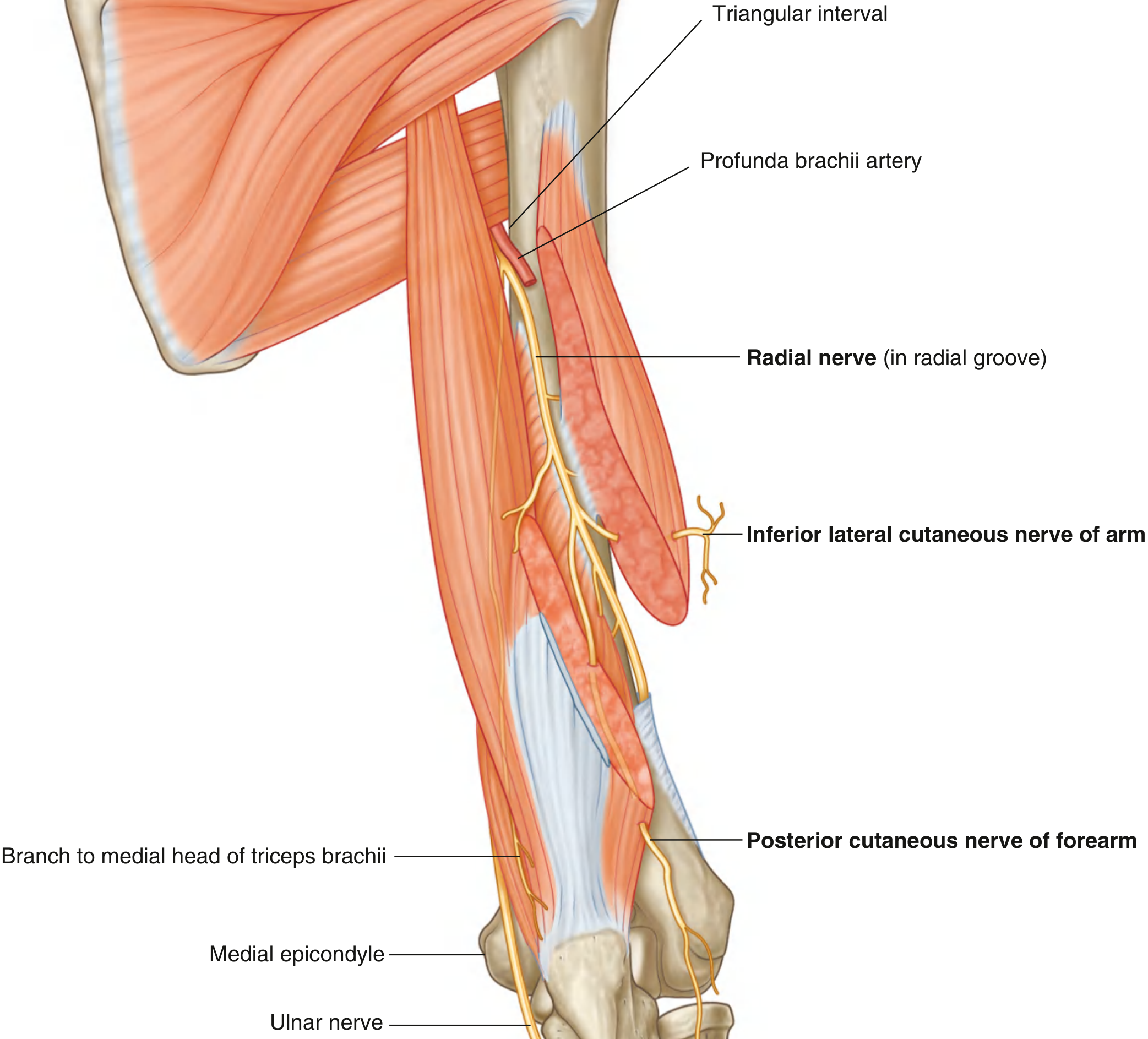
Enters posterior compartment via the triangular interval (bounded by teres major above, shaft of humerus laterally, long head of triceps medially):
- Lies in the radial groove (spiral groove) on the posterior surface of the humerus - in direct contact with bone
- Accompanied by the profunda brachii artery
- Travels diagonally from medial to lateral
Branches in the arm:
| Branch | Supplies |
|---|
| Muscular: medial head of triceps (before triangular interval) | Extension of forearm |
| Muscular: lateral and long heads of triceps | Extension of forearm |
| Muscular: anconeus | Assists elbow extension |
| Inferior lateral cutaneous nerve of arm | Skin of lower lateral arm |
| Posterior cutaneous nerve of forearm | Skin of posterior forearm |
3. At the Lateral Epicondyle
The radial nerve enters the anterior compartment by piercing the lateral intermuscular septum, then lies between brachialis (medially) and brachioradialis (laterally) in the cubital fossa.
Branches before dividing:
| Branch | Supplies |
|---|
| Brachioradialis | Flexion of elbow in mid-prone position |
| Extensor carpi radialis longus (ECRL) | Extension + radial deviation of wrist |
| Part of brachialis (lateral) | Elbow flexion |
Division into two terminal branches (at or just below the level of the lateral epicondyle):
4. Superficial Branch (Purely Sensory)
- Passes deep to brachioradialis, descending lateral to the radial artery
- Emerges at the wrist between brachioradialis and ECRL, winds around the radius
- Supplies: Skin of the dorsal lateral hand, dorsum of lateral 3½ digits (proximal phalanges and parts of middle phalanges of thumb, index, middle, lateral ring fingers)
- The first dorsal webspace (between thumb and index) is the most consistent area
5. Deep Branch = Posterior Interosseous Nerve (PIN)
- Winds around the neck of the radius between the two heads of the supinator muscle (passing through the "Arcade of Frohse" - the fibrous arch of the supinator)
- Enters the posterior compartment of the forearm
- Supplies all muscles of the posterior forearm:
| Muscle | Action |
|---|
| Supinator (C6) | Supination |
| Extensor carpi radialis brevis (ECRB) (C7) | Extension + radial deviation of wrist |
| Extensor digitorum (C7, C8) | Extension of fingers at MCP |
| Extensor digiti minimi (C7, C8) | Extension of little finger |
| Extensor carpi ulnaris (C7, C8) | Extension + ulnar deviation of wrist |
| Abductor pollicis longus (C7, C8) | Abduction + extension of 1st metacarpal |
| Extensor pollicis brevis (C7, C8) | Extension of thumb MCP |
| Extensor pollicis longus (C7, C8) | Extension of thumb IP |
| Extensor indicis (C7, C8) | Independent extension of index finger |
Diagram
Fig. 8: Radial Nerve in the Arm (Gray's Anatomy for Students)
Complete Summary of Distribution
Motor Distribution:
| Region | Muscles (all extensors) |
|---|
| Arm | Triceps (3 heads), anconeus, brachioradialis, ECRL, lateral brachialis |
| Forearm (via PIN) | Supinator, ECRB, ED, EDM, ECU, APL, EPB, EPL, EI |
Sensory Distribution:
| Branch | Area |
|---|
| Posterior cutaneous nerve of arm | Posterior arm skin |
| Inferior lateral cutaneous nerve of arm | Lower lateral arm |
| Posterior cutaneous nerve of forearm | Posterior forearm |
| Superficial radial nerve | Dorsal lateral hand + lateral 3½ digit dorsa |
Q.14 - Describe Root Value, Muscles Supplied and Clinical Anatomy of Radial Nerve [7 Marks]
Root Value
C5, C6, C7, C8, T1 (predominantly C7)
Muscles Supplied (Complete List)
| Segment | Muscle | Root Values |
|---|
| In the Arm | Triceps brachii (all 3 heads) | C6, C7, C8 |
| Anconeus | C7, C8 |
| Brachioradialis | C5, C6 |
| Extensor carpi radialis longus | C5, C6 |
| Lateral brachialis (partial) | C5, C6 |
| In the Forearm (via PIN) | Supinator | C6 |
| ECRB | C7 |
| Extensor digitorum | C7, C8 |
| Extensor digiti minimi | C7, C8 |
| Extensor carpi ulnaris | C7, C8 |
| Abductor pollicis longus | C7, C8 |
| Extensor pollicis brevis | C7, C8 |
| Extensor pollicis longus | C7, C8 |
| Extensor indicis | C7, C8 |
Mnemonic for forearm extensors (PIN supplies): "SB ED ECU APL EP EI" = Supinator, ECRB, Extensor Digitorum, ECU, APL, EPB, EPL, EI
Clinical Anatomy - Sites of Injury
Site 1: In the Axilla (High radial nerve injury)
| Feature | Detail |
|---|
| Cause | Crutch palsy (poorly fitted axillary crutch compresses nerve); Saturday night palsy (arm draped over chair back); humerus fracture at proximal level |
| Motor loss | ALL muscles below including triceps |
| Deformity | Wrist drop + inability to extend fingers + weak elbow extension |
| Sensory loss | Posterior arm + posterior forearm + dorsal lateral hand |
Site 2: In the Radial (Spiral) Groove - Most Common Site
| Feature | Detail |
|---|
| Cause | Fracture of the mid-shaft of humerus (most common); "Saturday night palsy" (drunken sleep with arm over chair); tourniquet injury |
| Motor loss | Wrist extensors + finger extensors; supinator is variably affected |
| Key feature | Triceps is SPARED (its branches arise proximal to the radial groove) |
| Deformity | Wrist drop - wrist falls into flexion; fingers cannot be extended at MCP joints |
| Sensory loss | Dorsum of hand (first dorsal webspace) |
| Reflexes | Brachioradialis reflex lost; triceps reflex intact |
Wrist Drop - The Classic Deformity
When the wrist cannot be extended, the extensor tendons become slack and the patient cannot grip effectively either. The flexor muscles are unopposed and the wrist falls into flexion. Finger extension at the MCP is lost (but IP joints can be extended by lumbricals and interossei, which are median and ulnar nerve).
Site 3: Posterior Interosseous Nerve (PIN) Palsy - At the Elbow
| Feature | Detail |
|---|
| Cause | Compression at the Arcade of Frohse (fibrous arch of supinator); radial head fracture; lipoma; rheumatoid synovitis |
| Motor loss | All muscles of posterior forearm EXCEPT ECRL |
| Key feature | No wrist drop (ECRL is intact - it comes off the main radial nerve before PIN). But the patient has radial deviation on wrist extension |
| Finger drop: Fingers cannot be extended at MCP | |
| Sensory loss | NONE (superficial branch is not affected) |
Site 4: Superficial Radial Nerve Injury (Wartenberg's Syndrome)
| Feature | Detail |
|---|
| Cause | Tight watch strap, handcuffs, de Quervain's surgery |
| Effect | Purely sensory - pain and paresthesia over dorsal lateral hand |
| No motor loss | |
Summary Table of Radial Nerve Injuries
| Level of Injury | Triceps | Wrist Extension | Finger Extension | Sensory Loss |
|---|
| Axilla | Lost | Lost | Lost | Full area |
| Radial groove | Spared | Lost | Lost | Dorsal hand |
| PIN (at elbow) | Spared | Radial deviation (ECRL intact) | Lost | NONE |
| Superficial branch | Spared | Normal | Normal | Dorsal hand only |
Clinical Testing
- Motor: Ask patient to extend wrist and fingers against resistance
- Reflex: Triceps jerk (C7), brachioradialis (C5-C6)
- Sensory: Test first dorsal webspace (most consistent area of radial nerve sensory territory)
- Tinel's sign: Tap over the radial groove for nerve regeneration
Q.15 - Specify the Parts, Course and Branches of the Axillary Artery [7 Marks]
Introduction
The axillary artery is the continuation of the subclavian artery. It begins as the subclavian artery crosses the lateral border of the 1st rib and ends as it crosses the inferior border of teres major, where it continues as the brachial artery. It is the principal blood supply to the shoulder region and upper limb.
Course
The axillary artery passes through the axilla, accompanied by the three cords of the brachial plexus (which wind around it). The cords - and therefore all terminal nerves of the upper limb - are named according to their position relative to the second part of this artery.
Parts (Divided by Pectoralis Minor)
The pectoralis minor muscle crosses the axillary artery anteriorly, dividing it into three parts:
| Part | Position | Number of Branches |
|---|
| First part | From lateral border of rib I to upper border of pectoralis minor | 1 branch |
| Second part | Behind (posterior to) pectoralis minor | 2 branches |
| Third part | From lower border of pectoralis minor to inferior border of teres major | 3 branches |
Mnemonic: "She Tells Lies" → 1, 2, 3 branches
Branches in Detail
First Part: 1 Branch
1. Superior (Supreme) Thoracic Artery
- Passes medially between pectoralis major and minor
- Supplies: Upper two intercostal spaces, pectoralis major and minor muscles
Second Part: 2 Branches
2. Thoracoacromial Artery (thoracicoaxillary artery)
- Short trunk that pierces the clavipectoral fascia just medial to the pectoralis minor
- Immediately divides into 4 branches:
| Branch | Distribution |
|---|
| Pectoral branch | Both pectoral muscles; follows the deltopectoral groove |
| Acromial branch | Acromion; forms acromial rete (arterial network on acromion) |
| Deltoid branch | Deltoid muscle (accompanies cephalic vein in deltopectoral groove) |
| Clavicular branch | Subclavius muscle; sternoclavicular joint |
3. Lateral Thoracic Artery
- Descends along the lateral border of pectoralis minor
- Accompanies the long thoracic nerve
- Supplies: Pectoralis major and minor, serratus anterior, lateral breast (important in breast surgery)
- Larger in females (supplies lateral mammary branches)
Third Part: 3 Branches
4. Subscapular Artery (largest branch of axillary artery)
- Descends along the lateral border of subscapularis
- Divides almost immediately into:
| Terminal Branch | Course | Supplies |
|---|
| Circumflex scapular artery | Passes through the triangular space (winds around lateral border of scapula) | Infraspinous fossa; participates in scapular arterial anastomosis |
| Thoracodorsal artery | Descends with thoracodorsal nerve to latissimus dorsi | Latissimus dorsi; serratus anterior |
5. Anterior Circumflex Humeral Artery
- Passes anteriorly around the surgical neck of the humerus
- Anastomoses with the posterior circumflex humeral artery
- Smaller of the two circumflex humeral arteries
- Supplies: Anterior capsule of shoulder joint; tendon of long head of biceps in bicipital groove
6. Posterior Circumflex Humeral Artery
- Much larger; passes through the quadrangular space with the axillary nerve
- Winds around the posterior surgical neck of the humerus
- Anastomoses with the anterior circumflex humeral artery
- Supplies: Deltoid (major supply), glenohumeral joint capsule, teres minor, head of humerus
Relations of the Axillary Artery
| Part | Medial | Lateral | Anterior | Posterior |
|---|
| 1st | Axillary vein | Roots of brachial plexus | Pectoral fascia/veins | Serratus anterior |
| 2nd | Medial cord | Lateral cord | Pectoralis minor | Posterior cord |
| 3rd | Ulnar, medial cutaneous nerves | Musculocutaneous, coracobrachialis | Median nerve | Radial, axillary nerves |
Applied Anatomy
1. Scapular Anastomosis
The subscapular artery connects to the suprascapular artery (from thyrocervical trunk of subclavian) through the circumflex scapular artery. This anastomosis:
- Provides collateral circulation when axillary artery is ligated
- Allows the hand to remain viable even when the axillary artery is occluded proximal to the subscapular artery origin
2. Axillary Artery Injury
- Penetrating trauma (stab, gunshot wounds) or severe shoulder dislocation
- Vascular surgeon must be involved early
- Collateral anastomosis may not be sufficient in acute occlusion
3. Surgical Importance
- In breast surgery (mastectomy, axillary clearance): The lateral thoracic, subscapular, and thoracodorsal arteries are all encountered
- The thoracodorsal artery is the pedicle for the latissimus dorsi flap - one of the most widely used reconstructive flaps
4. Thoracodorsal Artery Flap
- Reliable pedicle for latissimus dorsi myocutaneous flap
- Used in breast reconstruction, head and neck reconstruction
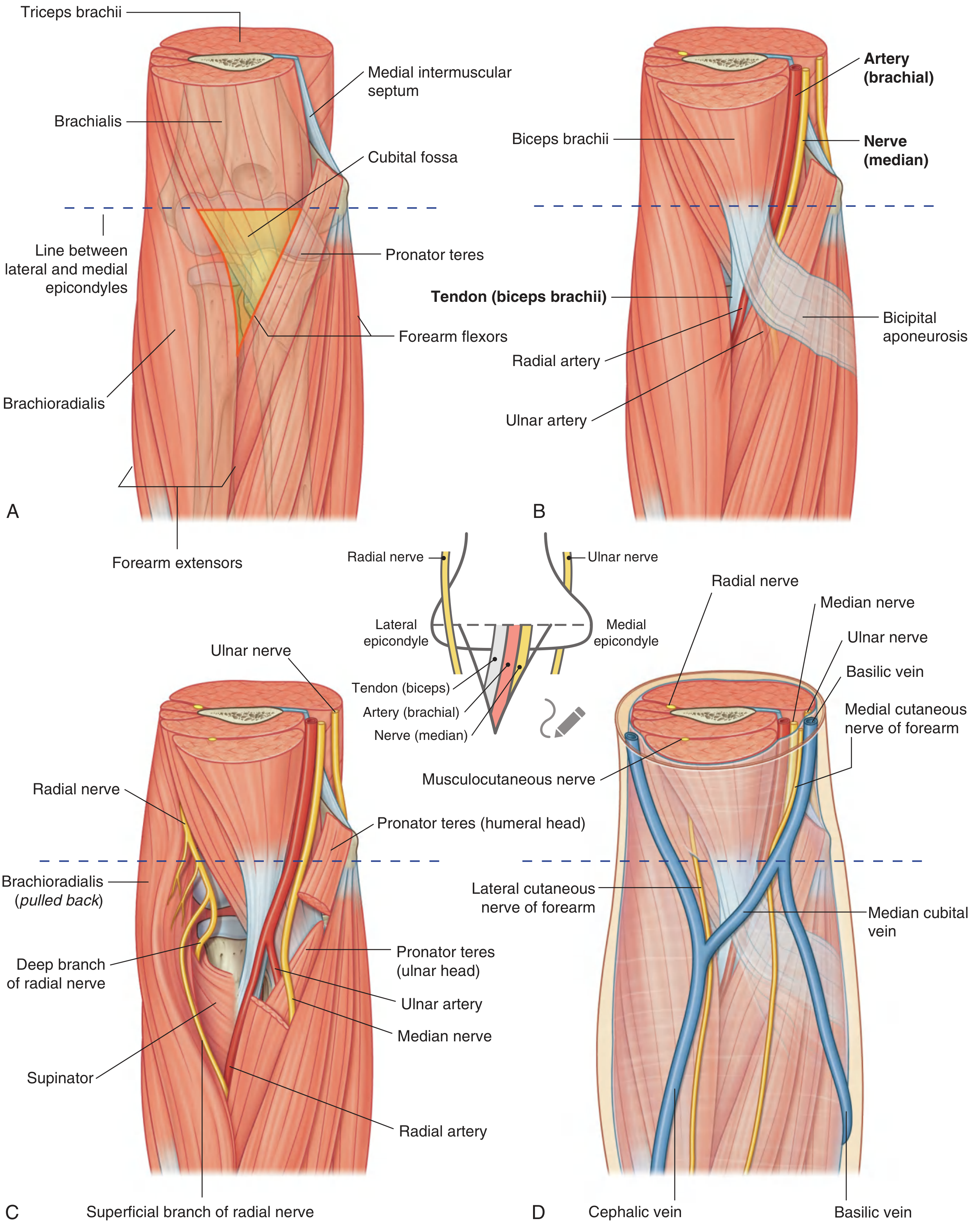
Q.16 - Cubital Fossa [7 Marks]
Introduction
The cubital fossa is a triangular depression on the anterior aspect of the elbow joint, representing the transition zone between the arm and forearm. It contains critical neurovascular structures and is an important site for clinical procedures and injuries.
Boundaries
| Boundary | Structure | Notes |
|---|
| Base (roof/superior border) | Imaginary horizontal line between the medial and lateral epicondyles of the humerus | The landmark for the "base" |
| Medial boundary | Medial margin of the pronator teres muscle | Pronator teres has two heads (humeral + ulnar) |
| Lateral boundary | Medial margin of the brachioradialis muscle | Brachioradialis is the most lateral muscle of forearm |
| Apex | Where pronator teres and brachioradialis meet, pointing inferiorly | This is the apex of the triangle |
| Floor (deep) | Brachialis (medial 2/3) and Supinator (lateral 1/3) | These muscles form the deep bed of the fossa |
| Roof (anterior) | 1. Skin + superficial fascia (containing veins and cutaneous nerves) 2. Bicipital aponeurosis (deep layer) | The bicipital aponeurosis covers and protects deeper structures |
Diagram
Fig. 9: Cubital Fossa. A - Margins. B - Contents. C - Radial nerve. D - Superficial structures (Gray's Anatomy for Students)
Contents (Lateral to Medial - mnemonic: "TAN" = Tendon, Artery, Nerve)
| Structure | Position | Notes |
|---|
| Tendon of biceps brachii | Most lateral content | Passes to radial tuberosity; gives off bicipital aponeurosis (medially) |
| Brachial artery | Medial to biceps tendon | Normally bifurcates into radial and ulnar arteries at the apex of the fossa |
| Median nerve | Most medial content | Exits fossa between the two heads of pronator teres |
Additional:
- The radial nerve and its terminal branches lie just outside the lateral boundary (beneath brachioradialis), not truly within the fossa - the radial nerve divides into:
- Superficial branch: Continues deep to brachioradialis
- Deep branch (PIN): Enters supinator
- The ulnar nerve does NOT pass through the cubital fossa - it passes posterior to the medial epicondyle (in the cubital tunnel)
Roof Contents (Superficial Layer)
The roof contains important structures within the subcutaneous tissue:
| Structure | Significance |
|---|
| Median cubital vein | Most clinically important superficial vein; connects cephalic vein (lateral) and basilic vein (medial); the most common site for venipuncture |
| Lateral cutaneous nerve of forearm (from musculocutaneous nerve) | Lateral to biceps tendon |
| Medial cutaneous nerve of forearm | Medial side; must avoid in venipuncture |
| Cephalic vein | Lateral boundary of fossa |
| Basilic vein | Medial |
Bicipital Aponeurosis
- A flat fibrous expansion from the medial aspect of the biceps tendon
- Passes medially and distally to blend with the deep fascia of the forearm
- Covers and protects the brachial artery and median nerve anteriorly
- Used as a guide during vascular surgery (divide the aponeurosis to access the brachial artery)
- The sharp medial edge of the bicipital aponeurosis can be palpated
Applied Anatomy
1. Blood Pressure Measurement
The brachial artery lies in the cubital fossa under the bicipital aponeurosis:
- The sphygmomanometer cuff is applied to the arm
- The stethoscope is placed over the brachial artery in the cubital fossa
- Korotkoff sounds are heard here
2. Venipuncture and IV Cannulation
The median cubital vein is the most commonly used vein for:
- Blood sampling
- IV cannulation
- Blood transfusion
- Cardiac catheterization (older technique)
Important: The brachial artery and median nerve lie just deep to the bicipital aponeurosis. A venipuncture that goes too deep may inadvertently puncture the brachial artery.
3. Elbow Dislocations and Fractures
Supracondylar fracture of humerus (children) - the most common fracture around the elbow in children:
- The sharp distal fragment may injure the brachial artery → ischemia to the forearm
- The median nerve (anterior interosseous branch) may be injured
- The radial nerve may be injured
- Volkmann's ischemic contracture results from unrecognized arterial injury → forearm compartment syndrome → fibrosis → flexion contracture of wrist and fingers
4. Entrapment Syndromes
- Pronator teres syndrome: Compression of the median nerve between the two heads of pronator teres as it exits the cubital fossa → pain in the forearm + weakness of FPL and FDP
- Anterior interosseous nerve syndrome: AIN compressed after it branches from the median nerve → weakness of FPL + lateral FDP + pronator quadratus
5. Branchial Aneurysm
- Traumatic pseudoaneurysm of the brachial artery can develop in the cubital fossa after arterial puncture
- Presents as a pulsatile swelling with a bruit
6. Surgical Access
- The Henry approach (anterior approach to the forearm) begins at the cubital fossa
- The brachioradialis-FCR interval is exploited after identifying the key structures of the fossa
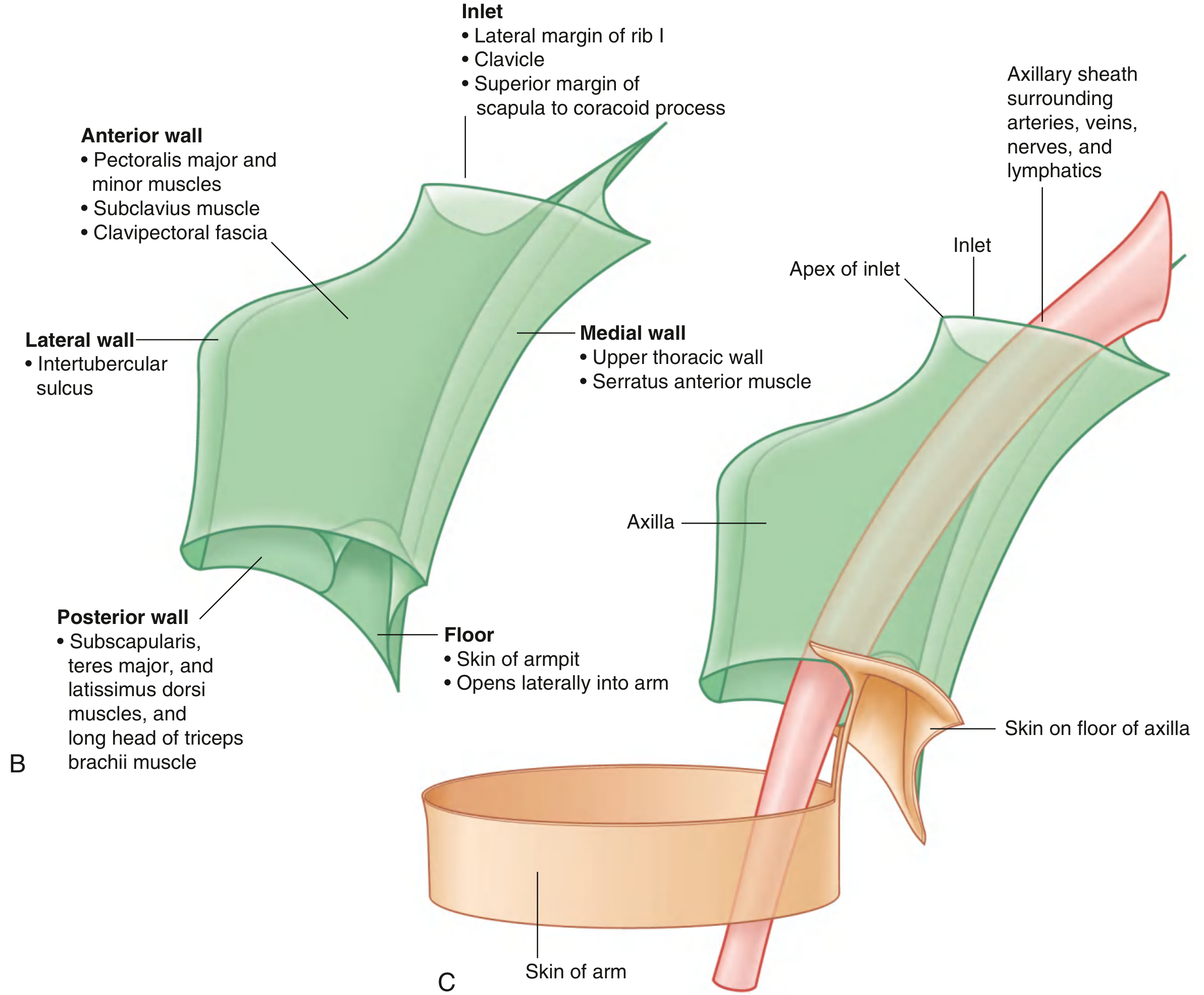
Q.17 - Axilla - Boundaries, Contents and Applied Anatomy [7 Marks]
Introduction
The axilla (armpit) is a pyramidal space situated between the arm and the chest wall. It acts as the gateway to the upper limb - all major neurovascular structures passing to or from the upper limb traverse this space. It is clinically important in breast cancer surgery and shoulder pathology.
Shape
The axilla is pyramidal with:
- 1 apex (inlet - superior)
- 4 walls (anterior, posterior, medial, lateral)
- 1 base (floor - inferior)
Boundaries
Apex (Axillary Inlet)
- Directed upward, medially, and posteriorly
- The margins of the inlet are entirely bony:
- Anterior: Posterior surface of the clavicle
- Posterior: Superior border of the scapula to the coracoid process
- Medially: Lateral border of rib I
- The apex communicates with the root of the neck (posterior triangle)
Anterior Wall
| Layer | Structure |
|---|
| Superficial | Pectoralis major (and its fascia) |
| Deep | Pectoralis minor + subclavius + clavipectoral fascia |
Posterior Wall
| Structure | Notes |
|---|
| Subscapularis (superior part) | Medially; forms bulk of posterior wall |
| Teres major (inferior) | Lower lateral |
| Latissimus dorsi (inferior) | Winds around teres major; forms the posterior axillary fold |
| Long head of triceps (lateral) | Most lateral structure |
Medial Wall
- Serratus anterior muscle (overlying ribs 1-4 and intercostal spaces)
- Upper part of thoracic wall
Lateral Wall (Narrowest Wall)
- Intertubercular sulcus (bicipital groove) of the humerus
- Formed by the convergence of the anterior and posterior walls on the humerus
Floor (Base)
- Formed by the axillary fascia (continuation of clavipectoral fascia and pectoral/latissimus fascia)
- Covered by skin bearing axillary hair
- The skin of the floor forms the "armpit"
Diagram
Fig. 10: Boundaries of the Axilla. B - All walls labeled. C - Continuity with the arm (Gray's Anatomy for Students)
Contents of the Axilla
1. Axillary Artery (and its 6 branches)
- Continuation of the subclavian artery from the lateral border of rib I
- Becomes the brachial artery at the inferior border of teres major
- Divided into 3 parts by pectoralis minor (see Q.15)
2. Axillary Vein
- Formed by the union of the brachial veins + basilic vein at the lower border of teres major
- Lies medial and anterior to the axillary artery
- Becomes the subclavian vein at the lateral border of rib I
- Tributaries: Cephalic vein + veins accompanying the 6 arterial branches
3. Brachial Plexus (Cords and Terminal Branches)
- The three cords surround the second part of the axillary artery:
- Lateral cord (C5, C6, C7): Lateral to artery
- Medial cord (C8, T1): Medial to artery
- Posterior cord (C5-T1): Posterior to artery
- Terminal branches arise in the distal axilla
4. Axillary Lymph Nodes (5 Groups)
This is the most clinically important content for cancer diagnosis and staging:
| Group | Position | Drainage Territory |
|---|
| Anterior (Pectoral) | Along lateral thoracic vessels, at the medial wall | Anterior and lateral chest wall, lateral breast (75% of breast lymph) |
| Posterior (Subscapular) | Along subscapular vessels, at the posterior wall | Posterior chest wall, back, posterior neck, shoulder |
| Lateral | Along the lateral axillary vein | Entire upper limb |
| Central | Centre of the axilla, embedded in fat | Receives from anterior, posterior, and lateral groups |
| Apical (Infraclavicular) | At the apex of the axilla, along medial side of axillary vein | Receives from all other groups; drains to subclavian trunk → thoracic duct (left) or right lymphatic duct |
Clinical Staging of Axillary Nodes in Breast Cancer:
- Level I: Below/lateral to pectoralis minor
- Level II: Behind pectoralis minor (including the central group)
- Level III: Above/medial to pectoralis minor (apical group)
5. Other Contents
| Structure | Notes |
|---|
| Axillary fat | Fills all remaining spaces; encloses lymph nodes |
| Long thoracic nerve | Runs on the external surface of serratus anterior on the medial wall |
| Intercostobrachial nerve | Lateral cutaneous branch of T2; crosses the axilla to supply posteromedial arm skin |
| Proximal parts of biceps brachii and coracobrachialis | Pass through axilla to arm |
| Axillary process of breast | An extension of breast tissue that projects through the clavipectoral fascia into the axilla |
Applied Anatomy
1. Breast Cancer and the Axilla
- Approximately 75% of breast lymphatic drainage goes to the axillary nodes (primarily Level I - pectoral group)
- 25% drains to the internal mammary chain
- Sentinel lymph node biopsy (SLNB): The first lymph node to receive drainage from the tumor is identified and biopsied; if negative, formal axillary dissection can be avoided
- Axillary node dissection: Removal of Level I-III nodes; staging procedure
- Complications of axillary dissection:
- Long thoracic nerve injury → winged scapula
- Thoracodorsal nerve injury → paralysis of latissimus dorsi
- Axillary vein injury → upper limb lymphedema (chronic arm swelling)
2. Winged Scapula
- Injury to the long thoracic nerve (C5, C6, C7) during axillary surgery
- Serratus anterior is paralyzed
- Medial border of scapula wings away from the chest wall on pushing
3. Quadrangular Space Syndrome
- Compression of the axillary nerve and posterior circumflex humeral artery in the quadrangular space (bounded by teres minor, teres major, long head of triceps, surgical neck of humerus)
- Causes: Hypertrophied muscles, fibrous bands, shoulder overuse
- Symptoms: Deltoid weakness, dull aching shoulder pain, loss of sensation over "badge area"
4. Axillary Vein Thrombosis
- "Effort thrombosis" or Paget-Schroetter syndrome
- Caused by repetitive overhead activities (swimmers, baseball pitchers, weight lifters)
- Presents with sudden arm swelling, heaviness, and pain
- Treated with anticoagulation or thrombolysis
5. Crutch Palsy
- Compression of the radial nerve (or whole posterior cord) in the axilla from poorly fitted axillary crutches
- Causes radial nerve injury at the axillary level (highest possible level)
- All muscles including triceps are paralyzed
6. Axillary Dissection and Lymphedema
- Disruption of lymphatic channels during axillary clearance → chronic lymphedema of the upper limb
- The arm becomes chronically swollen and there is a risk of recurrent cellulitis
- Prevented by sentinel node biopsy technique
Reference: All answers compiled from Gray's Anatomy for Students, 4th Edition (Drake, Vogl, Mitchell), S. Das Manual of Clinical Surgery, 13th Edition, General Anatomy and Musculoskeletal System - THIEME Atlas of Anatomy, and Gray's Anatomy, 41st Edition. Source: Medical Textbook Library (Orris).
Study Tips for 7-Mark Questions:
- Introduction (0.5 mark): Define the topic in 1-2 sentences
- Main body with subheadings (5 marks): Use tables, numbered lists, and organized subheadings. Examiners look for completeness.
- Diagram (1 mark): Even a simple labeled diagram earns a mark
- Applied/Clinical anatomy (0.5-1 mark): Always add 2-3 clinical points at the end - this differentiates good answers