2. Anesthetic and Anti pyretic drug
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed to write a comprehensive answer. Let me compile everything into a well-organized response.
Anesthetic and Antipyretic Drugs
PART 1: ANESTHETIC DRUGS
Anesthetics are drugs that cause loss of sensation. They are broadly divided into:
- General anesthetics (IV and inhalational)
- Local anesthetics
A. General Anesthetics
General anesthesia involves a reversible state of unconsciousness, analgesia, amnesia, and muscle relaxation. It is achieved through IV agents, inhalational agents, or a combination.
1. Intravenous (IV) Anesthetics
| Drug | Class | Mechanism | Key Features |
|---|---|---|---|
| Propofol | Alkylphenol | Enhances GABA-A (↑ Cl⁻ currents) | Most commonly used IV anesthetic; rapid onset/offset; antiemetic effect; causes ↓BP via ↓SVR |
| Thiopental | Barbiturate | GABA-A receptor agonist | Rapid onset; accumulates with prolonged use; cerebral protection; contraindicated in porphyria |
| Ketamine | Phencyclidine derivative | NMDA receptor antagonist | Dissociative anesthesia; preserves airway reflexes; sympathomimetic (↑HR, ↑BP); analgesic; risk of psychotomimetic effects; also used as antidepressant |
| Etomidate | Imidazole derivative | GABA-A receptor agonist | Minimal cardiovascular/respiratory effects; preferred in hemodynamically unstable patients; inhibits adrenocortical synthesis (single induction dose can suppress cortisol) |
| Midazolam | Benzodiazepine | GABA-A receptor agonist | Anxiolysis and amnesia; flumazenil reversal agent; prolonged effect in hepatic/renal failure |
| Dexmedetomidine | Alpha-2 agonist | Agonist at α₂-adrenergic receptors (locus coeruleus) | Sedation, sympatholysis, analgesia; minimal respiratory depression; used for ICU sedation and procedural sedation |
- Miller's Anesthesia, 10e, p. 2453-2455
Key point on Propofol: Its context-sensitive half-time is ~10 min for infusions <3 hours, rising to <40 min for infusions up to 8 hours. It produces a dose-dependent decrease in arterial blood pressure mainly via reduced systemic vascular resistance, and has a unique antiemetic property even at sub-sedating concentrations.
Ketamine is uniquely stimulating - it preserves cardiovascular reflexes (unlike other agents), making it useful in trauma/hypovolemic patients. However, it can cause emergence delirium - managed with benzodiazepine premedication.
Etomidate - note that even a single induction dose inhibits adrenocortical steroidogenesis (blocks 11β-hydroxylase), which can be significant in critically ill patients.
2. Inhalational Anesthetics
Used for maintenance (and sometimes induction) of general anesthesia. Key agents:
| Drug | Key Properties |
|---|---|
| Sevoflurane | Rapid onset/offset; preferred for inhalation induction (children); low airway irritation |
| Desflurane | Fastest emergence; airway irritant (not used for induction) |
| Isoflurane | Lowest critical rCBF threshold (best cerebral protection) |
| Nitrous oxide (N₂O) | Analgesic/anesthetic adjunct; associated with increased PONV; 50% N₂O in O₂ was previously favored |
Minimum Alveolar Concentration (MAC) - the concentration of inhaled anesthetic at which 50% of patients do not move in response to a surgical stimulus. Lower MAC = more potent.
Malignant Hyperthermia (MH): A life-threatening complication triggered by volatile anesthetics (e.g., halothane, sevoflurane) and succinylcholine. Propofol, etomidate, barbiturates, opioids, midazolam, and nondepolarizing muscle relaxants are all safe in MH-susceptible patients. Treatment: dantrolene.
- Miller's Anesthesia, 10e, p. 8048-8050; Morgan and Mikhail's Clinical Anesthesiology, 7e, p. 2454
B. Local Anesthetics
Local anesthetics block nerve conduction by dose-dependent blockade of voltage-gated sodium channels, preventing action potential propagation.
Classes
| Class | Examples | Key Feature |
|---|---|---|
| Amino Esters | Cocaine, procaine, chloroprocaine, tetracaine | Metabolized by plasma pseudocholinesterase |
| Amino Amides | Lidocaine, bupivacaine, ropivacaine, levobupivacaine, mepivacaine | Metabolized by liver |
Memory trick: Amides have 2 "i"s in their name (lidocaine → locaine); Esters have only 1 "i".
Physicochemical Properties
- pKa: Lower pKa → faster onset (more drug in uncharged form, which penetrates nerve membrane). All local anesthetics are ineffective in acidic (inflamed) tissue because they stay ionized and cannot penetrate the nerve.
- Protein binding: Higher protein binding → longer duration of action
- Hydrophobicity (lipid solubility): Greater hydrophobicity → greater potency
Toxicity
Early signs of local anesthetic systemic toxicity (LAST): numbness/tingling of tongue or lips, metallic taste, lightheadedness, tinnitus, visual disturbances → progressing to slurred speech, seizures → cardiovascular collapse.
Bupivacaine cardiotoxicity is especially difficult to treat (cardiac sodium channel block). Treatment of LAST: lipid emulsion therapy (Intralipid 20%).
Liposomal bupivacaine - encapsulated in multivesicular liposomes; can provide up to 72 hours of analgesia after local infiltration. However, evidence does not consistently show superior pain control compared with standard local anesthetics.
- Sabiston Textbook of Surgery, p. 1552-1560
PART 2: ANTIPYRETIC DRUGS
Antipyretics reduce fever by inhibiting prostaglandin synthesis (primarily PGE₂) in the hypothalamic thermoregulatory center.
Mechanism of Fever
Infection/inflammation → WBC activation → release of pyrogens (cytokines: IL-1, TNF-α) → stimulate COX-2 → ↑PGE₂ → raises the set-point of the anterior hypothalamus → fever.
Antipyretics block this pathway by inhibiting COX → ↓PGE₂ → thermostat resets to normal → heat dissipation via peripheral vasodilation and sweating.
Important: Antipyretics only lower elevated (febrile) temperature - they have no effect on normal body temperature.
The Cyclooxygenase (COX) Pathway
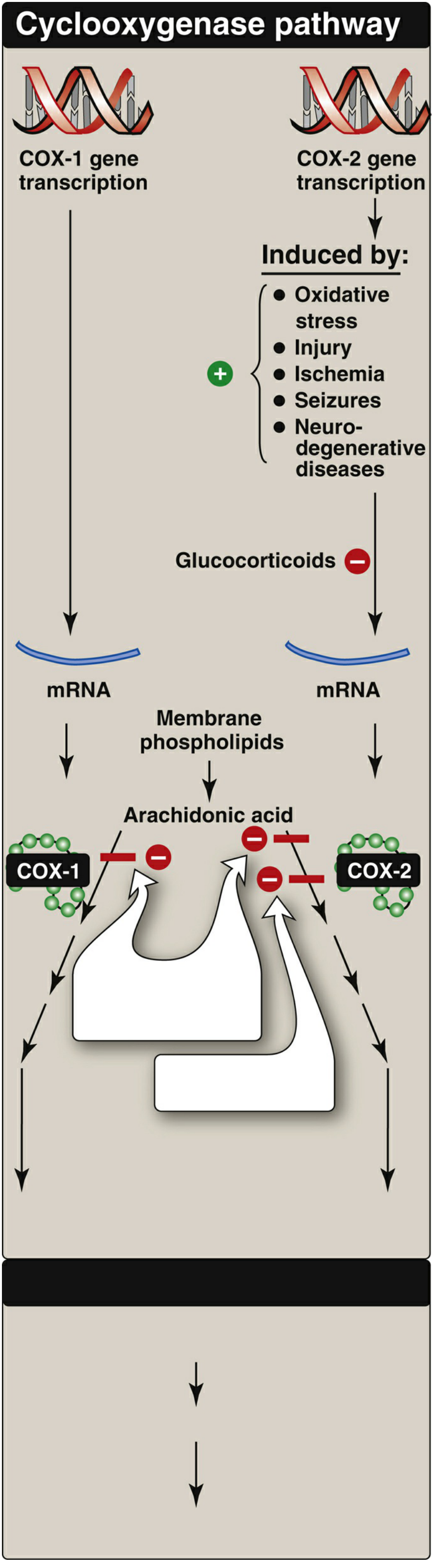
- COX-1: Constitutive enzyme - governs gastric cytoprotection, platelet aggregation, vascular homeostasis, renal function
- COX-2: Induced by inflammatory mediators (TNF-α, IL-1); also constitutively expressed in brain, kidney, bone. Inhibition of COX-2 → anti-inflammatory/analgesic effects
Major Antipyretic Drug Classes
1. NSAIDs (Non-Selective COX Inhibitors)
NSAIDs are chemically dissimilar agents classified by chemical structure:
| Chemical Class | Examples |
|---|---|
| Salicylic acid | Aspirin, diflunisal, salsalate |
| Propionic acid | Ibuprofen, naproxen, ketoprofen |
| Acetic acid | Indomethacin, diclofenac, ketorolac, etodolac |
| Enolic acid | Piroxicam, meloxicam |
| Fenamates | Mefenamic acid, meclofenamate |
Three major therapeutic actions: Anti-inflammatory, analgesic, antipyretic.
Aspirin is unique - it is an irreversible inhibitor of cyclooxygenase (acetylates the enzyme). All other NSAIDs are reversible inhibitors.
Antipyretic doses:
- Aspirin: 2 × 325 mg tablets → analgesia; 12-20 tablets/day → anti-inflammatory (dose-dependent)
- Ibuprofen, naproxen: commonly used for fever
Adverse effects of NSAIDs:
- GI: ulceration, bleeding (COX-1 inhibition reduces gastric mucosal protection)
- Renal: reduced renal blood flow (especially in volume-depleted states)
- Platelet dysfunction: aspirin irreversibly inhibits platelet COX-1 → ↓TXA₂ → ↓aggregation
- Cardiovascular: selective COX-2 inhibitors and some NSAIDs increase thrombotic risk
- Reye syndrome: Aspirin use in children (<19 years) with viral infections (varicella, influenza) → associated with Reye syndrome → use avoided in children
- Pregnancy: NSAIDs contraindicated in 3rd trimester (premature closure of ductus arteriosus)
2. Selective COX-2 Inhibitor: Celecoxib
- Mechanism: Selectively and reversibly inhibits COX-2 (unlike aspirin's irreversible inhibition)
- Uses: RA, osteoarthritis, acute pain
- Advantage: Less GI bleeding and dyspepsia than non-selective NSAIDs
- Disadvantage: ↑cardiovascular thrombotic risk; benefit over GI safety lost when combined with aspirin
- Metabolism: CYP2C9 in liver; half-life ~11 hours
- Avoid in severe hepatic or renal disease
3. Acetaminophen (Paracetamol)
- Mechanism: Inhibits prostaglandin synthesis in the CNS → antipyretic + analgesic effects. Has minimal effect on peripheral COX (inactivated peripherally) → weak anti-inflammatory action. Does not affect platelet function. Not an NSAID.
- Uses: Fever and mild-to-moderate pain; preferred in:
- Children with viral infections (safe alternative to aspirin - no Reye risk)
- Pregnant women needing analgesia/antipyresis
- Patients with GI intolerance to NSAIDs
Metabolism and Toxicity:
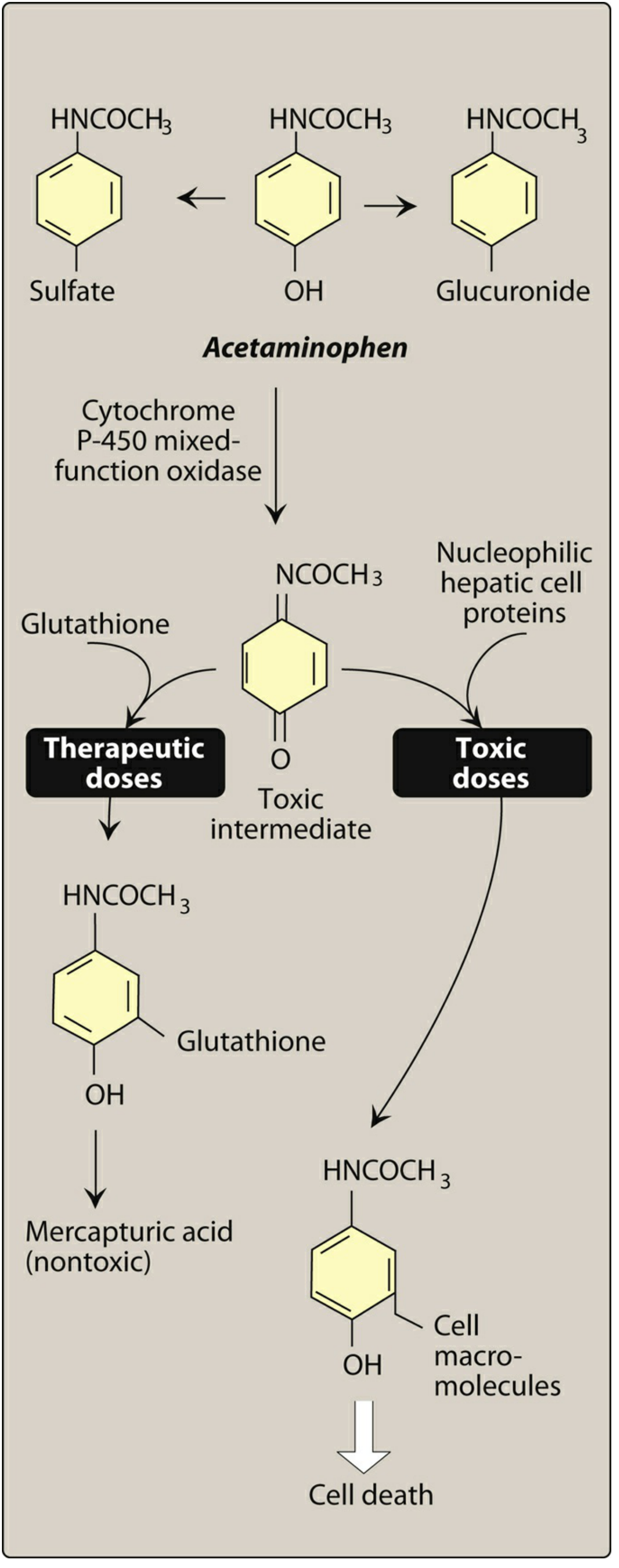
At normal doses: Acetaminophen → conjugated to glucuronide/sulfate (inactive) → excreted in urine. A small portion is oxidized via CYP450 to NAPQI (toxic intermediate), which is rapidly neutralized by glutathione → mercapturic acid (nontoxic).
At toxic doses (overdose): Glutathione depleted → NAPQI accumulates → binds sulfhydryl groups of hepatic proteins → hepatic necrosis (potentially fatal).
High-risk groups for hepatotoxicity: Hepatic disease, chronic alcoholism, malnutrition, viral hepatitis.
Antidote: N-acetylcysteine (NAC) - replenishes glutathione stores.
- Lippincott Illustrated Reviews: Pharmacology, p. 1331-1366
Summary Comparison Table
| Feature | NSAIDs | Celecoxib | Acetaminophen |
|---|---|---|---|
| COX selectivity | Non-selective (COX-1 + COX-2) | COX-2 selective | Minimal peripheral COX inhibition |
| Anti-inflammatory | Yes | Yes | Minimal |
| Analgesic | Yes | Yes | Yes |
| Antipyretic | Yes | Yes | Yes |
| Platelet effect | ↓Aggregation (aspirin irreversibly) | Minimal | None |
| GI risk | High | Low | None at therapeutic doses |
| Hepatotoxicity | Low | Low | High (overdose) |
| Safe in children with viral illness | No (Reye risk for aspirin) | No | Yes |
| Safe in pregnancy | Avoid 3rd trimester | Avoid | Preferred |
| Antidote in overdose | - | - | N-acetylcysteine |
Sources:
- Lippincott Illustrated Reviews: Pharmacology (NSAIDs and Acetaminophen chapter)
- Miller's Anesthesia, 10e (IV anesthetics and general anesthesia)
- Sabiston Textbook of Surgery (local anesthetic drugs)
- Morgan and Mikhail's Clinical Anesthesiology, 7e (MH, IV agents)
This is a shared conversation. Sign in to Orris to start your own chat.