Anemia for university exam
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
I now have everything needed for a complete, exam-ready guide. Here it is:
Anemia - Complete University Exam Guide
Sources: Harrison's Principles of Internal Medicine 22e (2025), Robbins & Kumar Pathologic Basis of Disease, Goldman-Cecil Medicine, Frameworks for Internal Medicine, Lippincott Pharmacology, Quick Compendium of Clinical Pathology
1. Definition
Anemia = blood counts (hemoglobin/hematocrit/RBC count) below normal for a given population.
Normal hemoglobin thresholds (WHO):
- Men: < 13 g/dL
- Women: < 12 g/dL
- Pregnant women: < 11 g/dL
2. Classification
There are two major frameworks to classify anemia. Know both.
A. By Red Cell Size (MCV-based) - Wintrobe Classification
| MCV Category | MCV | Key Causes |
|---|---|---|
| Microcytic | < 80 fL | Iron deficiency, Thalassemia, Anemia of inflammation, Sideroblastic |
| Normocytic | 80-100 fL | Aplastic anemia, Renal disease, Endocrinopathies, Marrow invasion, Myeloma, Pure red cell aplasia |
| Macrocytic | > 100 fL | B12 deficiency, Folate deficiency, Hypothyroidism, Liver disease, Alcohol, Medications (chemotherapy), Myelodysplasia |
Macrocytic anemias are further divided: oval macrocytes (megaloblastic - B12/folate/drugs) vs. round macrocytes (alcohol, liver disease, hypothyroidism, reticulocytosis).
B. By Mechanism (Reticulocyte-Based)
The absolute reticulocyte count is the key first step:
| Reticulocyte Count | Mechanism | Examples |
|---|---|---|
| High (> 100,000/µL) | Hyperproductive - increased loss/destruction | Bleeding, Hemolysis |
| Low/Normal | Hypoproliferative - impaired production | Nutritional deficiency, Aplastic anemia, Renal disease, Marrow replacement |
At least 75% of all anemias are hypoproliferative. The most common cause is mild-moderate iron deficiency or inflammation. - Harrison's 22e
3. Diagnostic Approach - Flowchart
Step 1: Check MCV (microcytic / normocytic / macrocytic)
Step 2: Check reticulocyte count (high = destruction/loss; low = underproduction)
Step 3: Peripheral blood smear morphology
Step 4: Targeted tests (ferritin, B12, Coombs, bone marrow biopsy, etc.)
4. Major Anemia Types
4.1 Iron Deficiency Anemia (IDA)
Most common nutritional deficiency worldwide.
Causes:
- Blood loss (most common in adults - GI bleeding, menstruation)
- Poor intake / malabsorption (celiac disease)
- Increased demand (pregnancy, growth)
Pathophysiology:
- Iron required for heme synthesis (4 atoms per hemoglobin molecule, ~1 billion per RBC)
- Depletion stages: depleted stores → transport iron falls → hemoglobin synthesis impaired
Lab findings:
| Test | IDA |
|---|---|
| Serum ferritin | LOW (< 30 µg/L = stores depleted) |
| Serum iron | Low |
| TIBC | HIGH |
| Transferrin saturation | Low (< 15%) |
| MCV | Low (microcytic) |
| Blood smear | Microcytic, hypochromic, pencil cells |
Ferritin is an acute-phase reactant - it can be falsely normal/elevated in inflammation even with iron deficiency.
Treatment: Oral iron (ferrous sulfate 325 mg TID); parenteral iron if malabsorption/intolerance.
4.2 Megaloblastic Anemia (B12 and Folate Deficiency)
Key concept: Both B12 and folate are required for DNA synthesis in RBC precursors. Deficiency impairs cell division, causing enlarged, abnormal precursors (megaloblasts).
Vitamin B12 Deficiency:
- Causes: Pernicious anemia (lack of intrinsic factor - autoimmune), strict veganism, malabsorption, gastrectomy, Crohn's disease, metformin use
- Blood smear: Macrocytic RBCs, hypersegmented neutrophils (>5 lobes)
- Bone marrow: Hypercellular with large abnormal red cell precursors
- Neurological features: Subacute combined degeneration of spinal cord (posterior + lateral columns) - does NOT occur with folate deficiency
Folate Deficiency:
- Causes: Poor diet, alcohol use, pregnancy, malabsorption, drugs (methotrexate, phenytoin, trimethoprim)
- Identical hematologic picture to B12 deficiency
- No neurological complications
EXAM TRAP: Giving folate to a B12-deficient patient will correct the anemia but will NOT prevent neurological damage - and may actually mask B12 deficiency. Always check B12 before treating.
Lab findings:
| Test | B12 Deficiency | Folate Deficiency |
|---|---|---|
| Serum B12 | Low | Normal |
| Serum folate | Normal | Low |
| RBC folate | Low | Low |
| MMA (methylmalonic acid) | Elevated | Normal |
| Homocysteine | Elevated | Elevated |
| Neuro symptoms | YES | NO |
4.3 Anemia of Chronic Disease / Inflammation (ACD)
Second most common cause of anemia (after IDA).
Mechanism:
- Chronic inflammation (infection, cancer, autoimmune disease, CKD) elevates cytokines (IL-6, TNF-α)
- IL-6 stimulates liver to produce hepcidin
- Hepcidin blocks ferroportin → traps iron inside macrophages → functional iron deficiency
- Reduced EPO production and EPO responsiveness
- Result: RBCs can't be made despite adequate iron stores
Lab findings:
| Test | ACD | IDA |
|---|---|---|
| Serum ferritin | Normal or HIGH | LOW |
| Serum iron | Low | Low |
| TIBC | Low or normal | HIGH |
| MCV | Normal (normocytic) or mildly low | Low |
Treatment: Treat underlying cause; recombinant EPO in CKD anemia; IV iron in some cases.
4.4 Hemolytic Anemias
Definition: Premature destruction of RBCs (normal lifespan ~120 days is shortened).
Key lab markers of hemolysis:
- High reticulocyte count
- Elevated LDH
- Elevated indirect (unconjugated) bilirubin
- Low haptoglobin
- Hemoglobinuria (in intravascular hemolysis)
Classification:
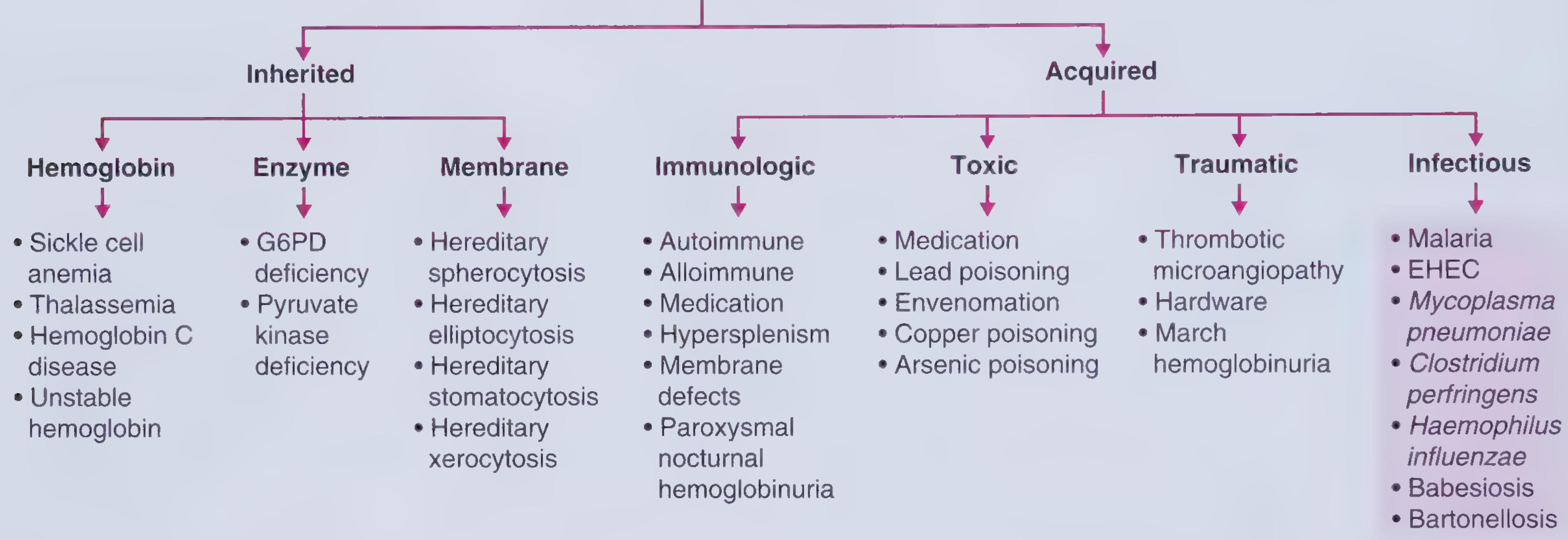
Intravascular vs Extravascular Hemolysis:
| Feature | Intravascular | Extravascular |
|---|---|---|
| Site | Blood vessels | Spleen/liver macrophages |
| Hemoglobinuria | YES | No |
| Haptoglobin | Very low | Low |
| Examples | TTP, G6PD crisis, PNH, mismatched transfusion | Autoimmune HA, hereditary spherocytosis |
Key Hemolytic Subtypes:
Sickle Cell Disease (HbSS):
- Point mutation: glutamate → valine at position 6 of β-globin chain
- HbS polymerizes when deoxygenated → RBCs sickle
- Results in vaso-occlusion, hemolysis, chronic end-organ damage
- Complications: painful crises, stroke, acute chest syndrome, splenic sequestration, avascular necrosis
- Peripheral smear: sickle cells, target cells, Howell-Jolly bodies (functional asplenia)
G6PD Deficiency:
- X-linked recessive enzyme defect
- RBCs vulnerable to oxidative stress
- Triggers: infections, fava beans, medications (primaquine, dapsone, nitrofurantoin)
- Peripheral smear: Heinz bodies (denatured Hb), bite cells
Autoimmune Hemolytic Anemia (AIHA):
- Warm AIHA (IgG): most common; caused by autoantibodies at 37°C - spleen destroys coated RBCs
- Cold AIHA (IgM): triggered by cold; complement activation
- Diagnosis: Direct Antiglobulin Test (Coombs) = POSITIVE
- Treatment: steroids (warm AIHA), avoid cold exposure (cold AIHA), rituximab
Hereditary Spherocytosis:
- Autosomal dominant defect in spectrin/ankyrin/band 3 proteins → loss of RBC membrane → spherocytes
- Symptoms: hemolytic anemia + splenomegaly + jaundice + pigment gallstones
- Osmotic fragility test positive; treated by splenectomy in severe cases
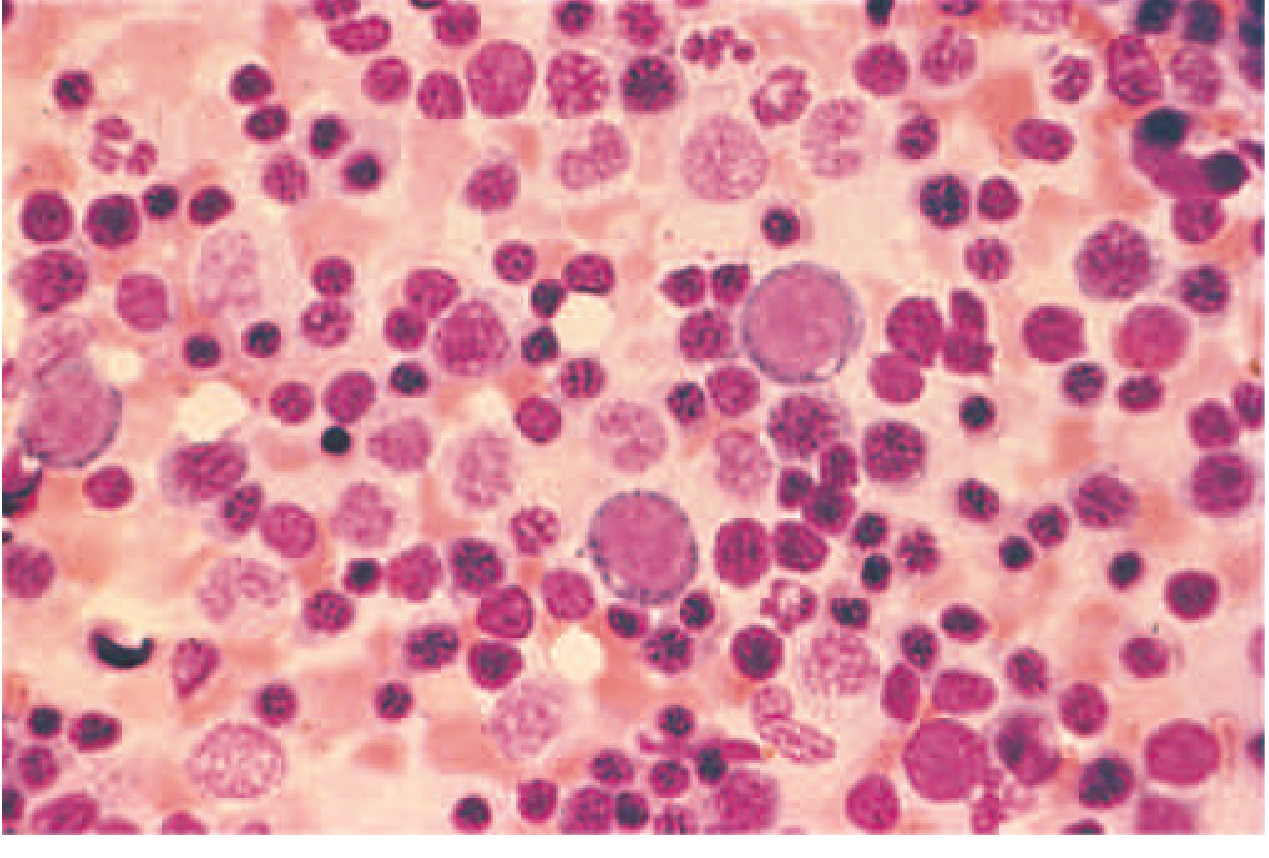
4.5 Aplastic Anemia
Definition: Bone marrow failure leading to pancytopenia (anemia + thrombocytopenia + neutropenia).
Causes:
- Idiopathic (most common - immune-mediated T-cell destruction of stem cells)
- Drugs: chloramphenicol, NSAIDs, chemotherapy
- Viral infections: hepatitis (seronegative), EBV, CMV, parvovirus B19
- Radiation
- Inherited: Fanconi anemia, dyskeratosis congenita
Lab/Diagnosis:
- Pancytopenia with relative lymphocytosis on peripheral smear
- Bone marrow biopsy: hypocellular marrow replaced by fat (gold standard)
- Diagnosis of exclusion
Severity (Camitta criteria):
- Severe: ≥2 of: neutrophils < 0.5×10⁹/L, platelets < 20×10⁹/L, reticulocytes < 20×10⁹/L
Treatment:
- Young patients: allogeneic bone marrow transplant (BMT) - potentially curative
- Older patients / no donor: anti-thymocyte globulin (ATG) + cyclosporine + eltrombopag
4.6 Anemia of Renal Disease (CKD)
- Primary mechanism: decreased EPO production by peritubular cells
- Contributing factors: functional iron deficiency, chronic bleeding, shortened RBC survival, marrow suppression
- Usually normocytic, normochromic
- Treatment: recombinant EPO (epoetin alfa / darbepoetin) + iron supplementation
5. Bone Marrow Examination
Indications for bone marrow biopsy in anemia:
- Circulating immature cells (blasts)
- Severe pancytopenia
- Very low reticulocyte counts (< 0.1%)
- Circulating nucleated RBCs
- Evidence of marrow infiltration (teardrop cells)
- Unexplained severe anemia
Myelophthisic pattern (marrow replacement by tumor/infection): peripheral smear shows nucleated RBCs, teardrop cells, immature WBCs.
6. Key Lab Values - Quick Reference
| Parameter | Normal (Adult) | Notes |
|---|---|---|
| Hb - Men | 13.5-17.5 g/dL | |
| Hb - Women | 12-16 g/dL | |
| MCV | 80-100 fL | Wintrobe classification basis |
| Reticulocytes | 0.5-2.5% | Elevated = loss/destruction |
| Serum ferritin | 30-300 µg/L | Best marker of iron stores |
| Serum iron | 50-150 µg/dL | |
| TIBC | 300-360 µg/dL | Inversely correlates with iron stores |
| Transferrin sat | 25-50% | < 15% = iron deficiency |
| B12 | 200-900 pg/mL | |
| Folate | > 4 ng/mL |
7. Exam High-Yield Summary Table
| Type | MCV | Retics | Key Finding | Classic Cause |
|---|---|---|---|---|
| Iron deficiency | Low | Low | Low ferritin, high TIBC | Chronic blood loss |
| Thalassemia | Very low | Normal/High | Normal ferritin, target cells | Mediterranean/Asian descent |
| B12 deficiency | High | Low | Hyperseg neutrophils, neuro sx | Pernicious anemia, vegans |
| Folate deficiency | High | Low | Hyperseg neutrophils, no neuro sx | Alcoholism, pregnancy |
| Anemia of inflammation | Normal | Low | High ferritin, low TIBC | CKD, cancer, infection |
| Aplastic anemia | Normal | Very low | Pancytopenia, hypocellular BM | Idiopathic (immune) |
| Hemolytic anemia | Normal | HIGH | Low haptoglobin, high LDH | Varies |
| Sickle cell | Normal | High | Sickle cells on smear | HbSS mutation |
8. Treatment Principles
| Anemia | First-Line Treatment |
|---|---|
| Iron deficiency | Oral ferrous sulfate; IV iron if malabsorption |
| B12 deficiency | IM cyanocobalamin; high-dose oral B12 |
| Folate deficiency | Oral folic acid 1-5 mg/day |
| Anemia of inflammation | Treat underlying cause; EPO in CKD |
| Aplastic anemia | BMT (young) or ATG + cyclosporine (older) |
| Warm AIHA | Prednisolone; splenectomy; rituximab |
| Sickle cell | Hydroxyurea (increases HbF); pain management; BMT |
| Thalassemia major | Regular transfusions + iron chelation; BMT |
9. Common Exam Traps
- Ferritin in inflammation: Can be high even in IDA - look at transferrin saturation + clinical context
- Folate masking B12 deficiency: Folate corrects blood count but neurological damage continues - always check B12 first
- Thalassemia trait vs IDA: Both are microcytic; thalassemia has normal ferritin, very low MCV (often < 70), high RBC count (Mentzer index: MCV/RBC < 13 = thalassemia, > 13 = IDA)
- Aplastic anemia = normocytic: Not microcytic despite severe anemia - rule out by bone marrow biopsy
- Reticulocyte count must be corrected: Correct for degree of anemia using: Corrected reticulocyte % = reticulocyte % × (patient Hct / 45)
- PNH: Paroxysmal Nocturnal Hemoglobinuria - complement-mediated intravascular hemolysis; Coombs NEGATIVE; diagnosed by flow cytometry (GPI-anchor deficiency)
References: Harrison's Principles of Internal Medicine 22e (2025), Robbins & Kumar Pathologic Basis of Disease, Goldman-Cecil Medicine, Frameworks for Internal Medicine, Lippincott Illustrated Reviews: Pharmacology, Quick Compendium of Clinical Pathology 5e
This is a shared conversation. Sign in to Orris to start your own chat.