PSVT TREATMENT
Reading File
Finding Sources
Searching PubMed
"supraventricular tachycardia" AND treatment
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Finding Sources
Reading File
Finding Sources
I now have comprehensive information to deliver a detailed, well-organized answer.
PSVT (Paroxysmal Supraventricular Tachycardia) - Treatment
PSVT encompasses AV nodal reentrant tachycardia (AVNRT, ~60% of cases), AV reentrant tachycardia (AVRT), and atrial tachycardia (AT). Most forms depend on AV nodal conduction, which is the key therapeutic target.
Treatment Algorithm (Hemodynamically Stable)
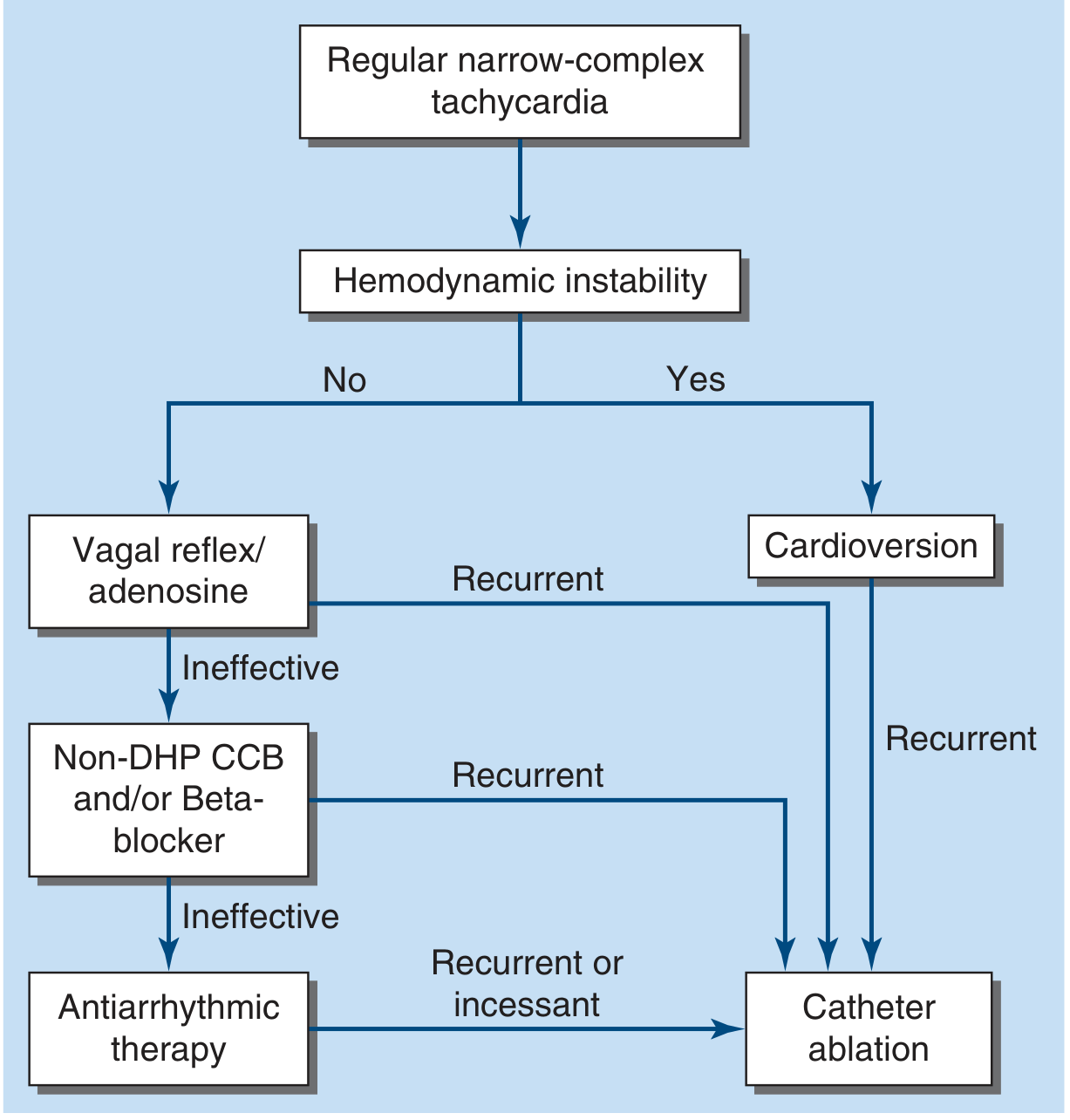
Step 1 - Assess Hemodynamic Status
| Stable | Unstable |
|---|---|
| Proceed stepwise (see below) | Immediate synchronized DC cardioversion |
Hypotension with unconsciousness or respiratory distress = cardiovert without delay. This is rarely needed because IV adenosine works promptly in most cases.
Step 2 - Vagal Maneuvers (Stable patients, first-line)
- Valsalva maneuver - most commonly used; teach patient to self-administer for future episodes
- Carotid sinus massage - reasonable if no carotid bruits and no prior stroke history
- Modified Valsalva (recumbent + leg elevation) - higher conversion rates per recent meta-analysis (PMID: 38235710)
- If effective, record the ECG response - AV block with transient slowing may expose ongoing P waves, revealing AT or atrial flutter as the underlying mechanism
Step 3 - Adenosine (First-line pharmacologic)
- Dose: 6 mg rapid IV bolus through a large-bore IV, followed immediately by NS flush
- If no effect: repeat with 12 mg IV bolus
- Mechanism: transiently blocks AV nodal conduction, terminating the vast majority of PSVT episodes
- Half-life: < 10 seconds (ultra-short acting)
Adverse effects and cautions:
- Transient chest pain, dyspnea, anxiety
- Precipitates AF in up to 15% of patients - use cautiously in WPW (preexcited AF can be hemodynamically catastrophic)
- Contraindicated after cardiac transplantation (hypersensitivity from surgical sympathetic denervation)
- Can theoretically aggravate bronchospasm (use with caution in severe asthma)
A 2025 meta-analysis confirmed adenosine's high efficacy and safety for SVT (PMID: 40055614).
Step 4 - Non-DHP CCB or Beta-Blocker (If adenosine fails)
| Drug | Notes |
|---|---|
| Verapamil IV | Effective; risk of hypotension; longer duration of action than adenosine |
| Diltiazem IV | Effective; also used for rate control in AF/flutter; can be used for stable narrow-complex SVT |
| Beta-blockers IV (metoprolol, esmolol) | Good option; may cause hypotension |
These agents can also be given orally and taken on an as-needed ("pill-in-pocket") basis - patient takes the oral drug when an episode starts, using Valsalva to facilitate termination.
Step 5 - Wide-Complex Tachycardia Special Considerations
- Treat as ventricular tachycardia until proven otherwise
- If regular and patient is stable: a trial of IV adenosine is reasonable
- Very irregular wide-complex tachycardia = likely preexcited AF/flutter - treat with cardioversion, IV procainamide, or ibutilide (NOT adenosine or AV-nodal blockers if WPW)
- If PSVT with aberrancy is unequivocal (prior documented episodes): treat with vagal maneuvers + adenosine
Long-Term / Preventive Management
Pharmacologic Options (for recurrent AVNRT)
| Drug Class | Examples | Classification |
|---|---|---|
| Non-DHP CCB | Verapamil, Diltiazem | Class IIa |
| Beta-blockers | Metoprolol, Atenolol | Class IIa |
| Class Ic | Flecainide, Propafenone | Class IIa |
| Class III | Sotalol, Amiodarone | Class IIa |
- Class Ic agents (flecainide, propafenone) are well-studied and effective but rarely used now given the curative nature of catheter ablation
- Amiodarone/sotalol reserved for patients who are not ablation candidates
Catheter Ablation (Preferred for recurrent PSVT)
- Indications (Class I): Poorly tolerated AVNRT with hemodynamic compromise; recurrent symptomatic AVNRT where patient prefers ablation over drugs
- Success rate: >95% with the posterior (slow-pathway) approach
- Recurrence after ablation: ~3%
- Main complication: AV block (~0.5-1%)
- Cryoablation vs. radiofrequency (RF): Cryo has lower AV block risk but longer procedure times and lower long-term efficacy; RF remains dominant in adults. Cryo preferred by many pediatric electrophysiologists.
- Catheter ablation is considered first-line for recurrent PSVT in most patients given >95% efficacy and low complication rate
Decision Framework for Long-Term Treatment
| Presentation | Recommended Approach |
|---|---|
| Single episode, well-tolerated, self-terminated | Observation; teach Valsalva |
| Minimally symptomatic, self-terminating | Follow clinically, no specific therapy required |
| Symptomatic, recurrent, requires ER visits | Catheter ablation (Class I) or pharmacologic therapy |
| Hemodynamic intolerance | Catheter ablation (Class I) |
| Patient prefers no ablation | Beta-blocker, verapamil, or diltiazem |
| Incessant PSVT | Catheter ablation |
Key Pearls
- Monitor ECG continuously throughout acute management - the response to vagal maneuvers or adenosine can establish the mechanism
- Don't use verapamil/diltiazem in WPW with wide-complex tachycardia - AV-nodal blockade can accelerate conduction via the accessory pathway
- PSVT is not life-threatening in structurally normal hearts; treatment decisions are quality-of-life driven
- Patients can be taught self-management (Valsalva or oral "pill-in-pocket" CCB/beta-blocker)
- Most patients with recurrent episodes are candidates for catheter ablation as definitive cure
Sources: Harrison's Principles of Internal Medicine 22E (2025), Fuster & Hurst's The Heart 15th Ed., Braunwald's Heart Disease, Rosen's Emergency Medicine, Tintinalli's Emergency Medicine; PMID 38235710, 40055614
Verapamil dosage for prophylaxis PSVT
Finding Sources
Searching the Web
verapamil oral dose PSVT prophylaxis mg/day guidelines
Finding Sources
Reading Web Page
https://www.ncbi.nlm.nih.gov/books/NBK538495
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have all the information needed for a complete, well-sourced answer.
Verapamil Dosage for PSVT Prophylaxis
Oral Dosing (Prophylaxis / Long-Term Prevention)
Immediate-Release (IR) Tablets (40, 80, 120 mg)
| Indication | Dose | Frequency | Total Daily Dose |
|---|---|---|---|
| PSVT prophylaxis (non-digitalized) | 80-120 mg | TID or QID | 240-480 mg/day |
| Starting dose (elderly or sensitive) | 40-80 mg | TID | 120-240 mg/day |
Sustained/Extended-Release (SR/ER) Formulations (Calan SR, Verelan, Verelan PM)
| Formulation | Available Strengths | Dosing |
|---|---|---|
| Calan SR / generic ER tabs | 120, 180, 240 mg | 120-480 mg once or twice daily |
| Verelan (caps, once-daily) | 120, 180, 240, 360 mg | Once daily |
| Verelan PM (bedtime dosing) | 100, 200, 240, 300, 360 mg | Once daily at bedtime |
- Typical starting SR dose: 120-180 mg once daily, titrate up as needed
- Maximum daily dose: 480 mg/day (400 mg/day for Verelan PM)
- SR/ER formulations are preferred for long-term prophylaxis due to better tolerability and once- or twice-daily dosing convenience
Note: Due to significant first-pass hepatic metabolism, oral verapamil prolongs the PR interval less than IV verapamil at equivalent concentrations. Dose-to-effect response must be assessed individually.
IV Dosing (Acute Termination - for reference)
| Population | Dose | Notes |
|---|---|---|
| Adults (SVT) | 5-10 mg (0.075-0.15 mg/kg) IV over 2-3 min | May repeat 10 mg after 15-30 min |
| Children 1-16 yr (PSVT) | 0.1-0.3 mg/kg/dose IV | Max 5 mg first dose, 10 mg second dose |
| Max total IV dose | 15-20 mg |
Contraindications
- WPW syndrome / accessory bypass tract with AF or atrial flutter - can accelerate antegrade conduction via accessory pathway, potentially causing VF
- Sick sinus syndrome or 2nd/3rd degree AV block (without pacemaker)
- Severe LV dysfunction / cardiogenic shock (SBP < 90 mmHg)
- Congestive heart failure - use with caution due to negative inotropic effects
- Known hypersensitivity
- Infants and neonates - IV verapamil is avoided due to risk of apnea, bradycardia, and hypotension
Key Clinical Points
- Oral verapamil for prophylaxis is classified as Class IIa (reasonable) for recurrent symptomatic AVNRT - Fuster & Hurst's The Heart, 15th Ed.
- It is generally considered second-line to catheter ablation for recurrent, symptomatic PSVT given ablation's >95% cure rate
- "Pill-in-pocket" strategy: Patients can also take a single oral dose (e.g., 80-120 mg IR) at the onset of a PSVT episode, combined with a Valsalva maneuver, to terminate and prevent early recurrence
- Drug interactions: Verapamil inhibits CYP3A4 and P-glycoprotein - raises digoxin levels (monitor), interacts with beta-blockers (additive AV block and negative inotropy), statins, cyclosporine, and many others
- Common side effects: Constipation (most frequent with oral use), hypotension, dizziness, headache, peripheral edema, bradycardia
- Pretreat with calcium gluconate 1 g IV before IV verapamil in hypotensive patients to reduce hypotension without compromising antiarrhythmic effect
Sources: Roberts & Hedges' Clinical Procedures in Emergency Medicine; The Harriet Lane Handbook 23rd Ed.; Goodman & Gilman's Pharmacological Basis of Therapeutics; drugs.com / FDA prescribing information; StatPearls (NIH)
This is a shared conversation. Sign in to Orris to start your own chat.