Can whiplash injuries causes brain injury?
Reading File
Searching PubMed
whiplash brain injury traumatic
Finding Sources
Finding Sources
Searching PubMed
whiplash associated disorder mild traumatic brain injury
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive textbook evidence to give a detailed, well-cited answer.
Can Whiplash Injuries Cause Brain Injury?
Yes - whiplash can cause brain injury, though it is one of the less widely appreciated aspects of this common trauma. Here is a thorough breakdown:
The Mechanism: How Whiplash Transmits Force to the Brain
The hallmark of whiplash is violent flexion-extension (acceleration-deceleration) of the neck, most commonly from rear-end motor vehicle collisions. Even without a direct blow to the skull, this motion transmits injurious forces to the brain through several mechanisms.
As Adams and Victor's Principles of Neurology (12th ed.) states directly:
"Unless the head is struck, the brain suffers no injury except in the few instances of violent flexion-extension (whiplash) of the neck and possibly in explosion-blast injury with a sudden extreme increase of atmospheric pressure."
The diagram below from Pye's Surgical Handicraft illustrates how acceleration forces generate shearing strains inside the brain - the same forces active in whiplash:
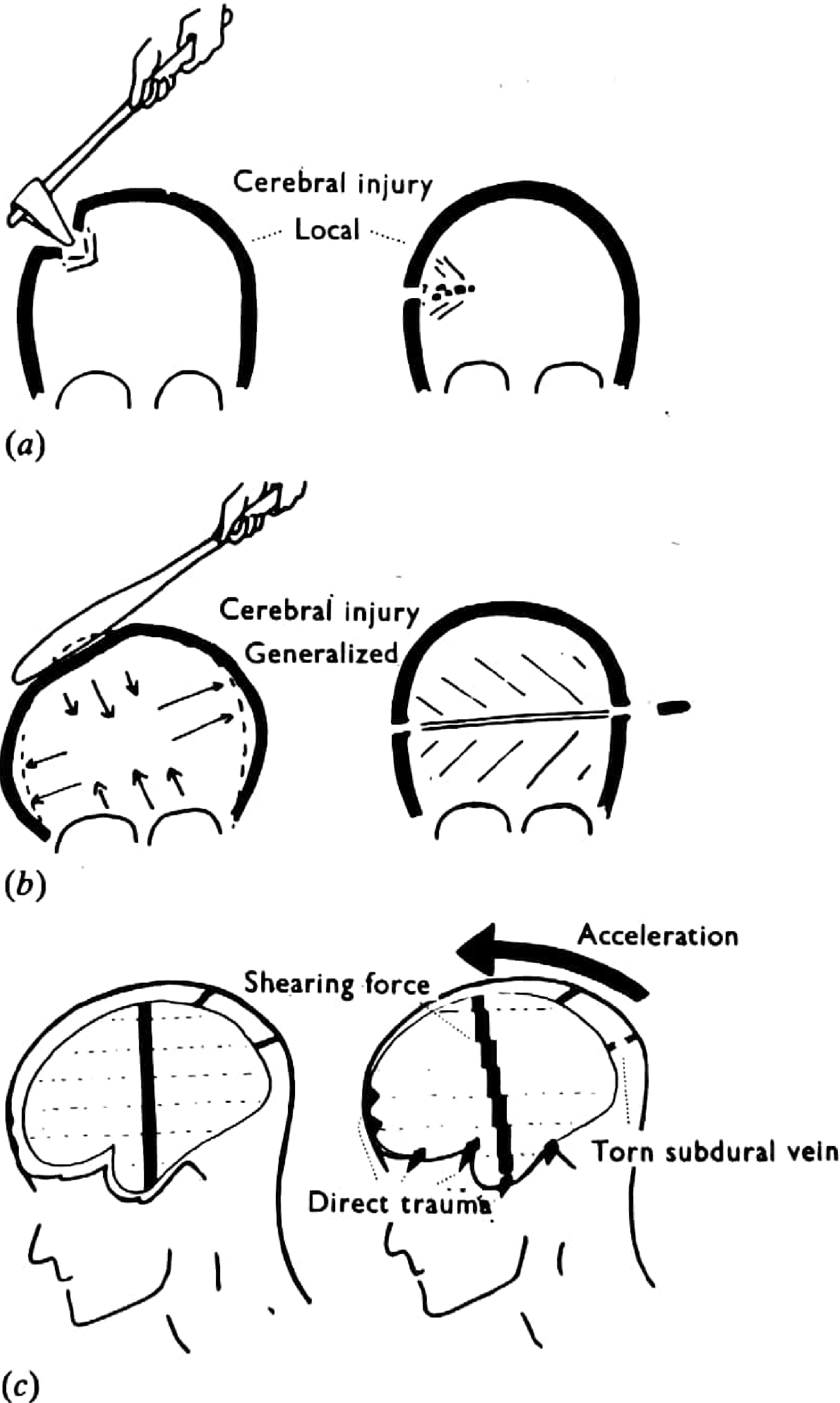
Diagram (c) shows how acceleration generates internal shearing forces and can tear bridging subdural veins - the whiplash mechanism.
Types of Brain Injury That Can Occur
1. Diffuse Axonal Injury (DAI)
This is the most important type. Schwartz's Principles of Surgery (11th ed.) explains:
"Diffuse axonal injury (DAI) is caused by damage to axons throughout the brain, due to rotational acceleration and then deceleration. Axons may be completely disrupted and then retract, forming axon balls. Small hemorrhages can be seen in more severe cases, especially on MRI. Hemorrhage is classically seen in the corpus callosum and the dorsolateral midbrain. DAI can be considered a severe form of concussion, often with irreversible consequence."
Bradley and Daroff's Neurology in Clinical Practice confirms that inertial acceleration-deceleration models (designed to mimic motor vehicle accidents) produce "pure acute subdural hematomas and diffuse axonal injury," with tissue-tear hemorrhages in the central white matter and gliding contusions at gray/white matter junctions.
2. Concussion / Mild TBI
Tintinalli's Emergency Medicine explains the neurochemical cascade triggered by the same acceleration-deceleration forces seen in whiplash:
"Acceleration and deceleration forces initiate a neurochemical cascade that results in neuronal membrane disruption and axonal stretching. The acute phase of injury is characterized by an increase in cerebral cellular energy demand coupled with insufficient energy substrate delivery, resulting in a metabolic crisis. This leads to alterations in neuronal depolarization, ion transport, glycolysis, mitochondrial function, and neurotransmitter release."
Key neurochemical events include:
- Indiscriminate neurotransmitter release
- Calcium influx and potassium efflux causing widespread depolarization
- Intracellular magnesium depletion (may persist for days)
- High intracellular calcium destroying microtubules within axons
- Reduced global and regional cerebral blood flow
3. Cerebral Contusions
Schwartz's describes contusions (bruises of the brain) occurring when deceleration forces slam brain tissue against bony skull surfaces. Frontal, occipital, and temporal poles are most vulnerable. Contre-coup injury - bruising on the brain surface opposite the point of impact - results specifically from deceleration of the brain against the skull, the same mechanism at play in whiplash.
4. Vascular Injuries
Pye's Surgical Handicraft notes that acceleration/deceleration forces can "avulse bridging veins," producing subdural hematomas. Late vascular complications have also been documented - Plum and Posner references cervical artery dissection as a late sequela of whiplash injury.
Why Brain Injury Is Often Missed After Whiplash
- Standard CT and MRI may appear normal even when there is genuine neuronal dysfunction (concussion is a "functional disturbance rather than a gross structural injury" - Tintinalli's)
- Cognitive symptoms (memory impairment, difficulty concentrating, mood change, fatigue) may be attributed solely to neck pain or anxiety
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry specifically lists whiplash among potential causes of traumatic brain injury in psychiatric evaluation, noting that symptoms such as "loss of consciousness, dizziness, unsteadiness, and gait abnormalities" may accompany it
Clinical Relevance
| Feature | Detail |
|---|---|
| Setting | Rear-end MVCs; also falls, sports, assault |
| Primary brain injuries | Concussion, DAI, contusion, subdural hematoma |
| Key symptom pattern | Headache, cognitive fog, memory difficulties, dizziness, mood changes |
| Imaging | Often normal on standard CT; MRI (especially gradient echo or susceptibility-weighted sequences) is more sensitive for DAI |
| Prognosis | Most recover, but a subset develop persistent post-concussive syndrome |
| Special risk | "Second-impact syndrome" - re-injury within 1-2 weeks of concussion carries markedly increased risk of severe brain injury |
Sources
- Adams and Victor's Principles of Neurology, 12th ed. - Definitions and Mechanisms of Head Injury
- Schwartz's Principles of Surgery, 11th ed. - Types of Closed Head Injury
- Tintinalli's Emergency Medicine, 9th ed. - Concussion Pathophysiology
- Bradley and Daroff's Neurology in Clinical Practice - Acceleration Concussion Models
- Pye's Surgical Handicraft, 22nd ed. - Head Injury Pathophysiology
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry - TBI in Psychological Evaluation
Can whiplash injuries causes brain injury?
Reading File
Finding Sources
Finding Sources
Searching PubMed
whiplash traumatic brain injury concussion
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
I now have thorough, authoritative textbook material across multiple sources. Here is the full answer:
Can Whiplash Injuries Cause Brain Injury?
Yes. This is well-established in neurology, surgery, and emergency medicine literature. Whiplash does not require a direct blow to the skull - the violent flexion-extension motion of the neck itself generates enough force inside the cranium to injure the brain through several distinct mechanisms.
The Core Mechanism
Adams and Victor's Principles of Neurology (12th ed.) states plainly:
"Unless the head is struck, the brain suffers no injury except in the few instances of violent flexion-extension (whiplash) of the neck and possibly in explosion-blast injury."
The key mechanical factors at play are:
- The differential mobility of the head on the neck and of the brain within the cranium
- The tethering of the upper brainstem, which allows the cerebral hemispheres to swing around it
- The brain striking against dural septa and bony prominences during this motion
- Shearing strains set up within the brain tissue itself
Pye's Surgical Handicraft (22nd ed.) summarizes it concisely:
"Acceleration/deceleration forces set up shearing strains within the brain, contuse the surfaces against the skull's bony ridges, and avulse bridging veins. The 'whiplash' mechanism also distorts the midbrain and brainstem, usually resulting in loss of consciousness and often alterations in vital signs."
The diagram below illustrates how acceleration forces generate internal shearing forces and can tear bridging subdural veins - the same forces at work in whiplash:
From Pye's Surgical Handicraft - Figure (c) shows the whiplash-type mechanism with acceleration generating internal shearing forces and avulsion of bridging veins.
Types of Brain Injury Caused by Whiplash
1. Concussion / Mild TBI
This is the most common. Grainger & Allison's Diagnostic Radiology notes that significant brain injury can occur with indirect trauma and no direct blow to the head when rotational and shearing forces are present, as in road traffic accidents - exactly the mechanism of whiplash.
Schwartz's Principles of Surgery (11th ed.) notes that the brain remains in a hypermetabolic state for up to one week after concussion, and is significantly more vulnerable to even minor re-injury during the first 1-2 weeks - a phenomenon called second-impact syndrome.
2. Diffuse Axonal Injury (DAI)
Schwartz's explains:
"Diffuse axonal injury (DAI) is caused by damage to axons throughout the brain due to rotational acceleration and then deceleration. Axons may be completely disrupted and then retract, forming axon balls. Hemorrhage is classically seen in the corpus callosum and the dorsolateral midbrain. DAI can be considered a severe form of concussion, often with irreversible consequence."
DAI is particularly important in whiplash because it can explain a poor neurological examination even when CT and standard MRI look normal. MRI with susceptibility-weighted imaging (SWI) or diffusion tensor imaging (DTI) is far more sensitive for detecting it.
3. Cerebral Contusions (Coup and Contre-Coup)
When the accelerating/decelerating brain collides with the rough inner surface of the skull, it bruises. Contusions appear bright on CT. Crucially, contre-coup injuries occur in brain tissue opposite the site of impact due to the brain decelerating against the skull - the same deceleration force central to whiplash. The frontal, occipital, and temporal poles are most vulnerable.
4. Vascular Injury
- Subdural hematoma - bridging veins are avulsed by the same acceleration-deceleration shearing forces
- Cervical artery dissection - documented as a late vascular sequela of whiplash injury (referenced in Plum and Posner's Stupor and Coma), and can lead to ischemic stroke
Why Brain Injury Is Frequently Missed After Whiplash
| Reason | Explanation |
|---|---|
| Normal standard imaging | Concussion is a functional, not structural, injury - CT and standard MRI are often normal |
| Symptom overlap | Headache, dizziness, and cognitive symptoms are attributed to the neck injury alone |
| No loss of consciousness | Many patients with genuine brain injury never lose consciousness |
| Delayed symptom onset | Signs of concussion/TBI may evolve over hours to days after injury |
Kaplan & Sadock's Comprehensive Textbook of Psychiatry specifically lists whiplash as a mechanism of traumatic brain injury in its psychiatric evaluation guidelines, alongside loss of consciousness, dizziness, unsteadiness, and gait abnormalities as TBI symptoms to screen for after whiplash.
Post-Concussion Syndrome After Whiplash
When brain injury does occur, a subset of patients develop post-concussion syndrome, characterized by persistent:
- Headache
- Dizziness and balance problems
- Inability to concentrate
- Impaired memory
- Irritability and mood changes
- Fatigue and sleep disturbance
(Swanson's Family Medicine Review)
These symptoms often persist for weeks to months and require cognitive rest and close physician follow-up.
Key Takeaway
Whiplash is not purely a musculoskeletal neck injury. The very same acceleration-deceleration forces that sprain cervical ligaments also transmit shearing, rotational, and compressive forces to the brain, capable of producing a spectrum from mild concussion to diffuse axonal injury and vascular complications. Any patient with whiplash who reports cognitive symptoms, persistent headache, dizziness, or altered consciousness should be evaluated for concurrent brain injury.
Sources:
- Adams and Victor's Principles of Neurology, 12th ed.
- Pye's Surgical Handicraft, 22nd ed.
- Schwartz's Principles of Surgery, 11th ed.
- Grainger & Allison's Diagnostic Radiology
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry
- Plum and Posner's Diagnosis and Treatment of Stupor and Coma
- Swanson's Family Medicine Review
This is a shared conversation. Sign in to Orris to start your own chat.