Hyperkalemia
Reading File
Finding Sources
Searching PubMed
hyperkalemia treatment management
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I now have everything needed for a comprehensive response. Let me compile it.
Hyperkalemia
Definition: Serum potassium > 5.5 mEq/L. It is potentially the most rapidly lethal electrolyte disturbance, often clinically silent until life-threatening cardiac arrhythmias develop.
Normal Potassium Homeostasis
- ~98% of total body K+ is intracellular (primarily in muscle); normal serum K+ is 3.5-5.0 mEq/L.
- The kidney is the primary route of excretion - aldosterone drives K+ secretion in the cortical collecting tubule (CCT) via ENaC and ROMK channels.
- Transcellular shifts are governed by insulin, catecholamines (beta-2), aldosterone, and acid-base status.
Causes
1. Pseudohyperkalemia (False Elevation)
- Traumatic hemolysis during blood draw (most common cause of a "high" lab value)
- Myeloproliferative disorders: thrombocytosis or extreme leukocytosis releasing K+ during clot formation in the sample tube
2. Increased K+ Load
- Exogenous: IV potassium infusion, inappropriate IV fluids, salt substitutes (KCl), transfusion of stored blood
- Endogenous cell breakdown: rhabdomyolysis, crush injuries, burns, hemolysis (mismatched transfusion), tumor lysis syndrome, GI bleeding with intestinal absorption
3. Transcellular Shift (K+ out of cells)
| Mechanism | Examples |
|---|---|
| Metabolic acidosis | H+/K+ exchange - H+ enters cells, K+ exits |
| Insulin deficiency | Loss of Na-K-ATPase stimulation |
| Beta-adrenergic blockade | Blocks beta-2 mediated cellular K+ uptake |
| Digitalis toxicity | Inhibits Na-K-ATPase directly |
| Hypertonicity/hyperosmolality | Solvent drag, cell shrinkage |
| Succinylcholine | Membrane depolarization, especially risky in CKD |
4. Decreased Renal Excretion (most common cause of sustained hyperkalemia)
- Advanced renal failure (CKD/AKI) - any etiology
- Hypoaldosteronism:
- Primary adrenal insufficiency (Addison's disease, adrenal hemorrhage)
- Type IV RTA (hyporeninemic hypoaldosteronism) - common in diabetic nephropathy
- Drugs impairing renal K+ excretion:
- ACE inhibitors / ARBs (suppress aldosterone)
- Potassium-sparing diuretics (spironolactone, eplerenone, amiloride, triamterene)
- NSAIDs - suppress renin release and reduce GFR
- Trimethoprim, heparin, calcineurin inhibitors
- Finerenone and other MRA class agents
Clinical Manifestations
Most patients are asymptomatic until K+ is significantly elevated.
Cardiac (most dangerous - present when K+ > 7 mEq/L)
Cardiac conduction delay is the most common and most dangerous manifestation. ECG changes progress in this sequence:
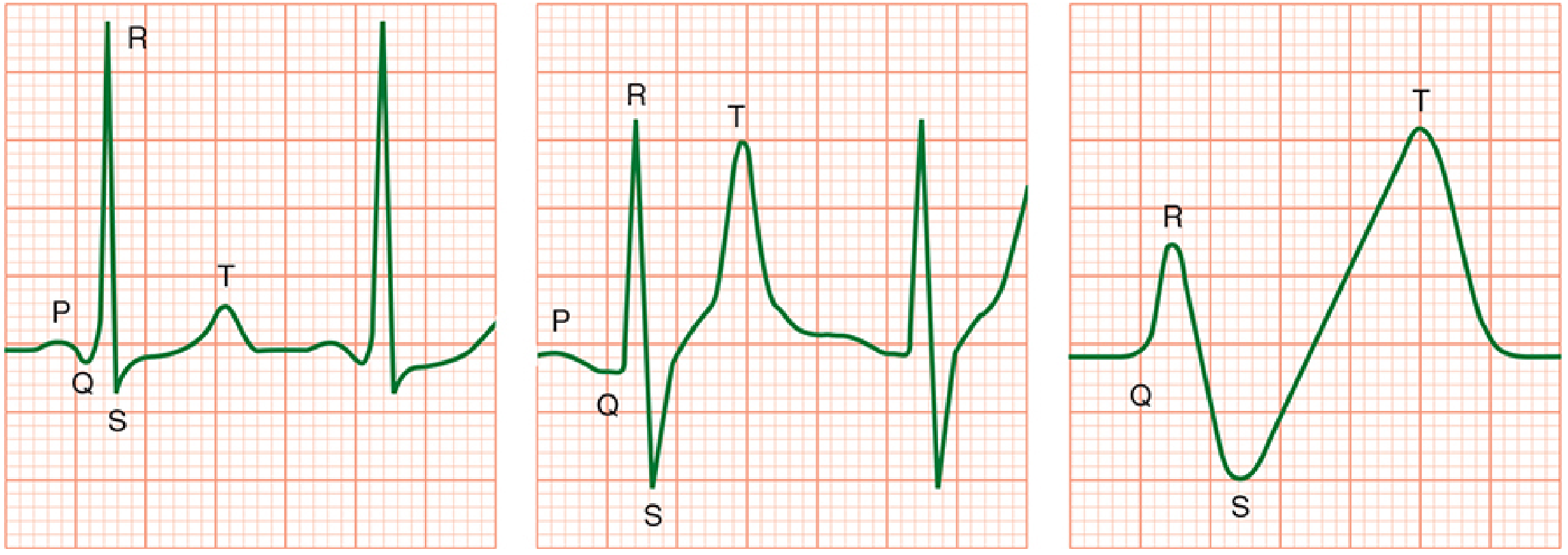
ECG progression: (Left) Normal. (Center) Peaked T waves and QRS widening. (Right) Sine wave pattern preceding arrest.
Sequential ECG changes:
- Symmetrically peaked (tall, narrow, "tented") T waves - first sign, often with shortened QT
- Prolonged PR interval
- Widening of the QRS complex - ominous
- Loss of P wave
- Loss of R-wave amplitude / ST depression
- Sine wave pattern - QRS merges with T wave
- Ventricular fibrillation / Asystole
Key point: A normal ECG does NOT exclude dangerous hyperkalemia. Hypocalcemia, hyponatremia, and acidosis worsen the cardiac effects.
Neuromuscular
- Skeletal muscle weakness (generally not seen until K+ > 8 mEq/L)
- Ascending paralysis (rare)
- Paresthesias
Treatment
Treatment Flowchart
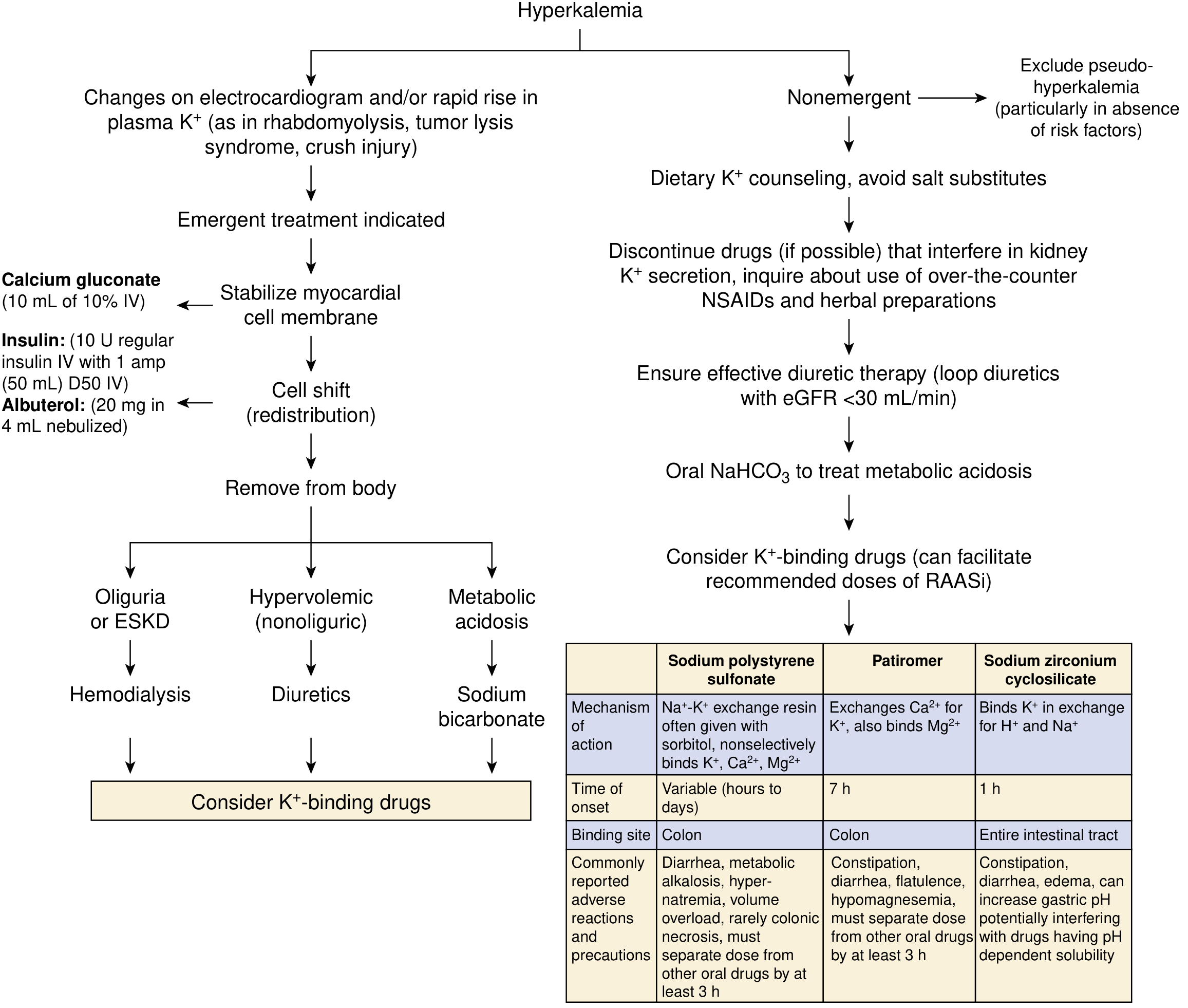
NKF Primer on Kidney Diseases, 8e - emergent vs. non-emergent management
Treatment uses three physiologic strategies in order:
Step 1 - Membrane Stabilization (Immediate, minutes)
Indication: ECG changes present, OR K+ > 6-6.5 mEq/L with symptoms
| Agent | Dose | Mechanism | Onset |
|---|---|---|---|
| Calcium gluconate 10% | 10 mL IV over 1-2 min; repeat in 3-5 min if no ECG improvement | Raises action potential threshold, stabilizes membrane. Does NOT lower K+ | Immediate (~1-2 min) |
| Calcium chloride 10% | 3-5 mL IV via central line | Same; more elemental Ca2+ per ampule; avoid peripherally (causes tissue necrosis) | Immediate |
Caution in digoxin toxicity: Calcium potentiates digoxin toxicity - administer slowly over 20-30 min as "calcium sandwich" with sodium bicarbonate.
Step 2 - Transcellular Shift (Temporizing, 15-60 min)
| Agent | Dose | Mechanism | Onset |
|---|---|---|---|
| Regular insulin + Dextrose | 10 units IV regular insulin + 50 mL D50W (1 amp) bolus, then D5W at 100 mL/h | Activates Na-K-ATPase, drives K+ into cells | 15-30 min; peak ~60 min |
| Nebulized albuterol | 20 mg (use concentrated 5 mg/mL form) nebulized over 10 min | Beta-2 stimulation activates Na-K-ATPase | 30 min; additive to insulin |
| Sodium bicarbonate | 50-100 mEq IV (if pH < 7.3) | Alkalosis drives K+ into cells; also enhances renal excretion | 15-30 min |
Note: 20-40% of patients are resistant to albuterol. Never give dextrose without insulin in patients with poor endogenous insulin production - the resulting hyperglycemia can paradoxically worsen hyperkalemia. Monitor glucose closely.
Step 3 - Remove K+ from the Body (Definitive)
| Modality | When | Notes |
|---|---|---|
| Furosemide (loop diuretic) | Adequate renal function, not hypovolemic | Enhances renal K+ excretion; give by slow infusion (not bolus) due to ototoxicity risk |
| Sodium polystyrene sulfonate (Kayexalate) | Can wait hours | Na-K exchange resin in colon; onset 1-2 h PO or <30 min rectally; risk of colonic necrosis (especially with sorbitol) |
| Patiromer | Non-emergent, chronic | Ca2+/K+ exchange in colon; onset ~7 h; constipation, hypomagnesemia; separate from other drugs by 3 h |
| Sodium zirconium cyclosilicate (ZS-9) | Non-emergent to semi-urgent | Binds K+ in exchange for H+ and Na+; onset ~1 h; entire GI tract |
| Hemodialysis | Oliguric/anuric or ESKD, life-threatening | Fastest and most reliable K+ removal; definitive treatment in renal failure |
Emergent vs. Non-Emergent Algorithm
Emergent (ECG changes, rapid rise, K+ >6.5):
Calcium gluconate → Insulin + dextrose + albuterol → Remove (dialysis, diuretics, or bicarb based on context)
Non-Emergent (mild, asymptomatic, no ECG changes):
- Exclude pseudohyperkalemia
- Dietary K+ restriction, avoid salt substitutes
- Discontinue offending drugs (NSAIDs, ACE-I, K+-sparing diuretics)
- Loop diuretics if renal function allows
- Oral NaHCO3 if metabolic acidosis present
- K+-binding agents (patiromer or ZS-9 preferred over SPS for chronic management, especially to allow continued RAAS inhibitor use)
Special Situations
- CKD patients: Chronically tolerate K+ slightly above 6 mEq/L but are at high risk with any additional load. Succinylcholine use should be cautious. Furosemide requires higher doses.
- Cardiac arrest with unknown cause: Assume hyperkalemia and treat empirically with calcium gluconate while resuscitating.
- Digoxin toxicity: Use calcium cautiously (slow infusion); hypomagnesemia co-treatment required.
- Post-RAAS inhibitor therapy: Patiromer and ZS-9 allow patients to remain on ACE inhibitors/ARBs/MRAs despite hyperkalemia - important for CKD and heart failure outcomes.
Recent Evidence (PubMed, 2024-2026)
A 2025 network meta-analysis (PMID 40542996) confirmed that novel K+-binding agents (patiromer, ZS-9) reduce hyperkalemia and enable optimization of RAAS inhibitor therapy in CKD and heart failure patients - supporting their use as adjuncts to maintain cardiorenal-protective medications.
Sources: NKF Primer on Kidney Diseases 8e, Morgan & Mikhail's Clinical Anesthesiology 7e, Tintinalli's Emergency Medicine, Rosen's Emergency Medicine, Medical Physiology (Boron & Boulpaep), Brenner & Rector's The Kidney
This is a shared conversation. Sign in to Orris to start your own chat.