Temporomandibular joint
Reading File
Finding Sources
Finding Sources
Searching PubMed
"temporomandibular joint" anatomy disorders
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information. Let me compile the full answer.
Temporomandibular Joint (TMJ)
Overview
The TMJ is a bilateral synovial joint between the condyle of the mandible and the mandibular (glenoid) fossa of the temporal bone, just anterior to the external auditory canal. It is the most frequently used joint in the body, involved in mastication, speech, and swallowing. It has several unique features that set it apart from other synovial joints.
Unique Anatomical Features
- Divided joint space - an intra-articular disc divides the cavity into upper and lower compartments
- Fibrocartilage articular surface - unlike most synovial joints, the articular surfaces are covered by fibrous tissue (not hyaline cartilage), reflecting the joint's intramembranous development
- Secondary condylar cartilage - present beneath the fibrous articular surface until puberty (~16 years); disappears with skeletal maturity
- Tooth-influenced movement - occlusal contacts directly modify joint kinematics
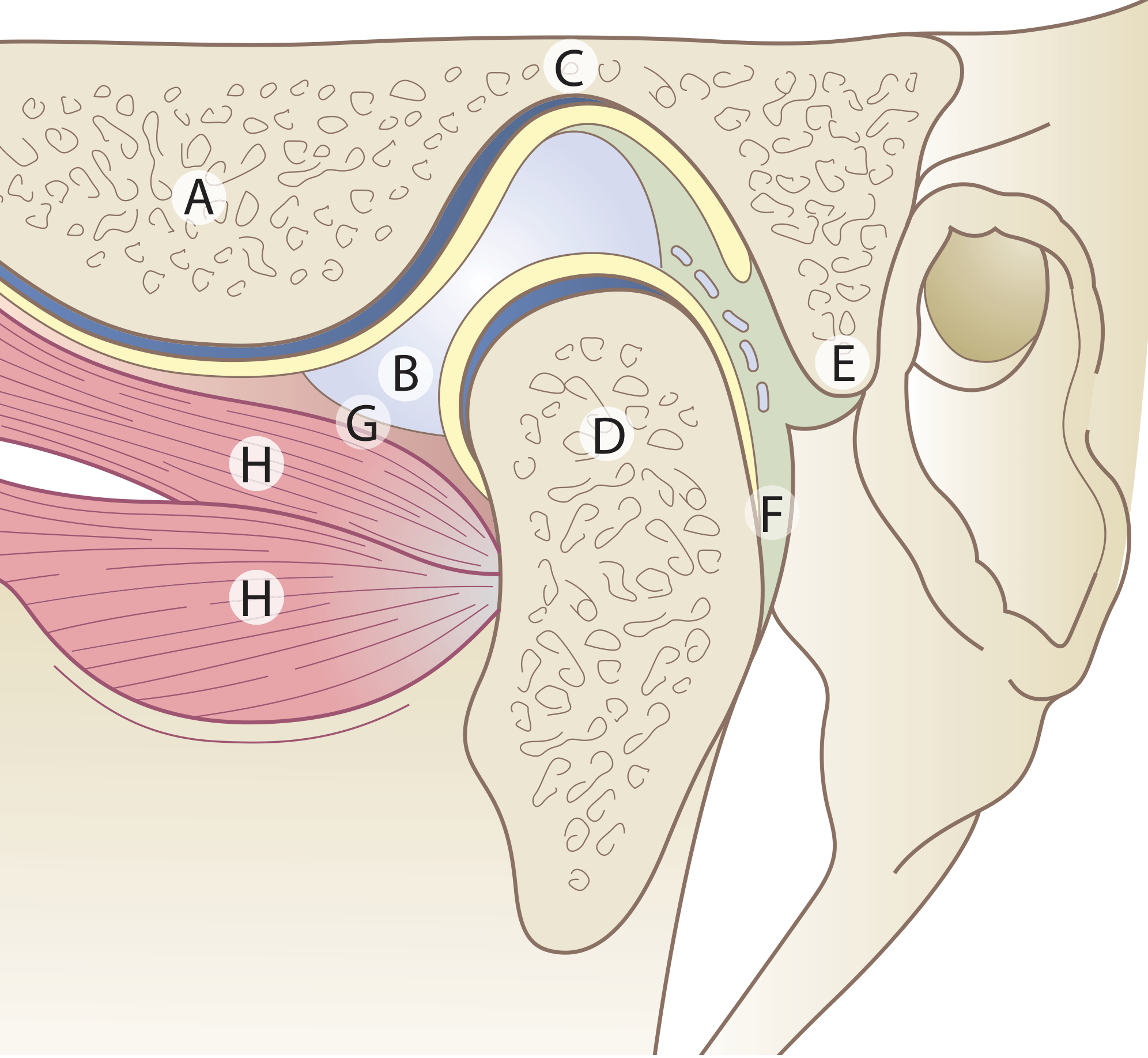
A = Articular eminence; B = Articular disc; C = Mandibular fossa; D = Condyle; E = Upper lamina (fibro-elastic); F = Lower lamina (non-elastic); G = Capsule of joint; H = Lateral pterygoid muscle. Yellow = upper and lower joint cavities.
Bony Components
- Mandibular condyle: The oval-shaped articular head of the mandible. Its articular surfaces are the anterior and superior aspects. The neck of the condyle is a frequent fracture site. The pterygoid fovea on the anterior neck marks the attachment of the lateral pterygoid.
- Mandibular (glenoid) fossa + articular eminence: The concave fossa and its anterior convex eminence form the temporal component. The shape mismatch between condyle and fossa is part of why the intra-articular disc is needed.
The Articular Disc (Meniscus)
A biconcave fibrocartilaginous structure that divides the joint into:
| Compartment | Type of movement |
|---|---|
| Upper (disc-temporal) | Gliding / translation |
| Lower (disc-condylar) | Hinge / rotation |
- The disc is thickest at its posterior band, thinnest centrally (intermediate zone), and thicker again anteriorly
- Anterior attachment: fibrous bands to the articular eminence above and condyle below; the superior head of the lateral pterygoid inserts here in ~60% of cases
- Posterior attachment: the retrodiscal tissue (bilaminar zone)
- Superior lamina: loose, highly vascular, elastic fibres - attaches to squamotympanic fissure; provides elastic recoil to return disc on closing
- Inferior lamina: relatively avascular, inelastic - attaches to posterior condyle
- Medial/lateral attachments: to the joint capsule and poles of the condyle via triangular connective tissue zones
- Retrodiscal tissue volume increases 4-5x through venous engorgement as the jaw opens
Joint Capsule
- Attached above to the mandibular fossa, anteriorly to just in front of the articular eminence crest, posteriorly to the squamotympanic and petrotympanic fissures
- Below, attached to the neck of the condyle
- The capsule is thin and relatively weak - particularly at the anteromedial portion, where loose synovial tissue allows translation; this anatomical weakness is one reason anterior dislocations occur
Ligaments
| Ligament | Origin | Insertion | Function |
|---|---|---|---|
| Temporomandibular (lateral/collateral) | Articular tubercle + zygomatic arch | Neck of condyle (lateral + posterior) | Limits lateral movement; principal joint ligament |
| Sphenomandibular | Spine of sphenoid | Lingula of mandible | Accessory; limits distraction |
| Stylomandibular | Styloid process | Angle + posterior border of ramus | Accessory; limits protrusion |
| Retinacular (recently described) | Articular eminence | Fascia over masseter (angle of mandible) | May maintain blood circulation during mastication |
Innervation
Branches of the mandibular nerve (V3):
- Auriculotemporal nerve (primary)
- Masseteric nerve
- Deep temporal nerves
Proprioceptive nerve endings are functionally important for reflex control of mastication. The proximity of the auriculotemporal nerve also explains why TMJ pathology commonly presents as referred ear pain.
Blood Supply
- Superficial temporal artery (primary)
- Maxillary artery - anterior tympanic and deep auricular branches
- Contributions from deep temporal and transverse facial arteries
Movements
| Movement | Compartment | Muscles |
|---|---|---|
| Mouth opening (inferior head of lateral pterygoid + digastric) | Lower (rotation) then upper (translation) | Lateral pterygoid (inf.), digastric, geniohyoid, mylohyoid |
| Protrusion | Upper | Lateral pterygoid (both heads), medial pterygoid |
| Retrusion | Upper | Posterior temporalis, digastric |
| Mouth closing | Lower then upper | Temporalis, masseter, medial pterygoid |
| Lateral excursion | Both | Ipsilateral temporalis; contralateral pterygoids |
- Normal maximal mouth opening (measured between upper and lower incisors): 3-6 cm
- The condyle undergoes rotation then anterior translation during opening (the meniscus translates with it)
Clinical Examination
- Palpate by placing a finger just anterior to the external auditory canal while the patient opens/closes and moves the jaw side to side
- Assess vertical movement: measure distance between upper and lower incisors at maximal opening (normal 3-6 cm)
- Assess lateral movement using incisors as landmarks
- Note: audible or palpable crepitus or clicking may be present with or without severe arthritis
Clinical Conditions
TMJ Disorders (TMD)
Multifactorial; common symptoms include jaw/face pain, clicking/popping, and limited mouth opening. Estimated to affect a considerable proportion of the population.
Pathophysiology of disc displacement:
- Inflammatory or degenerative damage to articular surfaces increases friction on the disc
- Disc gradually shifts anteromedially from its normal position
- The posterior retrodiscal tissue - now between bony surfaces - undergoes abnormal loading, loses structure, becomes vascularised, and can eventually perforate
- Degenerative changes can expose bone (osteoarthritic change)
- Synovial fluid in TMD shows elevated pro-inflammatory cytokines (IL, TNF), matrix metalloproteinases, and VEGF
Clicking/popping: occurs when the displaced disc catches up with the condyle during opening or closing ("reciprocal clicking")
Closed lock: disc fails to translate fully - limits mouth opening
Bruxism association: TMD arthralgias without inflammatory arthritis are considered by many to be a form of myofascial pain (similar to fibromyalgia), often linked to bruxism
Inflammatory Arthritis
- Both juvenile and adult rheumatoid arthritis can involve the TMJ
- Micrognathia may develop in children if the TMJ is involved, due to arrested mandibular bone growth
- Other arthritides (psoriatic, ankylosing spondylitis, reactive arthritis) may also affect the joint
Anterior Dislocation
- Occurs after any wide mouth opening (yawning, dental procedures, vomiting)
- Condyle translates anterior to the articular eminence and becomes trapped there by masseter/temporalis spasm
- Unilateral: jaw deviates away from affected side
- Bilateral: significant jaw protrusion, open-mouth drooling, garbled speech
- A depression is palpable just anterior to the ear
- Reduction: patient seated upright, operator places thumbs/index fingers in buccal sulcus, applies downward pressure on posterior mandible while rotating chin upward and backward; protect fingers from bite when jaws snap shut
- Rule out fracture before reduction with plain film or Panorex
Trauma/Internal Derangement
- Tearing of the meniscus or collateral ligaments causes abnormal translation - clicking, popping, or incomplete opening
- Paediatric patients with post-traumatic TMJ derangement are prone to asymmetric facial growth and retrognathia
- Management: soft diet, avoid wide opening, refer to oral surgeon with TMJ expertise
Imaging
| Modality | Use |
|---|---|
| Plain film / Panorex | Fracture screening; pre-reduction |
| CT | Fractures, bony anatomy, TMJ arthrosis |
| MRI | Gold standard for disc position, disc morphology, retrodiscal tissue, early inflammatory change |
| Arthrography | Historically used; largely replaced by MRI |
| Ultrashort TE (UTE) MRI | Emerging; quantitative disc/cartilage assessment |
Treatment Approaches
- Conservative: soft diet, NSAIDs, muscle relaxants, occlusal splints, physiotherapy
- Arthrocentesis: lavage and aspiration of the joint - reduces inflammatory mediators, improves mobility; effective as initial treatment for TMJ arthropathy
- Arthroscopy: for internal derangements refractory to conservative treatment
- Open surgery: reserved for failures of arthroscopy; includes disc repositioning, discectomy, or total joint replacement
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Ch. 41 | Firestein & Kelley's Textbook of Rheumatology, Ch. on Peripheral Joints | Rosen's Emergency Medicine, Ch. 34 & 56 | Cummings Otolaryngology Head and Neck Surgery, Ch. 19
This is a shared conversation. Sign in to Orris to start your own chat.