Hepatitis
Reading File
Asking for Preferences
All
Finding Sources
Searching the Web
hepatitis A B C D E overview classification pathophysiology treatment 2024
Reading File
Reading File
Finding Sources
Searching PubMed
viral hepatitis review
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Excellent - I now have comprehensive data from Goldman-Cecil Medicine, Park's Preventive Medicine, and Frameworks for Internal Medicine. I have enough to write a thorough, well-organized answer.
Hepatitis - Complete Clinical Overview
Hepatitis means inflammation of the liver. It can be caused by viruses, alcohol, drugs, autoimmune disease, or metabolic disorders. Viral hepatitis accounts for over 50% of acute hepatitis cases globally.
Classification at a Glance
| Feature | HAV | HBV | HCV | HDV | HEV |
|---|---|---|---|---|---|
| Genome | +ssRNA | dsDNA | +ssRNA | -ssRNA (satellite) | +ssRNA |
| Transmission | Fecal-oral | Parenteral / sexual / vertical | Parenteral (mainly blood) | Parenteral (requires HBV) | Fecal-oral |
| Incubation | 15-45 days | 45-180 days | 15-150 days | 30-45 days | 20-60 days |
| Chronicity | None | Yes (5% adults; 90% neonates) | Yes (50-80%) | Yes (in HBV carriers) | Rarely (immunocompromised) |
| Vaccine | Yes | Yes | No | HBV vaccine protects | Yes (HEV 239; not widely available) |
(Sources: Goldman-Cecil Medicine; Park's Textbook of Preventive & Social Medicine)
Pathophysiology (General)
A hepatotropic virus invades hepatocytes, triggering an immune-mediated inflammatory response. The key events:
- Viral entry into hepatocytes via specific surface receptors
- Innate immune activation - interferon release, NK cell recruitment
- Cytotoxic T lymphocyte (CTL) attack on infected hepatocytes - responsible for most of the liver damage (not the virus directly)
- Hepatocyte necrosis and apoptosis - leads to elevated transaminases (AST, ALT)
- Cholestasis - impaired bile flow causes jaundice, dark urine, pale stools
- Resolution or chronicity - depends on the virus and host immune response
In fulminant hepatic failure, massive hepatocyte necrosis leads to encephalopathy, coagulopathy, and multiorgan failure.
Clinical Phases
All acute viral hepatitis follows a similar pattern:
1. Incubation phase - Asymptomatic; viral replication occurring
2. Pre-icteric (prodromal) phase (1-2 weeks)
- Fatigue, malaise, anorexia, nausea, vomiting, right upper quadrant (RUQ) pain
- Flu-like symptoms: fever, headache, myalgia
- Immune-complex-mediated: rash, urticaria, arthralgias (10-20% of cases)
- Leukopenia with relative lymphocytosis
3. Icteric phase (1-3 weeks)
- Jaundice, dark urine (bilirubinuria), acholic (pale) stools
- Pruritus (in cholestatic forms)
- Hepatomegaly, possible splenomegaly
- LFTs: ALT/AST often >10x upper limit of normal (frequently >1000 U/L)
- Elevated total and direct bilirubin
4. Recovery phase
- Gradual normalization of LFTs and resolution of symptoms
Fulminant hepatitis (rare): personality change, encephalopathy, hemorrhage, coma - requires urgent assessment for liver transplantation.
Hepatitis A (HAV)
Virus: Picornaviridae family, non-enveloped +ssRNA
Transmission: Fecal-oral - contaminated food/water, shellfish, person-to-person contact. Most common in areas with poor sanitation.
Epidemiology: WHO estimates ~1.4 million cases/year worldwide. In high-endemic areas, 90% of children are infected by age 10 (mostly subclinical). In low-endemic areas, susceptibility persists into adulthood.
Clinical outcomes:
| Outcome | Children | Adults |
|---|---|---|
| Sub-clinical (inapparent) | 80-95% | 10-25% |
| Icteric disease | 5-20% | 75-90% |
| Mortality | 0.1% | 0.3-2.1% |
| Chronic disease | None | None |
(Park's Textbook of Preventive & Social Medicine)
- Relapsing cholestatic hepatitis occurs in 3-20% before full recovery
- HAV is the most common cause of relapsing cholestatic hepatitis
- No chronic form - always self-limited
Diagnosis:
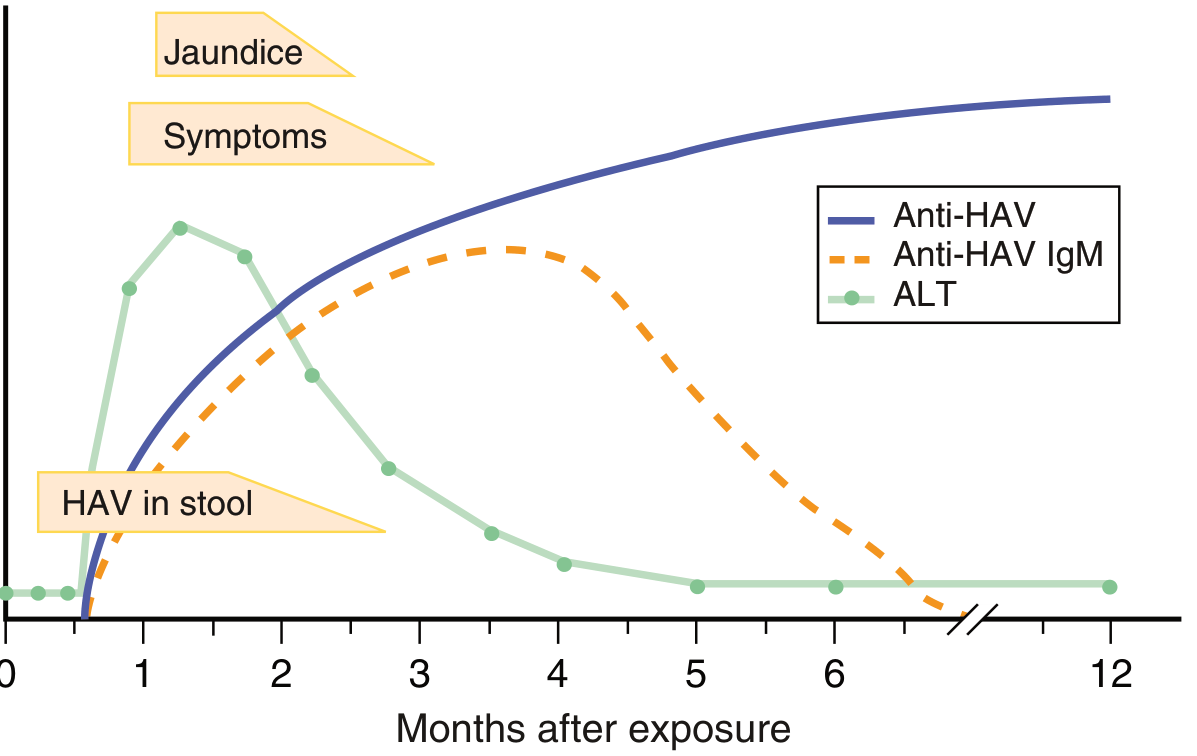
- Acute infection: Anti-HAV IgM (peaks at ~2 months, clears by 4-12 months) - diagnostic
- Past immunity: Anti-HAV IgG (persists for decades/lifetime)
- HAV RNA detectable in stool 2 weeks before to 2 weeks after jaundice onset
Treatment: No specific antiviral. Supportive care. Hospitalize severe cases; assess for transplant in acute liver failure.
Prevention:
- Inactivated vaccine (2 doses, 6-18 months apart) - ~94% protective efficacy, lifelong protection
- Live attenuated vaccine (single dose, used in China)
- Combination HAV+HBV and HAV+typhoid vaccines available
- Human immunoglobulin (IG): 80-90% effective if given within 14 days of exposure; protection lasts 1-5 months
- Improved sanitation and hand hygiene
(Goldman-Cecil Medicine; Park's Textbook)
Hepatitis B (HBV)
Virus: Hepadnaviridae, partially double-stranded DNA. Contains surface antigen (HBsAg), core antigen (HBcAg), and e antigen (HBeAg).
Transmission: Parenteral, sexual, and vertical (mother-to-child). Most chronic infections worldwide are acquired at birth or in early childhood.
Epidemiology: WHO (2024) estimates 240 million people living with chronic HBV, with 0.9 million new infections/year.
Key Serological Markers:
| Marker | Meaning |
|---|---|
| HBsAg (+) | Active HBV infection (acute or chronic) |
| Anti-HBs (+) | Immunity (past infection or vaccination) |
| HBeAg (+) | Active viral replication, high infectivity |
| Anti-HBe (+) | Low-level replication, resolving infection |
| Anti-HBc IgM (+) | Acute HBV infection |
| Anti-HBc IgG (+) | Past or chronic HBV exposure |
| HBV DNA | Quantifies viral load; guides treatment |
"Window period": When HBsAg has cleared but anti-HBs not yet detectable - anti-HBc IgM is the only positive marker.
Outcomes by age of infection:
- Neonatal/perinatal infection: 85-95% risk of chronicity
- Early childhood: ~30% chronicity
- Adult infection: 95-99% spontaneous resolution; fulminant hepatitis in ~0.1%
- In women HBeAg+ during pregnancy: ~90% vertical transmission without prophylaxis
Chronic HBV complications: Cirrhosis, hepatocellular carcinoma (HCC), portal hypertension, hepatic failure
Treatment:
- Acute HBV: Supportive - no antiviral therapy (self-resolves in 95-99% of adults)
- Chronic HBV: Antivirals - first-line agents include tenofovir (TDF or TAF) or entecavir; pegylated interferon-alpha is an alternative. Goal: suppress HBV DNA, prevent cirrhosis/HCC.
- In pregnancy: Tenofovir preferred (potent, safe, low resistance risk)
- Post-exposure prophylaxis (HCP): Hepatitis B immunoglobulin (HBIG) 0.06 mL/kg IM within 96h + start vaccine series (if unvaccinated)
Prevention:
- HBV vaccine (3 doses: 0, 1, 6 months) - safe, effective, >95% seroconversion
- Universal infant vaccination has dramatically reduced transmission
- Neonatal: HBIG + vaccine within 12 hours of birth if mother is HBsAg+
- The 2025 AGA guideline on HBV reactivation (PMID 39863345) also addresses prevention in immunosuppressed patients receiving biologics/chemotherapy
Hepatitis C (HCV)
Virus: Flaviviridae family, genus Hepacivirus. +ssRNA. Six major genotypes (1-6); genotype 1 is most common globally.
Transmission: Almost exclusively blood-borne. Main routes:
- Intravenous drug use (60-80% of new cases in developed countries)
- Unsafe medical/surgical procedures, blood transfusions (in developing countries)
- Nosocomial (contaminated equipment)
- Sexual transmission is less efficient than HBV; perinatal ~5-6%
Epidemiology: ~8 million chronically infected worldwide; ~1.5 million new infections/year.
Chronicity: 50-80% of acutely infected individuals develop chronic HCV. This is the highest chronicity rate among hepatitis viruses.
Clinical features:
- Acute HCV is often asymptomatic or mildly symptomatic - frequently goes undetected
- Chronic HCV: progressive liver fibrosis over decades, cirrhosis in ~20%, HCC
Diagnosis:
- Screening: Anti-HCV antibody (by ELISA/chemiluminescent assay)
- Confirmation: HCV RNA by PCR (detectable within weeks of infection)
- Genotyping guides treatment selection
Treatment:
- Acute HCV: Antiviral treatment indicated (because of 50-80% chronicity risk). Pegylated interferon ± ribavirin historically used; now direct-acting antivirals (DAAs) are preferred.
- Chronic HCV: DAA combinations achieve >95% sustained virological response (SVR/cure)
- Pan-genotypic regimens: sofosbuvir/velpatasvir (12 weeks), glecaprevir/pibrentasvir (8-12 weeks)
- SVR = undetectable HCV RNA 12 weeks after treatment = functional cure
- No vaccine available
- No role for post-exposure immunoglobulin
- Pregnancy: treatment not recommended during pregnancy; initiate post-delivery
Hepatitis D (HDV) - Delta Hepatitis
Virus: Defective -ssRNA virus. Requires HBV surface antigen (HBsAg) for its own envelopment - cannot infect independently of HBV.
Transmission: Same routes as HBV (parenteral, sexual). Affects ~5% of HBsAg carriers globally.
Two patterns of infection:
- Co-infection (HDV + HBV simultaneously): usually self-limited; higher risk of fulminant hepatitis
- Superinfection (HDV in a chronic HBV carrier): often leads to chronic HDV infection, rapid progression to cirrhosis, worse prognosis
Diagnosis: Anti-HDV antibodies; HDV RNA by PCR
Treatment: Pegylated interferon-alpha (limited efficacy). Bulevirtide (entry inhibitor) was approved in Europe in 2020 and shows promising results.
Prevention: HBV vaccination prevents HDV (since HDV cannot exist without HBV).
Hepatitis E (HEV)
Virus: Hepeviridae family. +ssRNA. 8 genotypes.
- Genotypes 1 & 2: Strictly human; fecal-oral, waterborne epidemics in Asia/Africa
- Genotypes 3 & 4: Zoonotic (pigs, wild boar, deer); sporadic cases in Europe, US, Japan
- Now considered the most common cause of acute viral hepatitis worldwide
Transmission: Fecal-oral (contaminated water, undercooked meat from infected animals)
Epidemiology: ~20 million infections/year; ~3.3 million symptomatic cases.
Clinical features:
- Incubation: 3-8 weeks
- Usually mild and self-limited in immunocompetent adults
- Severe disease in pregnant women - particularly genotypes 1 & 2: mortality up to 20-25% in the third trimester (fulminant hepatic failure)
- Chronic HEV in immunocompromised patients (transplant recipients, HIV) - especially genotype 3
- Neurological complications: Guillain-Barré syndrome association
Diagnosis: Anti-HEV IgM (appears within 6 weeks, persists 3-12 months); HEV RNA in stool/serum
Treatment: Self-limiting; no treatment needed for most. Ribavirin monotherapy for severe/fulminant cases and chronic HEV in immunocompromised. Reduce immunosuppression in organ transplant recipients.
Prevention: Improved sanitation, water treatment, cooking meat thoroughly. HEV 239 vaccine (Hecolin) licensed in China.
Diagnosis - Key Laboratory Approach
LFTs in acute hepatitis:
- AST, ALT: Often >10x ULN (frequently >1000 U/L)
- Bilirubin: Elevated total and direct
- ALP/GGT: Elevated in cholestatic forms
- PT/INR: Elevated in severe disease (reflects synthetic function)
Serological algorithm:
Suspected acute hepatitis
↓
Anti-HAV IgM → HAV
HBsAg + Anti-HBc IgM → Acute HBV
Anti-HCV + HCV RNA → HCV
Anti-HDV (in HBsAg+ patient) → HDV
Anti-HEV IgM → HEV
Non-Viral Causes of Hepatitis
- Alcoholic hepatitis: AST:ALT ratio >2:1; tender hepatomegaly, fever, jaundice
- Drug-induced liver injury (DILI): Paracetamol, INH, statins, herbal remedies
- Autoimmune hepatitis: Young women; ANA, anti-smooth muscle antibodies, elevated IgG; responds to steroids
- NAFLD/NASH: Metabolic syndrome association; now the most common cause of chronic liver disease in developed countries
- Other viruses: CMV (owl's eye inclusions), EBV, HSV (vesicular rash; acyclovir), VZV
Complications
| Complication | Associated Virus |
|---|---|
| Fulminant hepatic failure | HAV (rare), HBV, HDV co-infection, HEV (pregnancy) |
| Cirrhosis | HBV, HCV, HDV |
| Hepatocellular carcinoma (HCC) | HBV (even without cirrhosis), HCV |
| Portal hypertension | HBV, HCV (via cirrhosis) |
| Cryoglobulinemia | HCV |
| Glomerulonephritis | HBV (membranous), HCV (membranoproliferative) |
| Aplastic anemia | Seronegative hepatitis (idiopathic) |
Summary Table
| HAV | HBV | HCV | HDV | HEV | |
|---|---|---|---|---|---|
| Chronicity | No | Yes | Yes | Yes (superinfection) | Rarely |
| Treatment | Supportive | Tenofovir / Entecavir | DAAs (cure >95%) | Peg-IFN / Bulevirtide | Supportive / Ribavirin |
| Vaccine | Yes | Yes | No | (HBV vaccine protective) | Limited (China only) |
| Most at risk | Travellers, children | Neonates, HCWs | IDUs, transfusion | HBV carriers | Pregnant women, travellers |
Key references:
- Goldman-Cecil Medicine, Chapter 134 (Acute Viral Hepatitis)
- Park's Textbook of Preventive and Social Medicine, Viral Hepatitis chapter
- Frameworks for Internal Medicine, Infectious Causes of Hepatocellular Injury
- AGA 2025 Clinical Practice Guideline on HBV Reactivation (PMID 39863345)
- WHO Hepatitis B Fact Sheet 2024
This is a shared conversation. Sign in to Orris to start your own chat.