RESPIRATORY movement clinical anatomy
Respiratory Movement: Clinical Anatomy
Overview
1. Thoracic Dimensions That Change During Breathing
| Direction | Mechanism | Movement |
|---|---|---|
| Vertical | Diaphragm contraction/relaxation | Increases with inspiration |
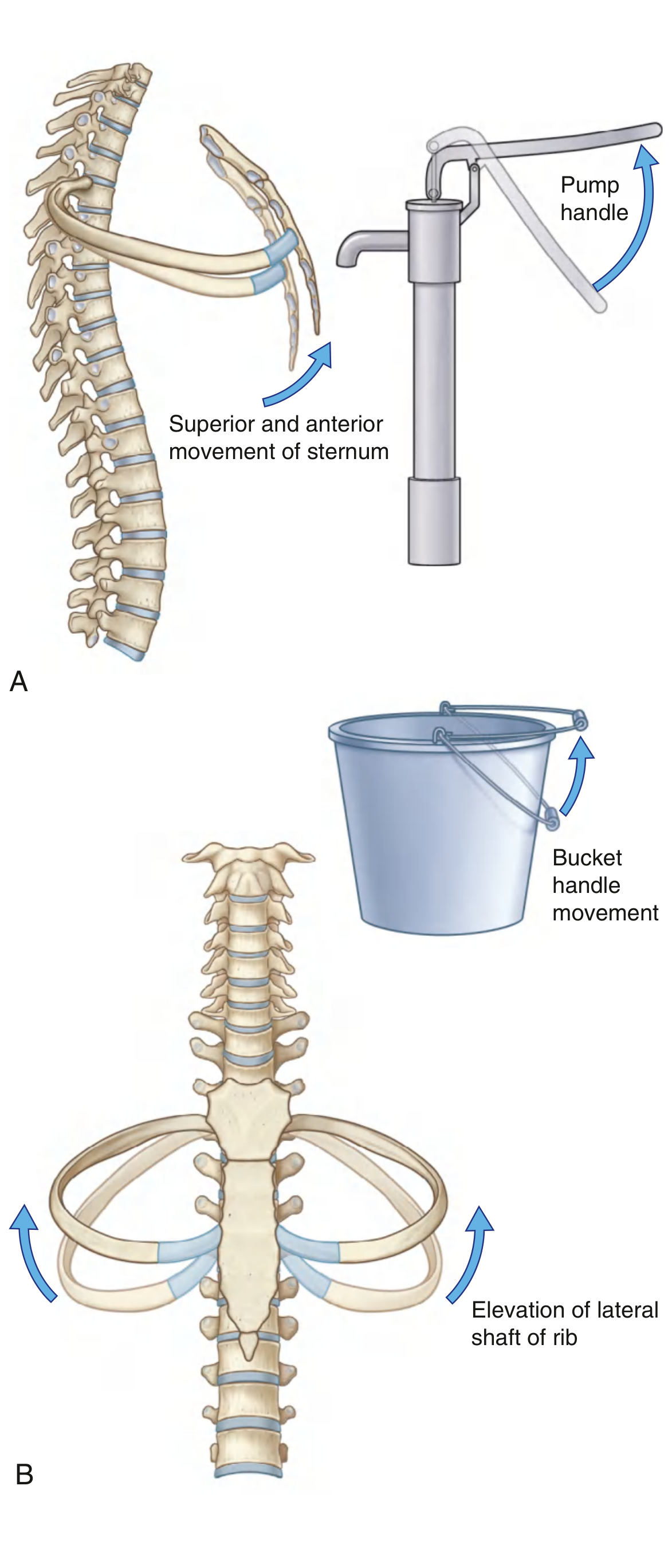
| Anteroposterior | Pump handle rib elevation | Sternum moves up and forward |
| Lateral | Bucket handle rib elevation | Lateral shafts of ribs swing outward |
2. Movements of the Thoracic Wall
Pump Handle Movement (Anteroposterior)
Bucket Handle Movement (Lateral)
"Any muscles attaching to the ribs can potentially move one rib relative to another and therefore act as accessory respiratory muscles. Muscles in the neck and the abdomen can fix or alter the positions of upper and lower ribs." - Gray's Anatomy for Students
3. The Diaphragm (Vertical Dimension)
Inspiratory Action
- Muscular fibers of the diaphragm contract, pulling the central tendon inferiorly
- The domes flatten - this expands the thoracic cavity caudally
- The abdominal contents are pushed downward
- The deeper the inspiration, the flatter the costodiaphragmatic recess becomes, allowing the inferior border of the lung to expand into this supplementary space
Expiratory Action
- The diaphragm relaxes, and elastic recoil returns it upward
- The domes ascend
Position of the Domes at Quiet Expiration (Clinically Important)
- Right dome: at the level of rib V (pushed higher by the liver)
- Left dome: at the fifth intercostal space (slightly lower due to the stomach and spleen)

Diaphragm Openings (Clinically Relevant Structures Passing Through)
| Opening | Vertebral Level | Structures |
|---|---|---|
| Aortic hiatus | T12 | Aorta, thoracic duct, (sometimes azygos vein) |
| Esophageal hiatus | T10 | Esophagus, anterior and posterior vagal trunks, esophageal branches of left gastric vessels |
| Caval opening | T8 | Inferior vena cava, right phrenic nerve |
Innervation
4. Respiratory Muscles
Muscles of Inspiration
- Diaphragm - most important; contraction pushes abdominal contents down and lifts ribs upward and outward
- External intercostal muscles - elevate the ribs, aid in inspiration
- Sternocleidomastoid
- Scalene muscles (anterior, middle, posterior)
- Pectoralis major/minor
Muscles of Expiration
- Internal intercostal muscles - depress ribs downward and inward
- Abdominal muscles (especially transversus abdominis) - compress the abdominal cavity, push the diaphragm upward, and increase intra-abdominal pressure
5. Pressure Changes During Breathing
| Phase | Intrapleural Pressure | Alveolar Pressure | Airflow |
|---|---|---|---|
| FRC (rest) | -5 cm H₂O | 0 (atmospheric) | None |
| Inspiration | More negative (-8 cm H₂O) | Slightly negative | Air flows in |
| End-inspiration | -8 cm H₂O | 0 | None |
| Expiration | Returns to -5 cm H₂O | Slightly positive | Air flows out |
6. Clinical Correlations
Diaphragmatic Paralysis (Phrenic Nerve Palsy)
- Unilateral paralysis: often asymptomatic, or mild exertional dyspnea
- Bilateral paralysis: rare but causes significant respiratory compromise
Diaphragmatic Hernia
Paradoxical Breathing
Referred Pain from the Diaphragm
- Subphrenic abscess (right shoulder tip pain)
- Hemoperitoneum (e.g., ruptured ectopic pregnancy, splenic rupture)
- Ruptured spleen (left shoulder tip - Kehr's sign)
Intercostal Nerve Block
Clinical Assessment of Breathing Pattern
- Abdominal breathing (normal in males and children): diaphragm dominates
- Thoracic breathing (normal in females): intercostal muscles more prominent
- Paradoxical breathing: sign of respiratory failure or phrenic nerve palsy
- Accessory muscle use: sign of increased work of breathing (COPD, asthma, upper airway obstruction)
Summary Table: Muscles, Movements, and Dimensions
| Structure | Movement | Thoracic Dimension Changed |
|---|---|---|
| Diaphragm | Descends on contraction | Vertical (height) |
| External intercostals + upper ribs | Pump handle elevation | Anteroposterior |
| External intercostals + lower ribs | Bucket handle elevation | Lateral (transverse) |
| Internal intercostals | Rib depression (forced expiration) | Reduces AP + lateral |
| Abdominal muscles | Push diaphragm up | Reduces vertical |
| Scalenes / SCM | Fix/elevate upper ribs (accessory) | AP + lateral |
- Gray's Anatomy for Students (9780323934237) - Movements of the thoracic wall and diaphragm during breathing, Diaphragm innervation and openings
- Color Atlas of Human Anatomy Vol. 2 (9783132424487) - Mechanics of Breathing
- Costanzo Physiology 7th Ed. (9780323793339) - Muscles of Inspiration and Expiration
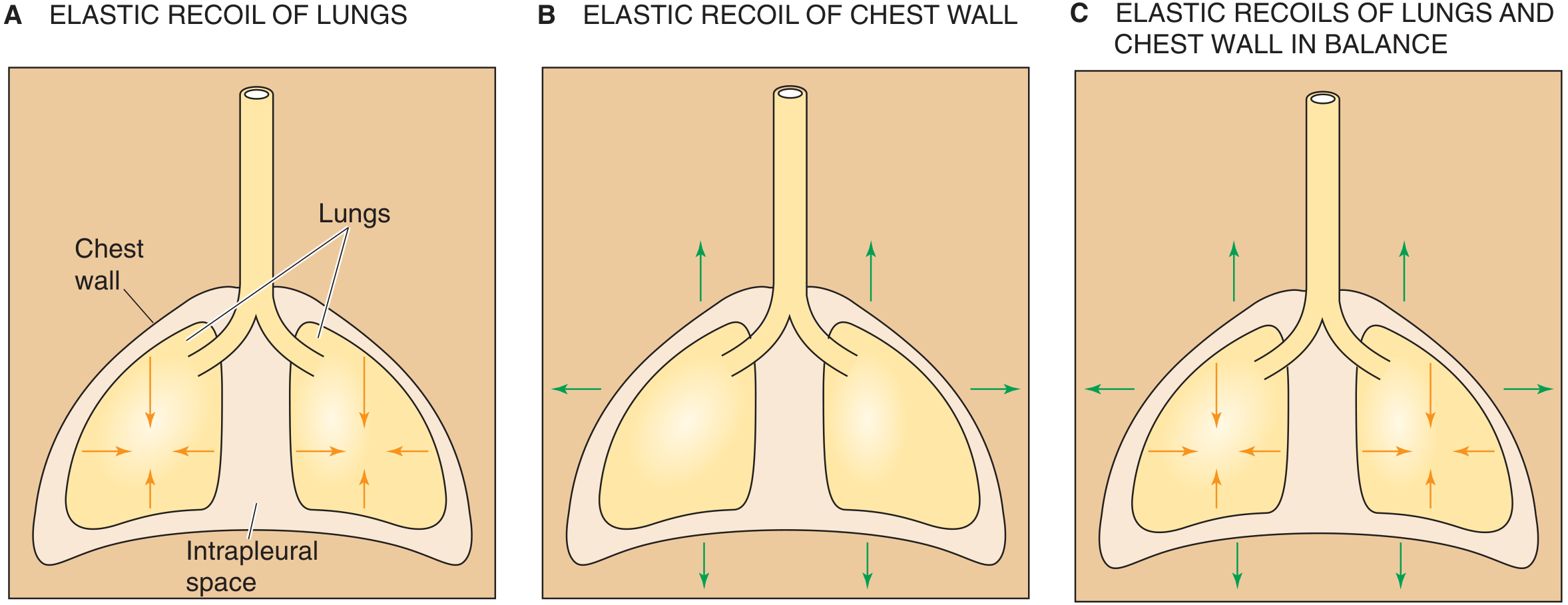
- Medical Physiology (Boron & Boulpaep) (9780323319737) - Opposing elastic recoils, intrapleural pressure
muscle and mechanism easel short brif daw
Clean medical diagram showing muscles and mechanism of respiration. Split into two panels labeled INSPIRATION and EXPIRATION. Show a frontal view of the thorax with: diaphragm (labeled, arrows showing descent during inspiration and ascent during expiration), external intercostal muscles (labeled, arrows showing rib elevation), internal intercostal muscles (labeled), abdominal muscles (labeled). Show thoracic diameter changes with arrows - anteroposterior (pump handle) and lateral (bucket handle). Include small icons for active vs passive process. Accessory muscles listed on side: scalenes, sternocleidomastoid, pectoralis. Clean anatomy illustration style, labeled, educational, white background.
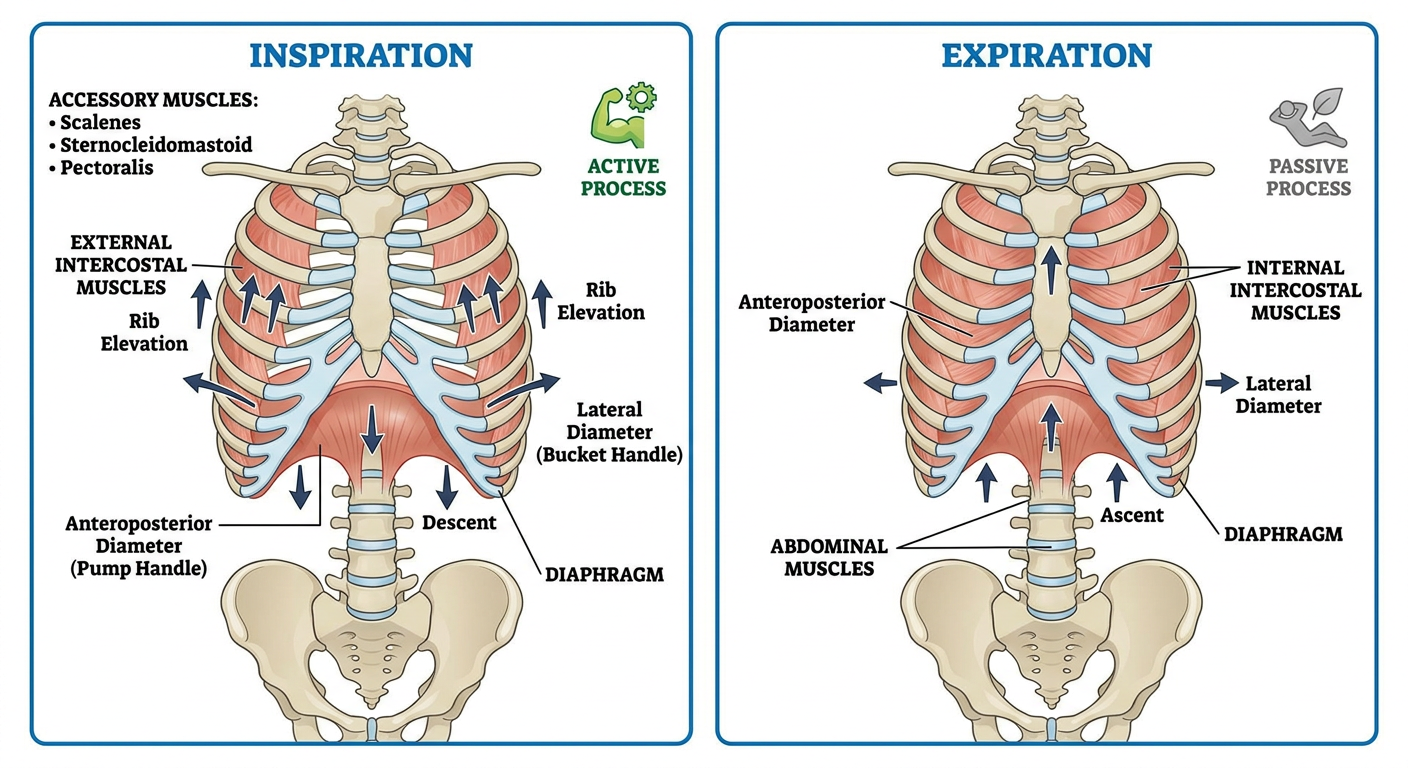
Muscles & Mechanism - Quick Brief
INSPIRATION (Active)
| Muscle | Action | Result |
|---|---|---|
| Diaphragm (primary) | Contracts → descends | ↑ vertical diameter |
| External intercostals | Elevate ribs | ↑ AP + lateral diameter |
| Scalenes (accessory) | Fix/elevate upper ribs | ↑ AP diameter |
| SCM (accessory) | Elevates sternum | ↑ AP diameter |
EXPIRATION (Passive at rest)
| Muscle | Action | Result |
|---|---|---|
| Elastic recoil of lungs + chest wall | No muscle needed | Thorax returns to FRC |
| Internal intercostals (forced only) | Depress ribs | ↓ AP + lateral diameter |
| Abdominal muscles (forced only) | Push diaphragm up | ↓ vertical diameter |
Rib Movement Types
- Pump handle → ribs elevate → sternum moves up & forward → ↑ anteroposterior diameter
- Bucket handle → lateral rib shafts swing outward → ↑ transverse diameter
muscle in inspiration and experimation
Medical education diagram two columns side by side. Left column header "INSPIRATION (Active)" with green color theme, right column header "EXPIRATION (Passive/Forced)" with blue/red color theme. Each column shows an anatomical frontal view of the thorax and lists the muscles with labeled arrows. Left side shows: diaphragm descending (large arrow down), external intercostal muscles with upward rib arrows, scalenes elevating upper ribs, sternocleidomastoid raising sternum, pectoralis minor. Right side shows: diaphragm ascending (passive), internal intercostal muscles depressing ribs, rectus abdominis, external oblique, internal oblique, transversus abdominis pushing diaphragm up. Bottom of each column shows a small summary box: inspiration "volume UP, pressure DOWN, air IN" and expiration "volume DOWN, pressure UP, air OUT". Clean white background, bold labels, medical textbook style.
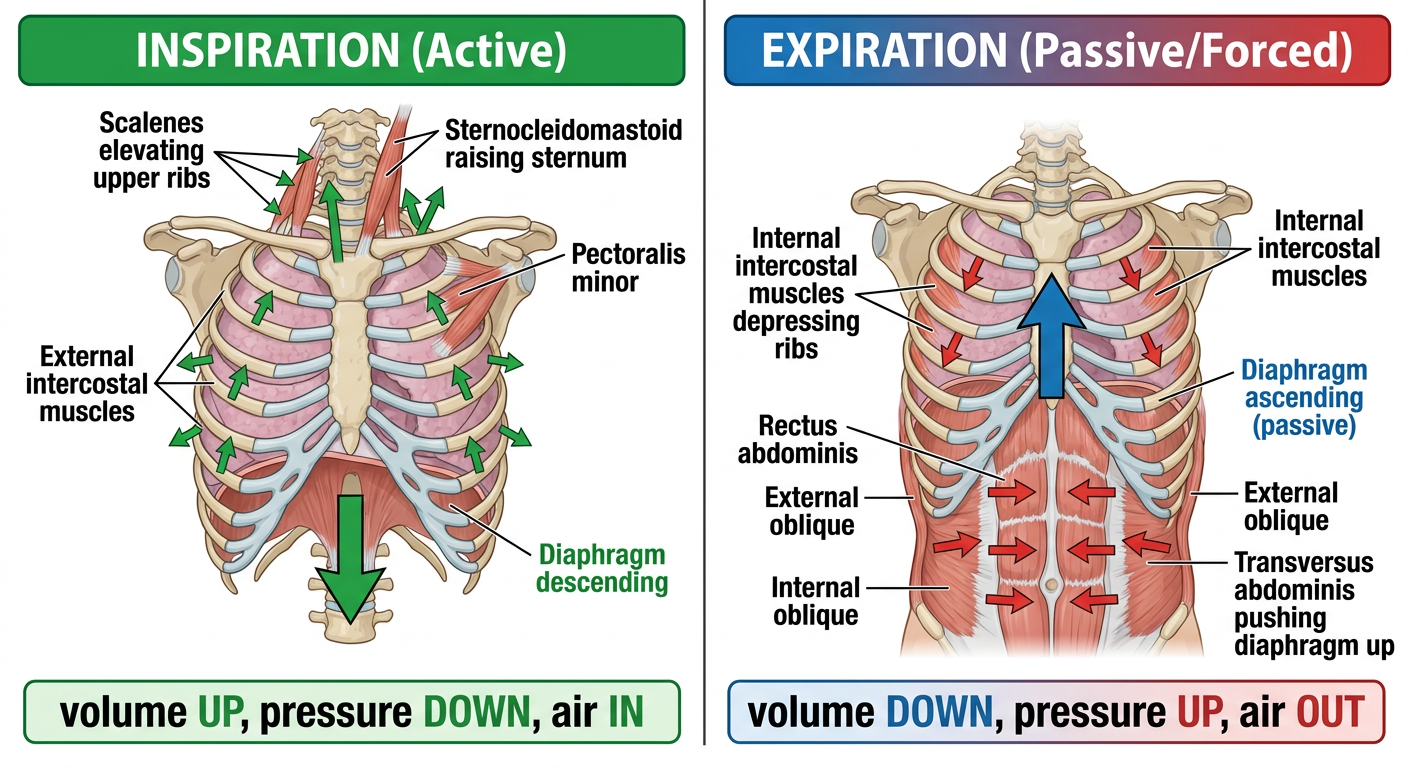
Muscles of Inspiration vs Expiration
INSPIRATION - Active Process
| Muscle | Nerve | Action |
|---|---|---|
| Diaphragm | Phrenic (C3,4,5) | Contracts → descends → ↑ vertical diameter |
| External intercostals | Intercostal nerves | Elevate ribs → ↑ AP + lateral diameter |
| Muscle | Action |
|---|---|
| Scalenes (ant, mid, post) | Fix + elevate upper 2 ribs |
| Sternocleidomastoid (SCM) | Elevates sternum upward |
| Pectoralis minor | Elevates ribs 3-5 (when shoulder fixed) |
| Serratus anterior | Elevates ribs |
EXPIRATION - Passive at Rest / Active When Forced
| Muscle | Action |
|---|---|
| Internal intercostals | Depress ribs → ↓ AP + lateral diameter |
| Rectus abdominis | Compress abdomen → push diaphragm up |
| External oblique | Compress abdomen → push diaphragm up |
| Internal oblique | Compress abdomen → push diaphragm up |
| Transversus abdominis | Most powerful - compresses abdomen |
Memory Summary
INSPIRATION = ACTIVE
Diaphragm (main) + External intercostals
+ Accessory: Scalenes, SCM, Pec minor
EXPIRATION = PASSIVE (quiet) / ACTIVE (forced)
Forced: Internal intercostals + 4 abdominal muscles
Key rule: Diaphragm accounts for 60-70% of all lung volume change during quiet breathing.
External intercostal muscles, erector spinae muscles, scaleni group of muscles, sternocleidomastoid muscles, pectoral muscles, serratus anterior muscles, quadratus lumborum in inspiration.
Detailed medical anatomy diagram showing all accessory muscles of inspiration on a human body anterior and posterior view. Label each muscle with its action during inspiration. Include: External intercostal muscles (between ribs, elevate ribs), Scaleni group - anterior middle posterior scalene (elevate ribs 1 and 2, fix upper chest), Sternocleidomastoid (elevates sternum and clavicle), Pectoral muscles - pectoralis major and minor (elevate ribs when arm fixed), Serratus anterior (elevates ribs, expands chest), Erector spinae group (extend spine, elevate ribs), Quadratus lumborum (fixes 12th rib, stabilizes diaphragm). Show anterior view on left and posterior view on right. Each muscle highlighted in different color with labeled arrows showing direction of action. Clean white background, medical textbook illustration style, bold clear labels.
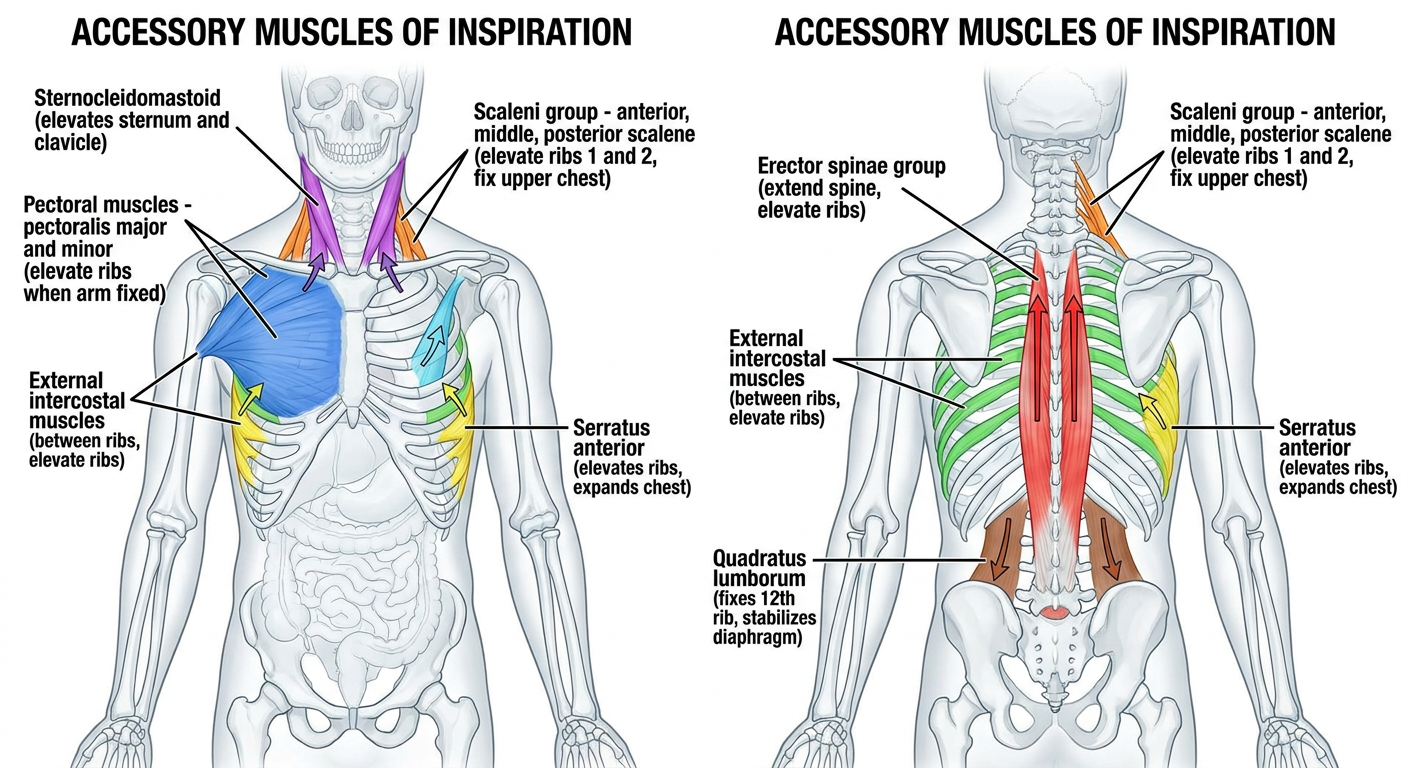
Muscles of Inspiration - Detailed Breakdown
PRIMARY Muscle (always active in quiet breathing)
| Muscle | Nerve Supply | Action in Inspiration |
|---|---|---|
| Diaphragm | Phrenic nerve (C3, C4, C5) | Contracts → descends → ↑ vertical diameter of thorax |
SECONDARY / ACCESSORY Muscles (recruited during deep/forced inspiration, exercise, respiratory distress)
1. External Intercostal Muscles
- Origin: Lower border of rib above
- Insertion: Upper border of rib below
- Nerve: Intercostal nerves (T1-T11)
- Action in inspiration: Elevate the ribs upward and outward → increases anteroposterior and lateral diameters (pump handle + bucket handle)
- Note: Fibers run downward and forward (like hands in pockets)
2. Scaleni Group (Anterior, Middle, Posterior)
- Origin: Transverse processes of cervical vertebrae (C2-C7)
- Insertion: Ant/Mid → 1st rib; Post → 2nd rib
- Nerve: Cervical nerves (C4-C8)
- Action in inspiration:
- Elevate ribs 1 and 2 to expand the upper thorax
- Prevent inward collapse of the upper ribs during diaphragm contraction
- Active even in quiet breathing - they stabilize the upper chest wall
- Clinical note: Hypertrophy visible in COPD patients ("barrel chest")
3. Sternocleidomastoid (SCM)
- Origin: Manubrium sterni + medial clavicle
- Insertion: Mastoid process + superior nuchal line
- Nerve: Accessory nerve (CN XI) + C2, C3
- Action in inspiration: Elevates the sternum and clavicle → lifts the entire anterior chest wall → ↑ AP diameter
- Clinical note: Visible SCM contraction at rest = sign of severe respiratory distress (e.g., acute asthma, COPD exacerbation, upper airway obstruction)
4. Pectoral Muscles (Pectoralis Major + Minor)
- Pectoralis Major
- Origin: Clavicle, sternum, costal cartilages 1-6
- Nerve: Medial + lateral pectoral nerves (C5-T1)
- Action: When arm is fixed (hands on knees / gripping a surface), reverses its action → elevates ribs and sternum → ↑ AP diameter
- Pectoralis Minor
- Origin: Ribs 3, 4, 5
- Insertion: Coracoid process
- Nerve: Medial pectoral nerve (C8, T1)
- Action: When shoulder is fixed, elevates ribs 3-5 upward
- Clinical note: Patients in respiratory distress instinctively lean forward on their arms ("tripod position") to fix the shoulder girdle and activate pectorals as inspiratory muscles
5. Serratus Anterior
- Origin: Outer surfaces of ribs 1-8 (digitations)
- Insertion: Costal surface of medial border of scapula
- Nerve: Long thoracic nerve (C5, C6, C7)
- Action in inspiration: When scapula is fixed, pulls ribs upward and outward → elevates and expands the lateral thorax
- Also: Rotates scapula upward - if scapula is held fixed by other muscles, the ribs are raised instead
- Clinical note: Long thoracic nerve palsy → winged scapula → impaired accessory inspiration
6. Erector Spinae (Sacrospinalis Group)
- Includes: Iliocostalis, Longissimus, Spinalis
- Origin: Sacrum, iliac crest, lumbar vertebrae
- Insertion: Ribs, transverse processes, spinous processes
- Nerve: Posterior rami of spinal nerves
- Action in inspiration:
- Extends the thoracic spine → opens up the thoracic cage anteriorly
- Elevates ribs by straightening the thoracic kyphosis → ↑ AP diameter
- Counteracts the tendency of the spine to flex during deep inspiration
- Note: Particularly important during deep breath in - allows the chest to "open up" fully
7. Quadratus Lumborum
- Origin: Iliac crest + iliolumbar ligament
- Insertion: 12th rib + transverse processes of L1-L4
- Nerve: Subcostal nerve (T12) + lumbar plexus (L1-L3)
- Action in inspiration:
- Fixes and stabilizes the 12th rib from below
- This gives the diaphragm a firm lower attachment point to pull against
- Without QL fixation, the 12th rib would be pulled upward by the diaphragm, reducing its mechanical efficiency
- Analogy: Acts as an anchor for the diaphragm - like staking down a tent
- Clinical note: Paralysis of QL (L1-L2 lesion) → paradoxical elevation of 12th rib during inspiration → reduced diaphragmatic efficiency
Summary Table
| Muscle | Role | When Active |
|---|---|---|
| External intercostals | Elevate ribs (AP + lateral ↑) | Quiet + deep inspiration |
| Scaleni | Elevate ribs 1-2, stabilize upper chest | Even in quiet breathing |
| SCM | Elevate sternum + clavicle | Deep / forced inspiration, distress |
| Pectoralis major/minor | Elevate chest wall (arm/shoulder fixed) | Deep inspiration, distress (tripod) |
| Serratus anterior | Elevate lateral ribs (scapula fixed) | Deep inspiration |
| Erector spinae | Extend spine → open thorax | Deep inspiration |
| Quadratus lumborum | Fix 12th rib → anchor for diaphragm | All inspiration |
Key clinical point: Visible use of SCM and scalenes at rest = accessory muscle recruitment - a sign the patient is working hard to breathe. The tripod position (leaning forward on hands) maximizes pectoral and serratus contribution.
Description of mechanism of respiration mention the diameter of a's the centers, axis throat and masses, pump handle and the bucket handle movement.
Medical anatomy diagram showing the mechanism of rib movement during respiration. Three separate labeled sections: Section 1 top left - "THREE DIAMETERS OF THORAX" showing a frontal view of chest with three arrows labeled: Vertical (up-down, diaphragm), Anteroposterior (front-back, pump handle), Transverse/Lateral (side-side, bucket handle). Section 2 bottom left - "PUMP HANDLE MOVEMENT" lateral/sagittal view of ribs and sternum showing axis of rotation running through costovertebral joint and sternocostal joint (horizontal axis), with arrow showing sternum moving superiorly and anteriorly, labeled "increases AP diameter", upper ribs 1-6. Section 3 right - "BUCKET HANDLE MOVEMENT" anterior view showing axis of rotation running through neck of rib (oblique axis front to back), middle of rib shaft swinging outward and upward laterally like a bucket handle, labeled "increases transverse diameter", lower ribs 7-10. Include small inset showing the two joint axes with dotted lines. Clean white background, color coded, bold labels, medical textbook style.
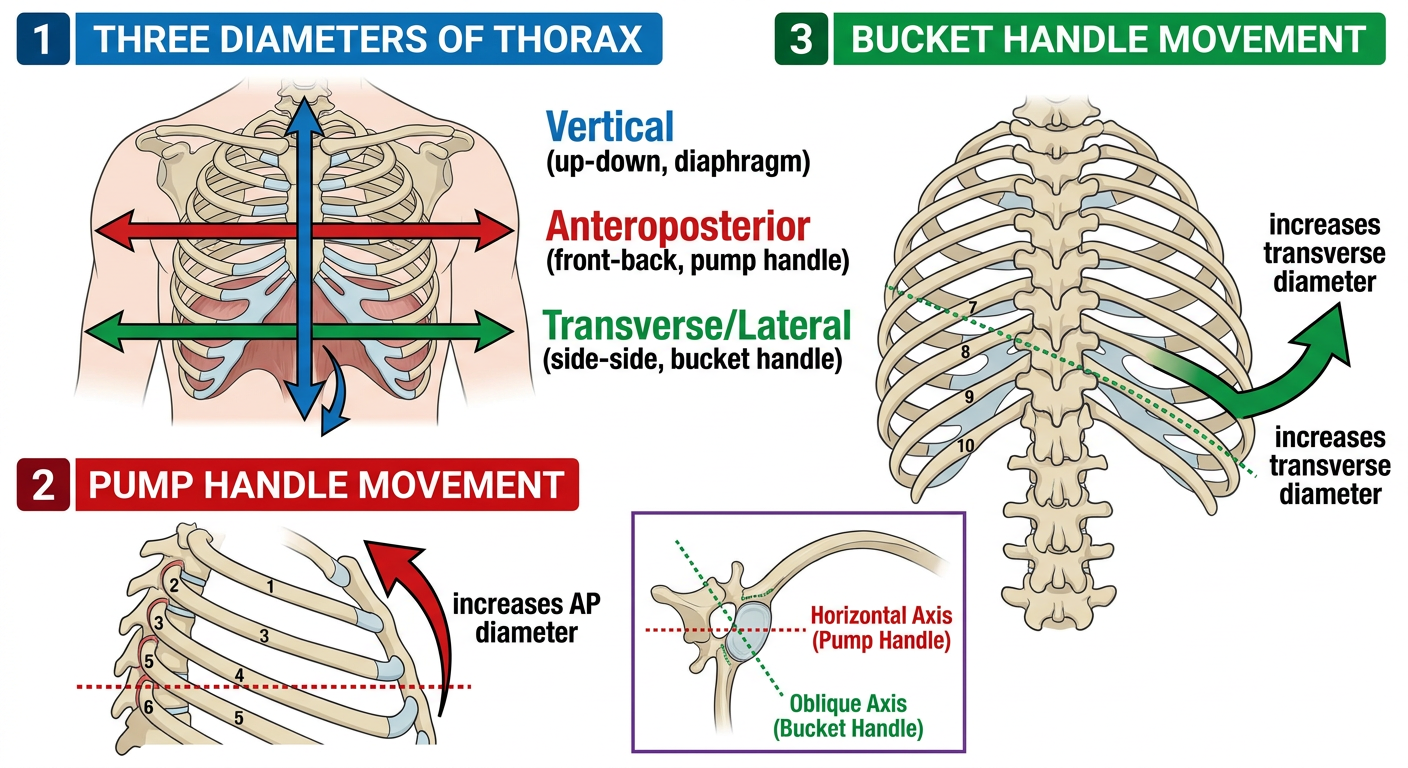
Mechanism of Respiration - Full Description
The Three Diameters of the Thorax
| Diameter | Direction | Mechanism | Normal Range of Change |
|---|---|---|---|
| Vertical | Top to bottom | Diaphragm descends | ~1.5 - 7 cm |
| Anteroposterior (AP) | Front to back | Pump handle movement | Sternum moves ~1.5 cm forward |
| Transverse (Lateral) | Side to side | Bucket handle movement | Ribs swing outward |
The Joints (Centers / Axes of Rotation)
Joints Involved
| Joint | Location | Type |
|---|---|---|
| Costovertebral joint | Head of rib + body of vertebra | Synovial, plane joint |
| Costotransverse joint | Tubercle of rib + transverse process of vertebra | Synovial, plane joint |
| Sternocostal (costochondral) joint | Anterior end of rib + sternum | Fibrocartilaginous (or synovial for 1st) |
The axis of rotation passes through the costovertebral joint posteriorly and the sternocostal joint anteriorly - a line connecting these two points is the hinge on which the rib rotates.
Pump Handle Movement
Anatomy
- Applies mainly to upper ribs (1-6)
- The anterior end of the rib lies lower than the posterior end
- The axis of rotation runs roughly transversely (side to side) through the costovertebral and sternocostal joints
Movement
- When the rib rotates around this transverse axis:
- The anterior end (sternum) moves upward and forward
- The sternum swings like the handle of an old water pump
- Result: Increases the anteroposterior (AP) diameter of the thorax
Analogy
Like the handle of a water pump - it hinges at the back (costovertebral joint) and the front swings upward.
Muscles Responsible
- External intercostals (upper fibers)
- Scaleni (fix ribs 1 and 2 as the upper pivot)
- SCM (lifts the sternum directly)
Bucket Handle Movement
Anatomy
- Applies mainly to lower ribs (7-10)
- The middle of the rib shaft lies lower than both ends
- The axis of rotation runs in an anteroposterior direction (front to back) through the neck of the rib
Movement
- When the rib rotates around this AP axis:
- The lateral part of the shaft swings outward and upward
- Like the handle of a bucket being lifted sideways
- Result: Increases the transverse (lateral) diameter of the thorax
Analogy
Like lifting the handle of a bucket - the midpoint of the handle rises outward to the side.
Muscles Responsible
- External intercostals (lower fibers)
- Diaphragm (pulls the lower ribs outward - zone of apposition effect)
Vertical Diameter - Diaphragm
- The diaphragm is the sole driver of vertical diameter change
- At rest (quiet expiration): Right dome at rib V, Left dome at 5th intercostal space
- During inspiration: Central tendon descends 1.5 to 7 cm depending on depth
- The costodiaphragmatic recess fills as the lungs expand downward into it
Complete Summary - The Mechanism Step by Step
INSPIRATION:
1. Diaphragm contracts
→ descends 1.5-7 cm
→ VERTICAL diameter ↑
2. Upper ribs rotate on TRANSVERSE axis (costovertebral + sternocostal joints)
→ sternum moves UP and FORWARD (pump handle)
→ ANTEROPOSTERIOR diameter ↑
3. Lower ribs rotate on ANTEROPOSTERIOR axis (neck of rib)
→ lateral rib shafts swing OUTWARD (bucket handle)
→ TRANSVERSE (LATERAL) diameter ↑
4. All three together → thoracic VOLUME ↑
→ Intrapleural pressure ↓ (becomes more negative)
→ Alveolar pressure < Atmospheric pressure
→ Air flows INTO the lungs
EXPIRATION (quiet):
→ Elastic recoil of lungs + chest wall
→ All movements reverse passively
→ Volume ↓ → air flows OUT
Quick Reference: Which Ribs, Which Movement
| Rib Group | Predominant Movement | Axis | Diameter Changed |
|---|---|---|---|
| Ribs 1-2 | Pump handle (small) | Transverse | AP |
| Ribs 3-6 | Pump handle (main) | Transverse | AP |
| Ribs 7-10 | Bucket handle (main) | Anteroposterior (oblique) | Transverse |
| Ribs 11-12 (floating) | Caliper movement | Multiple | Posterior expansion |
| All ribs | Combined | Both axes | AP + Transverse |
3 ta diameter e movment axis muscle joints daw
Clean detailed medical education diagram showing all three thoracic diameter changes during respiration, divided into three clear vertical sections on white background. SECTION 1 - LEFT: "VERTICAL DIAMETER" - Frontal view of thorax showing diaphragm - Large downward arrow labeled "Diaphragm descends 1.5-7 cm" - Joint label: "No joint - muscle contraction only" - Axis label: "No bony axis" - Muscle label: "Diaphragm (Phrenic nerve C3,C4,C5)" - Result box: "Vertical diameter INCREASES" - Show diaphragm domes at expiration (dotted line, rib V right, 5th ICS left) vs inspiration (solid line, lower) SECTION 2 - MIDDLE: "ANTEROPOSTERIOR DIAMETER - PUMP HANDLE" - Lateral/sagittal view of ribs and sternum - Dotted line showing AXIS OF ROTATION passing through costovertebral joint (posterior) and sternocostal joint (anterior) - TRANSVERSE horizontal axis - Large curved arrow showing sternum swinging UP and FORWARD - Labels: "Axis: Transverse - through costovertebral + sternocostal joints" "Joints: Costovertebral + Costotransverse + Sternocostal" "Ribs: Upper ribs 1-6" "Muscles: External intercostals, Scaleni, SCM" - Result box: "AP diameter INCREASES" - Small pump handle icon beside it SECTION 3 - RIGHT: "TRANSVERSE DIAMETER - BUCKET HANDLE" - Anterior/coronal view of lower ribs from front - Dotted line showing AXIS OF ROTATION running front-to-back (anteroposterior axis) through neck of rib - Large curved arrows showing lateral rib shafts swinging OUTWARD on both sides - Labels: "Axis: Anteroposterior - through neck of rib" "Joints: Costovertebral + Costotransverse" "Ribs: Lower ribs 7-10" "Muscles: External intercostals (lower), Diaphragm" - Result box: "Transverse diameter INCREASES" - Small bucket handle icon beside it Bottom row: summary table with 3 columns matching above sections. Style: clean, color-coded (blue for vertical, green for AP, orange for transverse), bold black labels, medical textbook quality, white background.
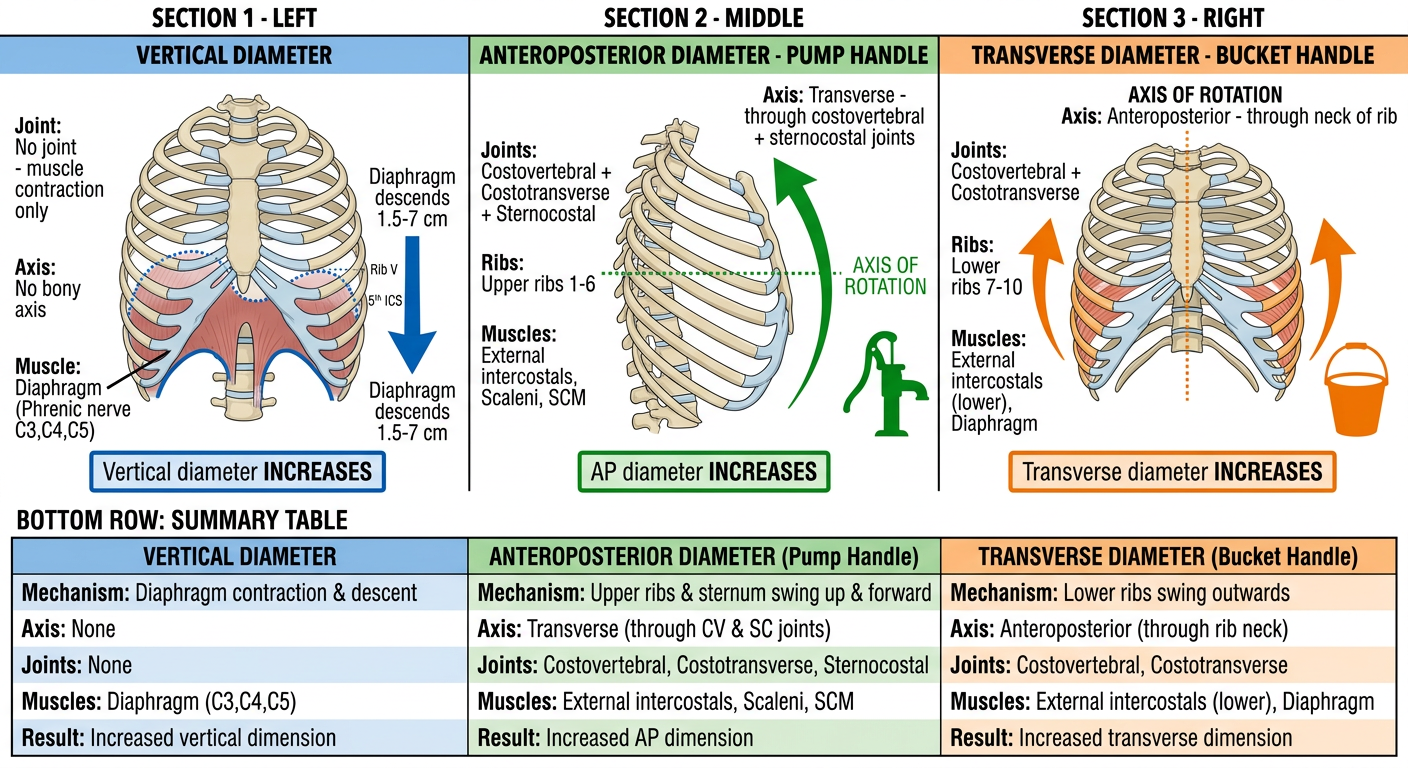
3 Diameters - Quick Reference Table
| VERTICAL | ANTEROPOSTERIOR | TRANSVERSE | |
|---|---|---|---|
| Movement | Diaphragm descends 1.5-7 cm | Sternum moves UP + FORWARD | Lateral rib shafts swing OUTWARD |
| Name | - | Pump Handle | Bucket Handle |
| Axis | No bony axis | Transverse axis (side to side) | Anteroposterior axis (front to back) |
| Joints | - | Costovertebral + Costotransverse + Sternocostal | Costovertebral + Costotransverse |
| Ribs involved | All (via diaphragm) | Upper ribs 1-6 | Lower ribs 7-10 |
| Muscles | Diaphragm (C3,4,5) | Ext. intercostals, Scaleni, SCM | Ext. intercostals (lower), Diaphragm |
| Result | ↑ Height of thorax | ↑ AP diameter | ↑ Lateral diameter |