I am madical student in gujarati university
Welcome! It's great to meet a medical student from Gujarat University.
How can I help you today? Whether it's:
- Anatomy, Physiology, Biochemistry (preclinical subjects)
- Pathology, Pharmacology, Microbiology (para-clinical)
- Medicine, Surgery, Obstetrics (clinical subjects)
- Exam prep, case discussions, MCQs
Just ask your question and I'll do my best to help! 😊
histology of bone
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have comprehensive content and images. Let me compile a thorough answer.
Histology of Bone
Source: Junqueira's Basic Histology, 17e & Histology: A Text and Atlas (Ross & Pawlina)
1. Overview
Bone is a specialized connective tissue composed of cells embedded in a hard, mineralized extracellular matrix (ECM). It differs from other connective tissues because its matrix is calcified - approximately 70% inorganic (mainly hydroxyapatite crystals: Ca₁₀(PO₄)₆(OH)₂) and 30% organic (mainly type I collagen + proteoglycans + glycoproteins).
2. Types of Bone
Macroscopic Types
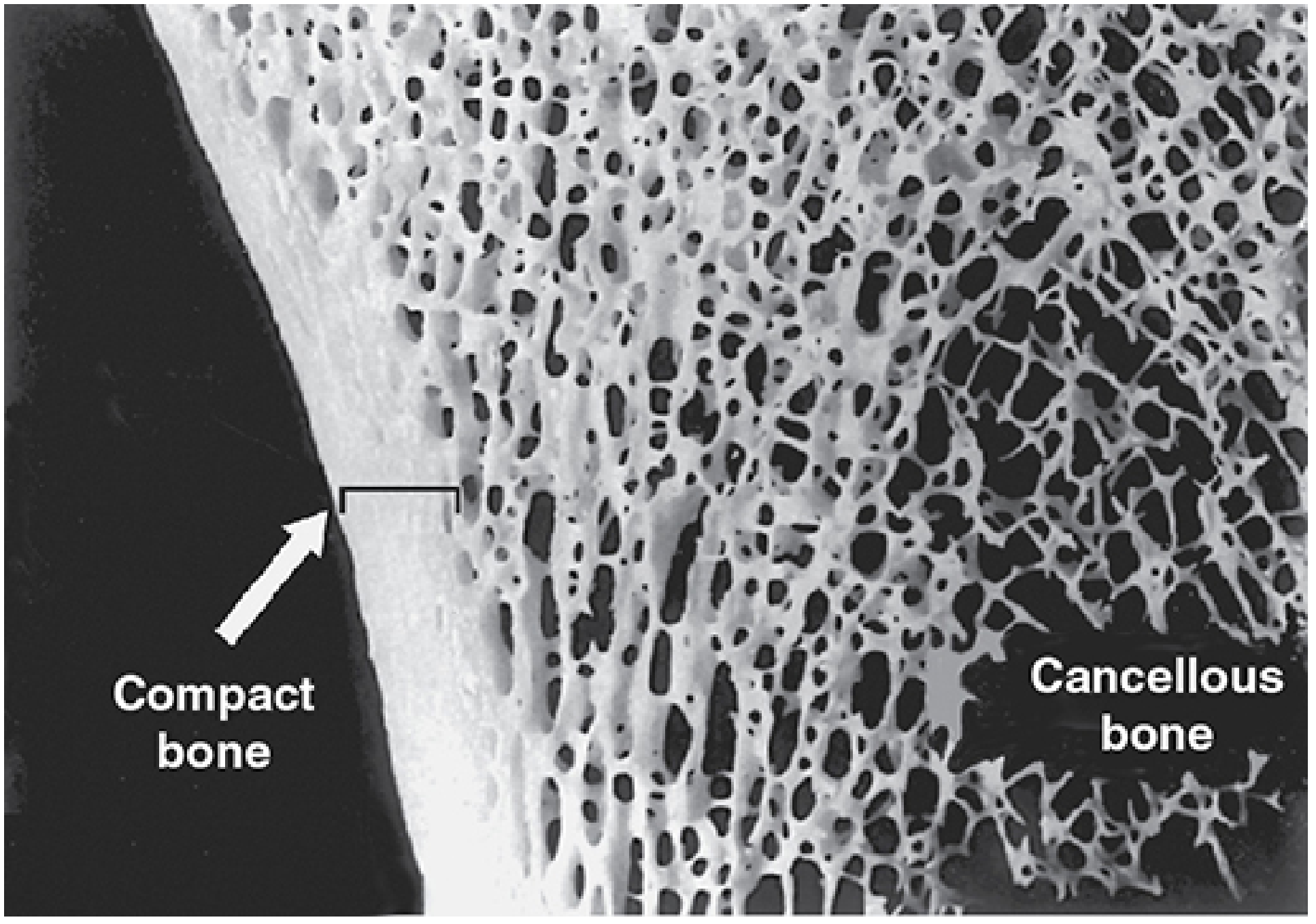
| Type | Also Called | % of Total | Location | Structure |
|---|---|---|---|---|
| Compact bone | Cortical bone | ~80% | Outer region (diaphysis of long bones) | Dense, parallel lamellae / osteons |
| Cancellous bone | Spongy / trabecular bone | ~20% | Inner region (epiphyses), around marrow cavities | Interconnected trabeculae / spicules covered by endosteum |
Microscopic Types
| Type | Features | Found In |
|---|---|---|
| Woven (primary) bone | Irregular, random collagen arrangement; lightly calcified; rapidly formed | Fetal bone, fracture callus |
| Lamellar (secondary) bone | Ordered parallel collagen in lamellae 3-7 μm thick; heavily calcified | All adult normal bone |
Key exam point: Woven bone is replaced by lamellar bone during remodeling. Under polarized light, lamellar bone shows alternating bright and dark bands due to the orthogonal shift in collagen fiber orientation between successive lamellae - this is birefringence.
3. Bone Cells
A. Osteoprogenitor Cells
- Origin: mesenchymal stem cells (periosteum and endosteum)
- Flat, spindle-shaped cells with pale-staining nuclei
- Can proliferate and differentiate into osteoblasts
- Found in inner cellular layer of periosteum and in endosteum
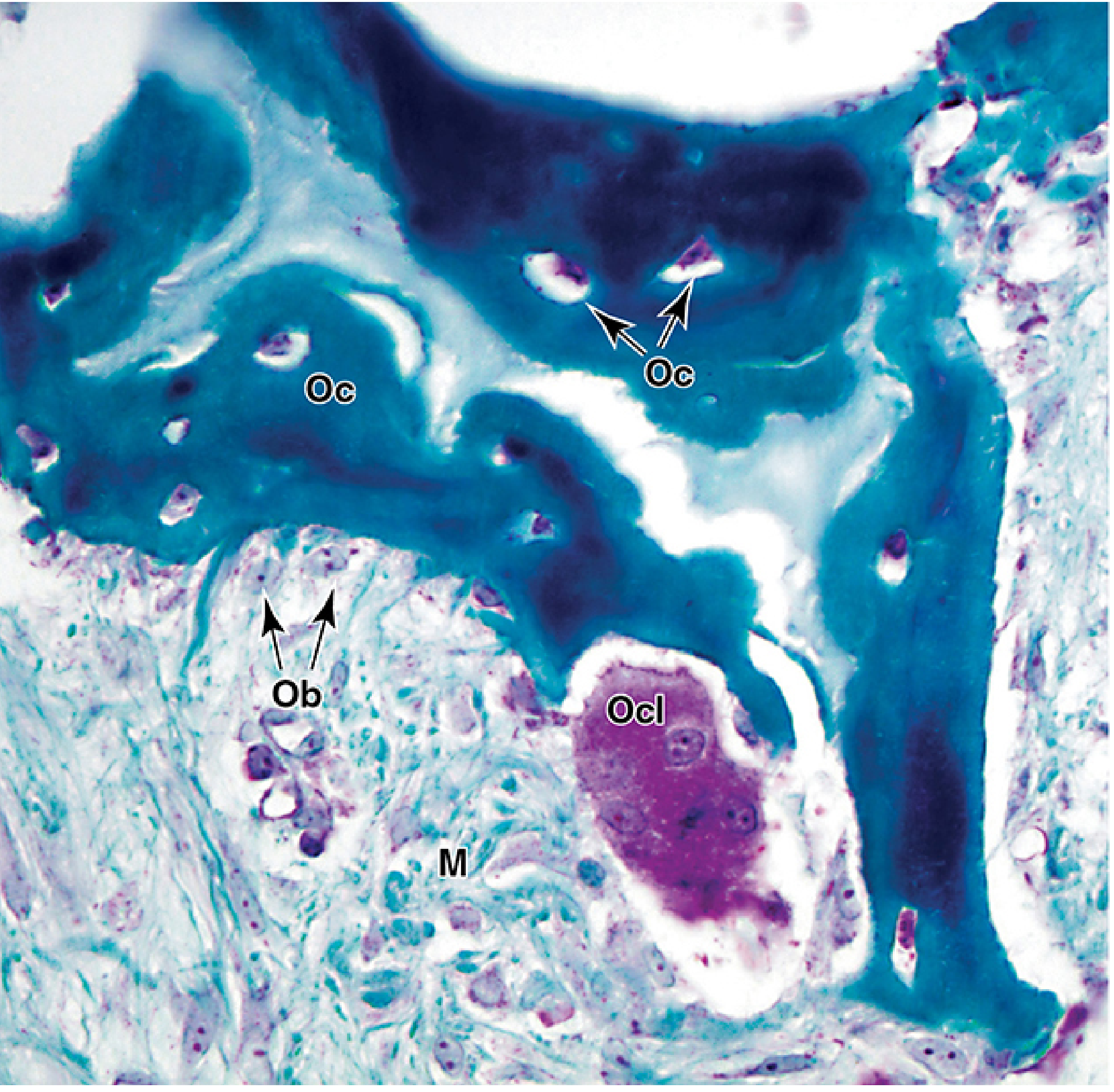
B. Osteoblasts (Ob)
- Bone-forming cells
- Single layer of cuboidal cells on bone surfaces
- Basophilic cytoplasm (rich in RER) - actively synthesize osteoid
- Secrete: type I collagen, proteoglycans, osteonectin, osteocalcin
- Alkaline phosphatase activity - essential for mineralization
- Joined by gap junctions and adherent junctions
- Fate: become osteocytes (trapped in matrix), bone lining cells, or undergo apoptosis
C. Osteocytes (Oc)
- Most numerous bone cell
- Former osteoblasts trapped in lacunae within calcified matrix
- Flattened cell body with long dendritic processes in canaliculi
- Processes connect to adjacent osteocytes and to central canal via gap junctions
- Maintain bone matrix; act as mechanosensors
- Cannot divide; metabolites exchanged via canalicular network
D. Osteoclasts (Ocl)
- Bone-resorbing cells
- Very large, multinucleated (up to 50 nuclei) - formed by fusion of blood monocytes
- Located in shallow resorption pits = Howship's lacunae
- Ruffled border (brush border) - greatly increases surface area for resorption
- Secrete: HCl (dissolves mineral) + cathepsin K (degrades collagen)
- Sealing zone - ring of tight contact between osteoclast and bone
- Acidophilic (eosinophilic) cytoplasm
| Cell | Origin | Function | Key Feature |
|---|---|---|---|
| Osteoprogenitor | Mesenchyme | Stem cell | Flat, pale |
| Osteoblast | Mesenchyme | Forms bone (osteoid) | Cuboidal, basophilic, on surface |
| Osteocyte | Osteoblast | Maintains matrix, mechanosensor | In lacunae + canaliculi |
| Osteoclast | Blood monocyte | Resorbs bone | Multinuclear, ruffled border, Howship's lacuna |
4. Bone Matrix
Organic Component (30%)
- Type I collagen (90% of organic matrix) - provides tensile strength
- Non-collagenous proteins: osteonectin (binds collagen to mineral), osteocalcin, osteopontin, proteoglycans, bone morphogenetic proteins (BMPs)
- The unmineralized organic matrix is called osteoid
Inorganic Component (70%)
- Mainly hydroxyapatite [Ca₁₀(PO₄)₆(OH)₂]
- Also carbonate, citrate, fluoride, magnesium
- Provides compressive strength and hardness
5. The Osteon (Haversian System) - Structural Unit of Compact Bone
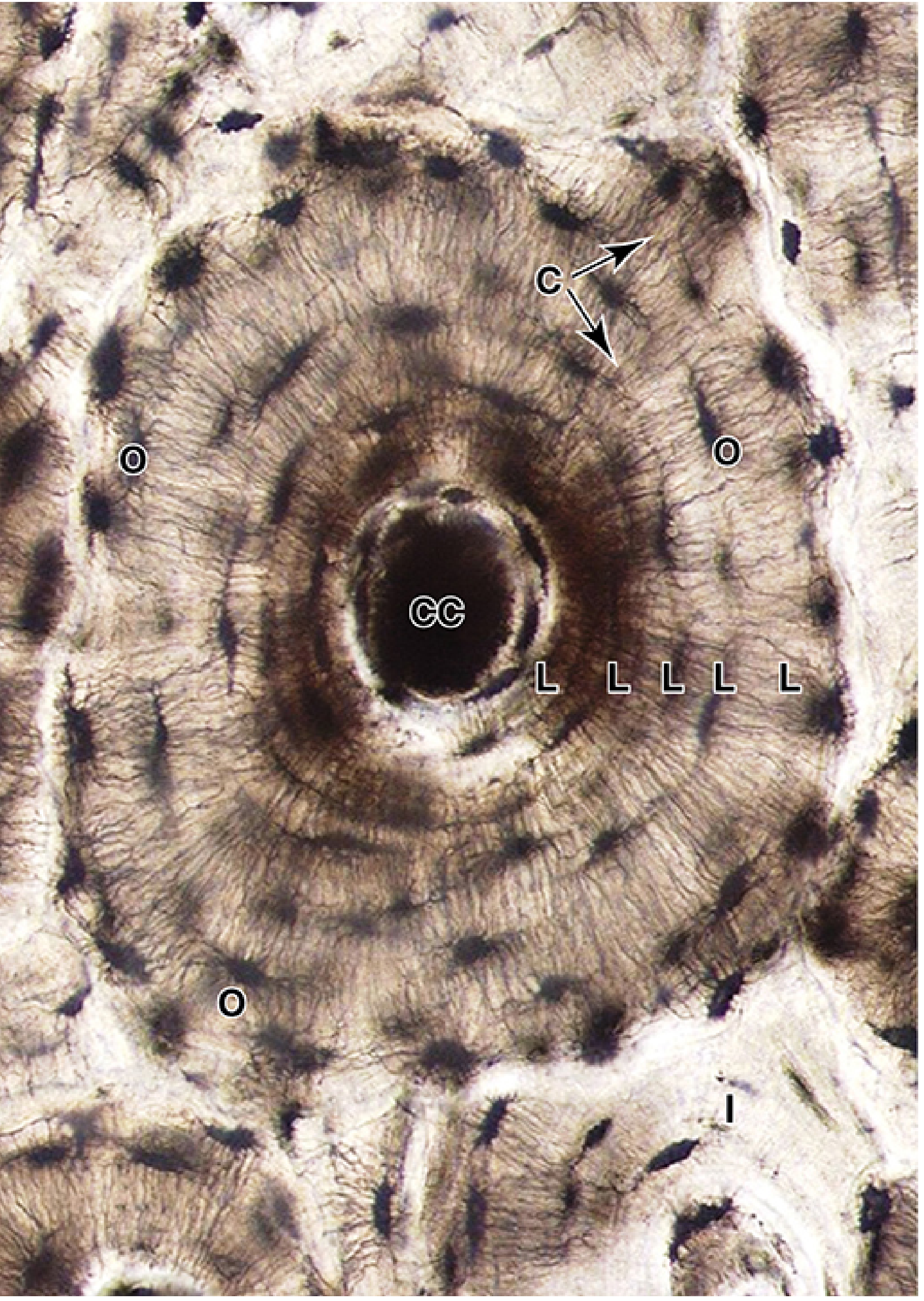
The osteon is 100-250 μm in diameter and consists of:
| Component | Description |
|---|---|
| Haversian canal (central canal) | Contains blood vessels, nerves, loose connective tissue, endosteum |
| Concentric lamellae | 4-20 rings of calcified matrix surrounding the canal |
| Lacunae | Small spaces between lamellae, each housing one osteocyte |
| Canaliculi | Tiny channels radiating from lacunae, containing cell processes |
| Cement line | Outer boundary of osteon; rich in non-collagen proteins, poor in collagen |
| Interstitial lamellae | Remnants of old, remodeled osteons between current osteons |
Canal System
- Haversian canals - run longitudinally (parallel to long axis of bone)
- Volkmann's (perforating) canals - run perpendicular/oblique, connect Haversian canals to each other and to the periosteum and marrow
6. Periosteum and Endosteum
Periosteum (outer covering)
- Outer fibrous layer: dense connective tissue, fibroblasts, blood vessels
- Inner cellular (cambium) layer: osteoprogenitor cells, osteoblasts, bone lining cells
- Sharpey's (perforating) fibers - collagen bundles anchoring periosteum into bone matrix
Endosteum (inner covering)
- Lines marrow cavities and covers trabeculae of cancellous bone
- Thin layer of osteoprogenitor cells and bone lining cells
- Covers surfaces of all haversian and Volkmann canals
7. Bone Formation (Ossification)
A. Intramembranous Ossification
- Direct from mesenchyme - no cartilage template
- Forms: flat bones of skull, clavicle, mandible
- Mesenchymal cells → osteoprogenitor cells → osteoblasts → deposit osteoid → calcification
- Forms woven bone first, then remodeled to lamellar bone
B. Endochondral Ossification
- Uses hyaline cartilage model as template
- Forms: long bones, short bones, base of skull, vertebrae, ribs
- Zones of epiphyseal growth plate (from epiphysis toward diaphysis):
- Zone of reserve (resting) cartilage - no proliferation
- Zone of proliferating cartilage - chondrocytes dividing (coin-stack columns)
- Zone of hypertrophic cartilage - cells enlarge, matrix calcifies
- Zone of calcified cartilage - chondrocytes die (apoptosis), cartilage calcifies
- Zone of ossification (bone deposition) - osteoblasts deposit bone on calcified cartilage spicules
8. Histological Preparation Note
Bone cannot be sectioned routinely because of its hardness. Two methods are used:
- Decalcification - immerse in acid or EDTA to remove mineral, then paraffin-embed and section
- Ground sections - bone is ground down to thin slices without decalcification (used to study Haversian systems)
Quick Summary for Exams
| Feature | Compact Bone | Cancellous Bone |
|---|---|---|
| % of bone mass | 80% | 20% |
| Structure | Osteons (Haversian systems) | Trabeculae / spicules |
| Surface covering | Periosteum outside | Endosteum on all surfaces |
| Location | Diaphysis of long bones | Epiphyses, around marrow |
Key associations to remember:
- Osteoblast = Basophilic cytoplasm (lots of RER)
- Osteoclast = Multinucleated, ruffled border, Howship's lacuna
- Osteocyte = Lacuna + canaliculi
- Haversian canal = longitudinal; Volkmann canal = transverse/oblique
- Bone mineral = hydroxyapatite
- Junqueira's Basic Histology, 17e, pp. 353-370
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology (Ross & Pawlina)
action potentials in nerve fibres
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
Loading Image
I now have all the images and content needed. Let me compile the complete, exam-ready answer.
Action Potentials in Nerve Fibres
Source: Guyton and Hall Textbook of Medical Physiology & Neuroscience: Exploring the Brain, 5e
1. Resting Membrane Potential
Before discussing action potentials, the resting state must be understood:
- Resting membrane potential (RMP) = -70 mV (inside negative relative to outside)
- Maintained by: Na⁺-K⁺ ATPase pump (pumps 3 Na⁺ out, 2 K⁺ in), K⁺ leak channels, and ionic concentration gradients
- K⁺ is more concentrated inside the cell; Na⁺ is more concentrated outside
- The membrane is said to be "polarized" at rest
2. What is an Action Potential?
An action potential (AP) is a rapid, self-propagating, all-or-none change in membrane potential that travels along the nerve fibre. It is the electrical signal by which nerve impulses are transmitted.
Key property: All-or-None Law - once threshold is reached, the AP fires at full amplitude regardless of stimulus strength. Stimulus strength is encoded by frequency of APs, not their size.
3. Phases of the Action Potential
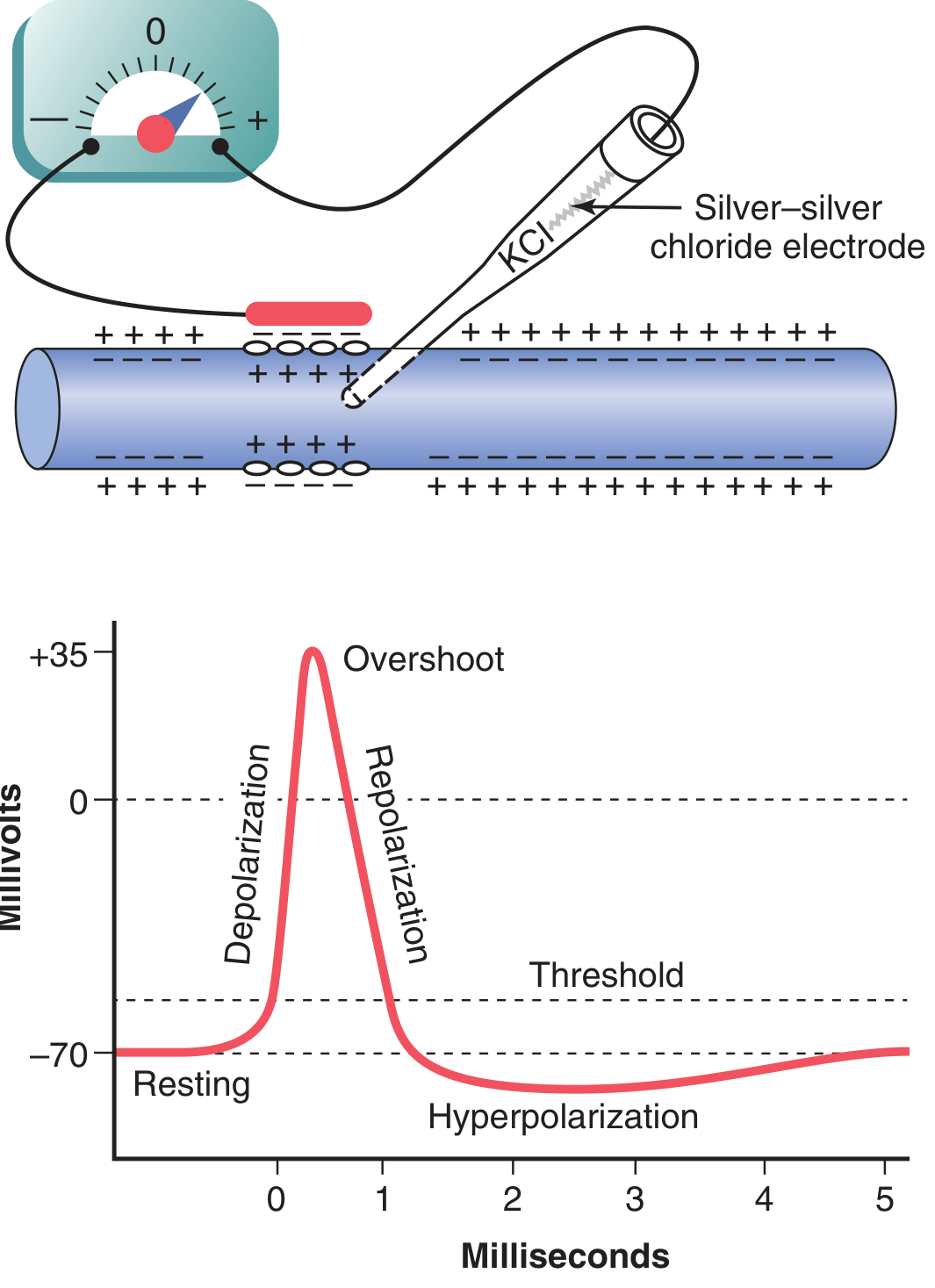
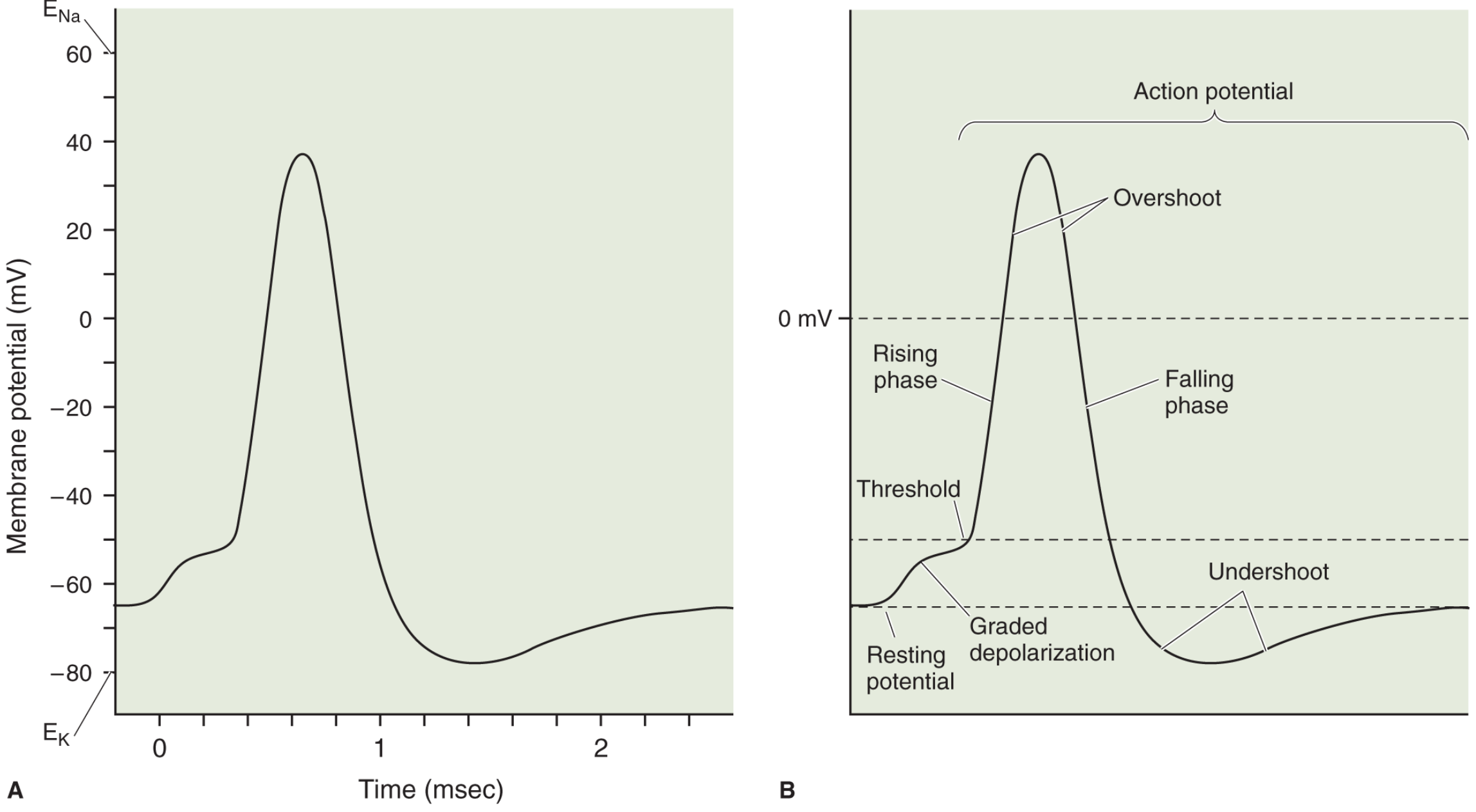
Phase-by-Phase Breakdown
| Phase | mV Range | Ion Movement | Channel Event |
|---|---|---|---|
| Resting | -70 mV | None | Na⁺ channels closed; K⁺ leak channels open |
| Graded depolarization | -70 → -55 mV | Small Na⁺ inflow | Stimulus brings membrane toward threshold |
| Threshold | ~-55 mV | - | Critical point - AP becomes inevitable |
| Rising phase (depolarization) | -55 → +35 mV | Rapid Na⁺ influx | Voltage-gated Na⁺ channels open (activation gate opens) |
| Overshoot | ~+35 mV peak | Na⁺ influx at peak | Vm approaches E_Na (+60 mV) but doesn't reach it |
| Falling phase (repolarization) | +35 → -70 mV | K⁺ efflux | Na⁺ channels inactivate (inactivation gate closes); K⁺ channels open |
| Undershoot (after-hyperpolarization) | Below -70 mV | Excess K⁺ efflux | K⁺ channels remain open too long |
| Restoration | back to -70 mV | Na⁺-K⁺ pump restores gradients | K⁺ channels close; Na⁺-K⁺ ATPase active |
Total duration: ~2 milliseconds
4. Voltage-Gated Ion Channels (The Molecular Basis)
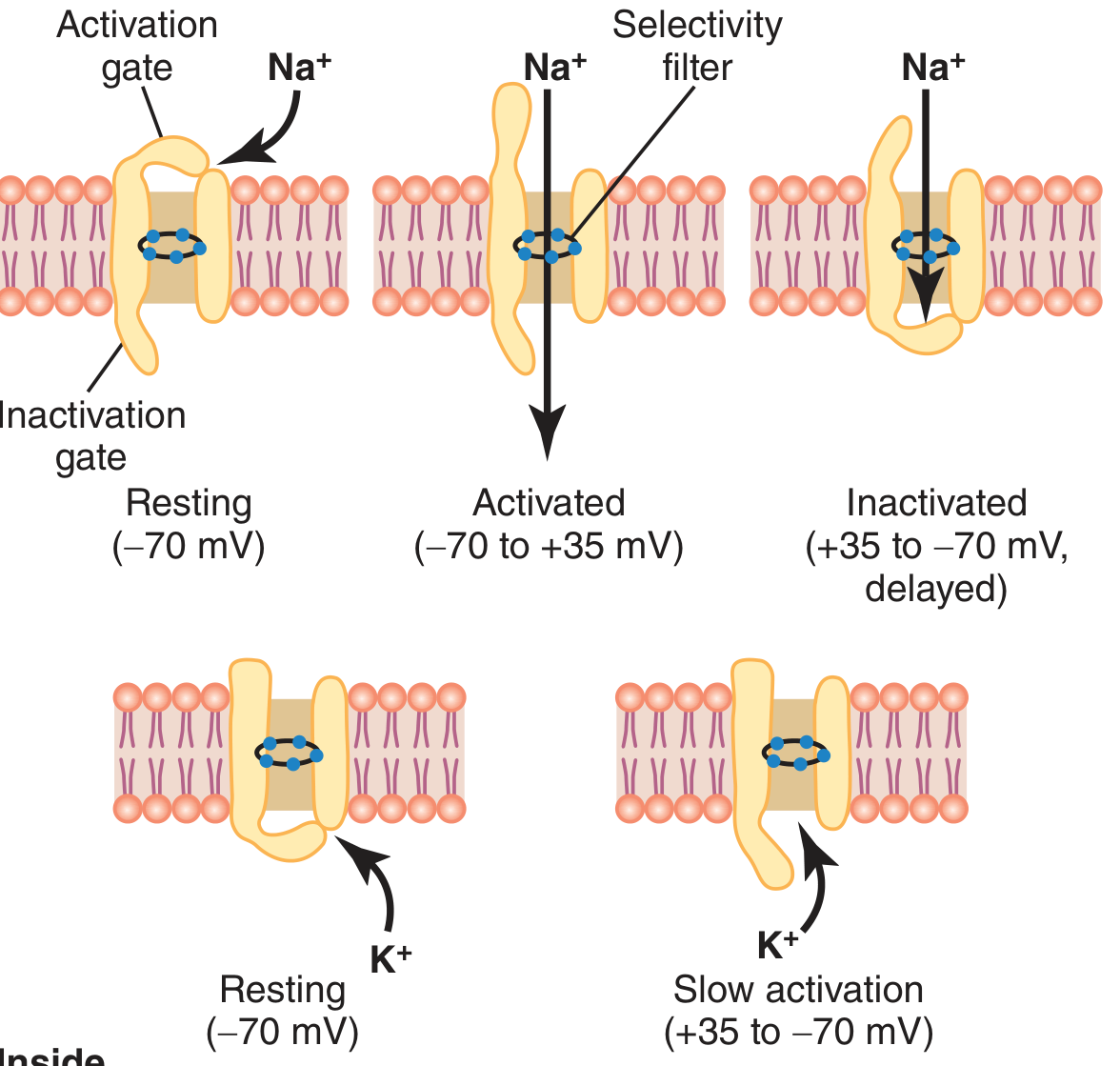
Voltage-Gated Na⁺ Channel - THREE STATES
The Na⁺ channel has two gates:
- Activation gate (outer) - opens rapidly with depolarization
- Inactivation gate (inner) - closes slowly after activation
| State | Membrane Potential | Activation Gate | Inactivation Gate | Na⁺ Flow |
|---|---|---|---|---|
| Resting (closed) | -70 mV | Closed | Open | None |
| Activated (open) | -55 to +35 mV | Open | Open | Inward (rapid) |
| Inactivated | Returning to -70 mV | Open | Closed | None |
Key point: The channel cannot re-open from the inactivated state until the membrane repolarizes back to near resting potential. This is the basis of the absolute refractory period.
When depolarization occurs, permeability to Na⁺ increases 500-5000 fold.
Voltage-Gated K⁺ Channel - TWO STATES
- Has only one gate (activation gate)
- Opens more slowly than Na⁺ channels (delayed rectifier)
- Opens during repolarization phase (after Na⁺ channels inactivate)
- Stays open a little too long → causes after-hyperpolarization (undershoot)
- No inactivation gate - simply closes slowly as membrane repolarizes
Positive Feedback (Hodgkin Cycle)
Depolarization → Na⁺ channels open → Na⁺ rushes in → more depolarization → more Na⁺ channels open...
This explosive positive feedback explains the all-or-none, spike-like nature of the AP.
5. Refractory Periods
| Period | Duration | Mechanism | Can AP be fired? |
|---|---|---|---|
| Absolute Refractory Period (ARP) | ~1 ms (during AP + early repolarization) | Na⁺ channels are inactivated - cannot open regardless of stimulus strength | No |
| Relative Refractory Period (RRP) | ~1-2 ms after ARP | Na⁺ channels recovering; K⁺ channels still partially open (membrane hyperpolarized) | Yes, but needs supramaximal stimulus |
Significance: Refractory periods ensure:
- APs travel in one direction only (forward, never backward)
- APs are discrete, separated signals
- Limits maximum firing frequency (~500-1000 Hz)
6. Propagation of the Action Potential
Unmyelinated fibres (continuous conduction)
- Na⁺ influx at active site creates local currents that depolarize adjacent membrane
- This brings adjacent membrane to threshold → AP propagates forward
- Cannot go backward because that region is in the refractory period
- Like a burning fuse - the flame moves forward, can't go back because the material behind it is spent
Myelinated fibres (saltatory conduction)
- Myelin sheath insulates the axon between nodes of Ranvier
- AP can only be generated at nodes (where ion channels are concentrated)
- Electrical current "jumps" from one node to the next - saltatory conduction (Latin: saltare = to jump)
- Much faster and more energy-efficient than continuous conduction
| Feature | Unmyelinated | Myelinated |
|---|---|---|
| Conduction velocity | 0.5-2 m/s | Up to 120 m/s |
| Type of conduction | Continuous | Saltatory |
| Energy cost | Higher | Lower |
| Example | C fibres (pain, temperature) | Aα fibres (motor, proprioception) |
7. Nerve Fibre Classification
| Fibre Type | Myelin | Diameter | Velocity | Function |
|---|---|---|---|---|
| Aα | Thick | 12-20 μm | 70-120 m/s | Skeletal muscle motor, proprioception |
| Aβ | Medium | 5-12 μm | 30-70 m/s | Touch, pressure |
| Aγ | Thin | 3-6 μm | 15-30 m/s | Muscle spindle (intrafusal) |
| Aδ | Thin | 2-5 μm | 5-30 m/s | Fast pain, cold temperature |
| B | Thin | <3 μm | 3-15 m/s | Preganglionic autonomic |
| C | None | 0.2-1.5 μm | 0.5-2 m/s | Slow pain, warmth, postganglionic autonomic |
8. Factors Affecting Conduction Velocity
- Myelin - increases velocity dramatically (saltatory conduction)
- Axon diameter - larger diameter = faster conduction (less resistance)
- Temperature - higher temperature = faster conduction (cold slows or blocks conduction - used in cryoanesthesia)
9. Role of the Na⁺-K⁺ ATPase Pump
- Works continuously in the background to restore ionic gradients
- Pumps 3 Na⁺ out and 2 K⁺ in per cycle (electrogenic - contributes ~-4 mV)
- A single AP barely changes ionic gradients - 100,000 to 50 million APs can fire before gradients run down significantly
- Activity increases ~8-fold when intracellular Na⁺ doubles (concentration-sensitive)
- Requires ATP - explains why neurons are highly sensitive to ischemia/hypoxia
10. Clinical Relevance
| Clinical Condition | Mechanism |
|---|---|
| Local anesthetics (lidocaine) | Block voltage-gated Na⁺ channels → prevent AP generation |
| Tetrodotoxin (TTX) | Blocks Na⁺ channel activation gate from outside |
| Multiple sclerosis | Demyelination slows/blocks saltatory conduction |
| Hypocalcemia | Ca²⁺ normally stabilizes Na⁺ channel gating; low Ca²⁺ → hyperexcitability, tetany |
| Hyperkalemia | Reduces RMP (less negative) → partial inactivation of Na⁺ channels → weakness/paralysis |
Quick Exam Summary
- RMP: -70 mV (Guyton) / -65 mV (Neuroscience texts)
- Threshold: ~-55 mV (about 15 mV above RMP)
- Peak overshoot: ~+35 mV
- Duration: ~2 ms
- Depolarization: Na⁺ in (via voltage-gated Na⁺ channels)
- Repolarization: K⁺ out (via voltage-gated K⁺ channels)
- Na⁺ channel has 3 states: Resting → Activated → Inactivated
- ARP: Na⁺ channels inactivated → no AP possible
- RRP: Partial recovery → suprathreshold stimulus needed
- Saltatory conduction: Jumps between nodes of Ranvier → fast + efficient
- Guyton and Hall Textbook of Medical Physiology, 14e, pp. 79-90
- Neuroscience: Exploring the Brain, 5e, Chapter 4
This is a shared conversation. Sign in to Orris to start your own chat.