Brachial plexus
Reading File
Finding Sources
Searching the Web
brachial plexus anatomy roots trunks divisions cords branches
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content to deliver a thorough answer. Let me compile everything.
Brachial Plexus
The brachial plexus is a somatic nerve network formed by the anterior rami of C5, C6, C7, C8, and most of T1. It originates in the neck, passes laterally and inferiorly over rib I, and enters the axilla, where it supplies the entire upper limb (motor and sensory).
- Gray's Anatomy for Students, p. 858
Anatomical Organization: Roots → Trunks → Divisions → Cords → Branches
The plexus is classically organized from medial to lateral in five levels: Roads To Drink Cold Beer (Roots, Trunks, Divisions, Cords, Branches).
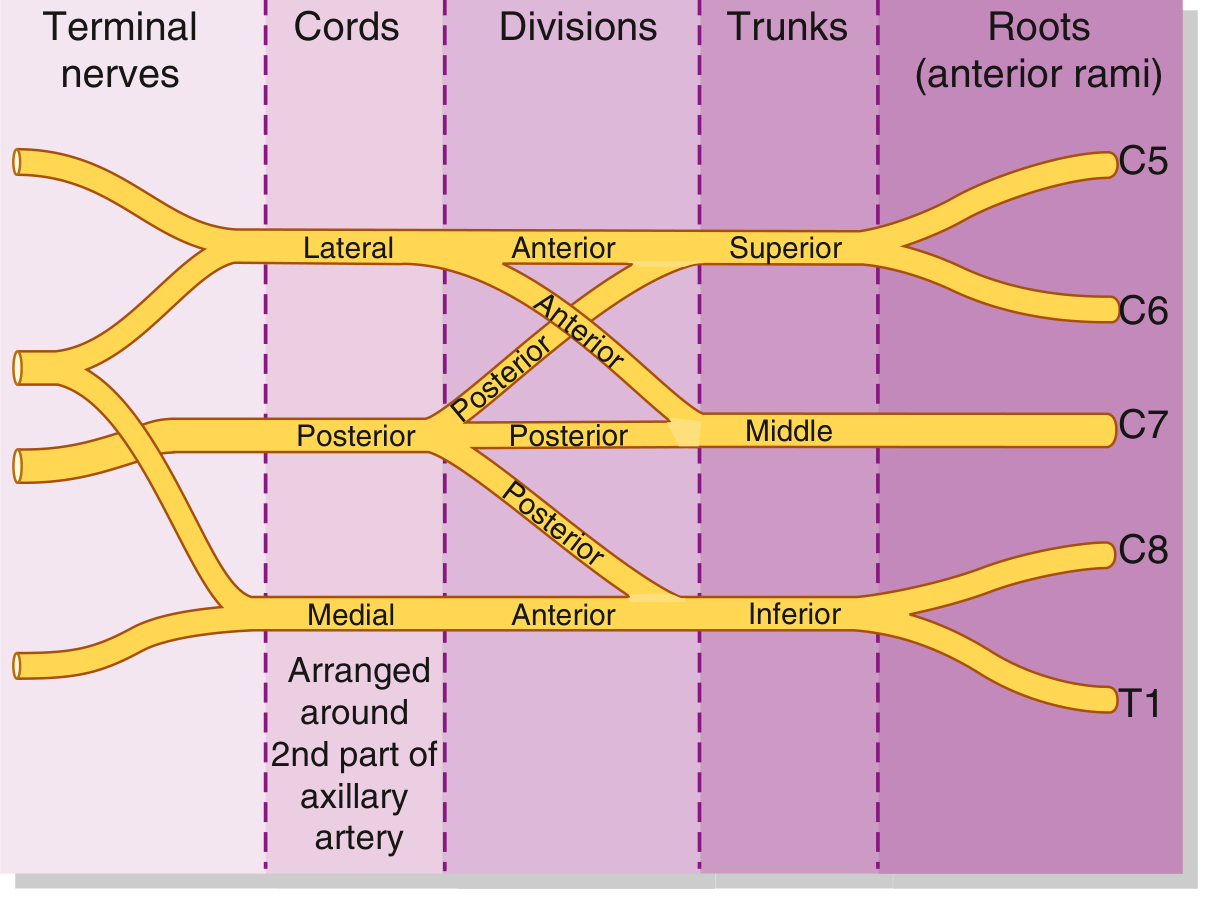
Fig. 7.52B - Schematic of brachial plexus organization (Gray's Anatomy for Students)

Fig. 7.52A - Major components of the brachial plexus in the neck and axilla
1. Roots (Anterior Rami)
The five roots (C5-T1) emerge between the anterior and middle scalene muscles and receive gray rami communicantes from the sympathetic trunk (postganglionic sympathetic fibers).
- C5 gives a contribution to the phrenic nerve
Branches from the roots:
| Nerve | Root(s) | Supplies |
|---|---|---|
| Dorsal scapular | C5 | Rhomboid major, rhomboid minor (and levator scapulae) |
| Long thoracic | C5, C6, C7 | Serratus anterior |
2. Trunks
The roots combine to form three trunks, which cross the posterior triangle of the neck and pass over rib I:
| Trunk | Formed by |
|---|---|
| Superior (upper) | C5 + C6 |
| Middle | C7 alone |
| Inferior (lower) | C8 + T1 |
The inferior trunk lies on rib I posterior to the subclavian artery.
Branches from trunks (from the superior trunk only):
- Suprascapular nerve (C5, C6) - passes through the suprascapular foramen; innervates supraspinatus and infraspinatus
- Nerve to subclavius (C5, C6) - innervates the subclavius muscle
No branches arise from the middle or inferior trunks.
3. Divisions
Each trunk splits into an anterior and a posterior division as the plexus passes behind the clavicle. This reorganizes fibers destined for anterior vs. posterior compartments:
- Anterior divisions → supply flexor (anterior) compartments
- Posterior divisions → supply extensor (posterior) compartments
No peripheral nerves originate directly from the divisions.
4. Cords
The divisions recombine to form three cords, named by their position relative to the second part of the axillary artery:
| Cord | Formed from | Root contributions |
|---|---|---|
| Lateral | Anterior divisions of superior + middle trunks | C5, C6, C7 |
| Medial | Anterior division of inferior trunk | C8, T1 |
| Posterior | All three posterior divisions | C5, C6, C7, C8, T1 |
5. Branches (Terminal and Collateral)
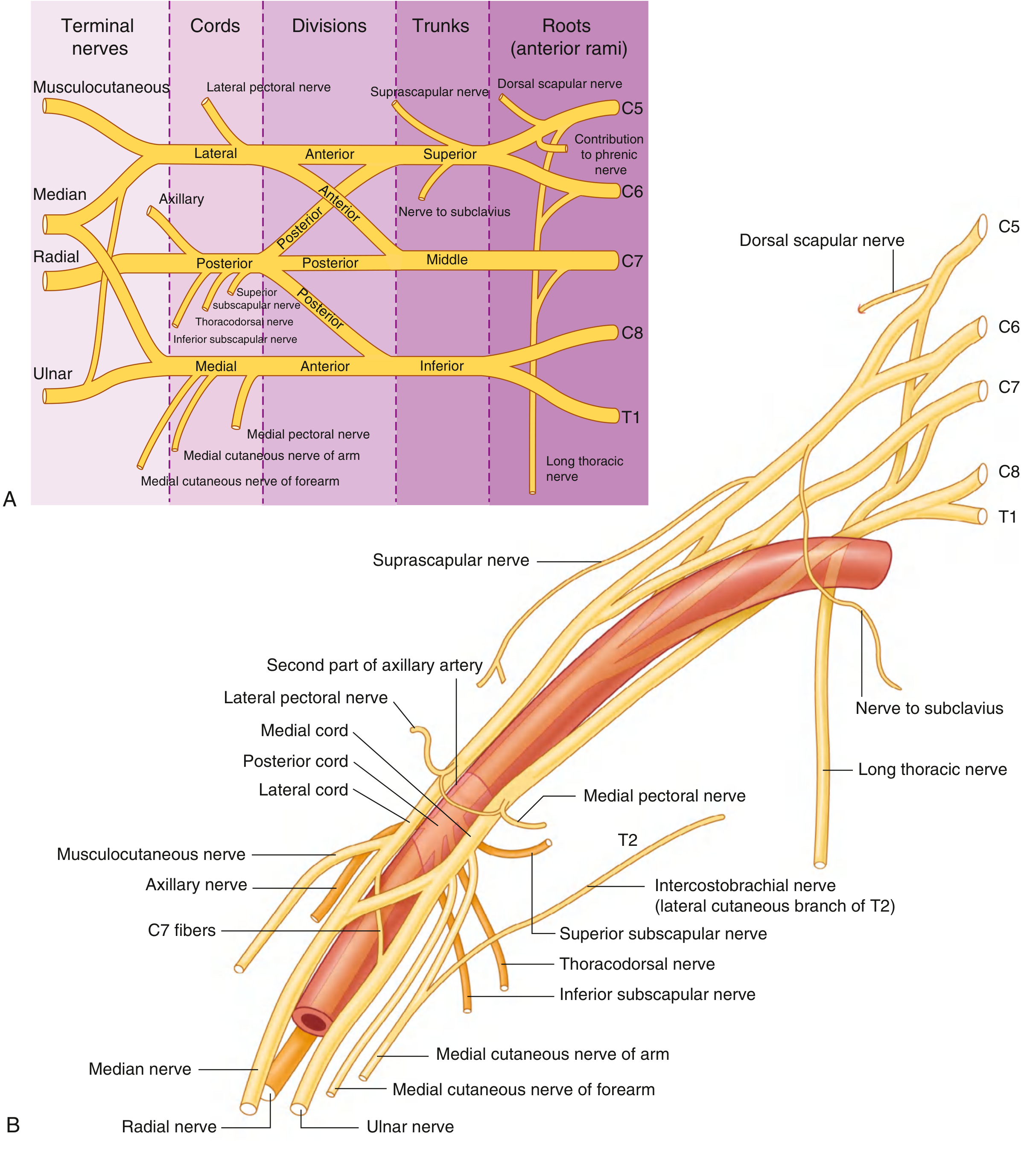
Fig. 7.53 - All branches of the brachial plexus with relationships to axillary artery
From the Lateral Cord (C5-C7):
- Lateral pectoral nerve - pectoralis major (clavicular head)
- Musculocutaneous nerve - all three anterior arm muscles (coracobrachialis, biceps brachii, brachialis); terminates as lateral cutaneous nerve of forearm
- Lateral root of median nerve - joins medial root to form the median nerve
From the Medial Cord (C8-T1):
- Medial pectoral nerve - pectoralis major and minor
- Medial cutaneous nerve of the arm - skin on medial distal arm
- Medial cutaneous nerve of the forearm - skin on medial forearm to wrist
- Medial root of median nerve - joins lateral root
- Ulnar nerve - all intrinsic hand muscles except 3 thenar + 2 lateral lumbricals; flexor carpi ulnaris; medial half flexor digitorum profundus; skin over medial 1.5 fingers
Median nerve (C5-T1):
Formed anterior to the third part of the axillary artery by union of the lateral + medial roots. Innervates most anterior forearm muscles, thenar muscles, lateral two lumbricals, and skin over lateral 3.5 digits (palmar).
From the Posterior Cord (C5-T1):
- Superior subscapular nerve - subscapularis (upper part)
- Thoracodorsal nerve - latissimus dorsi
- Inferior subscapular nerve - subscapularis (lower part) and teres major
- Axillary nerve - exits via quadrangular space; innervates deltoid and teres minor; gives superior lateral cutaneous nerve of arm
- Radial nerve (largest terminal branch) - all posterior compartment muscles of arm and forearm; skin on posterior arm, posterior forearm, dorsolateral hand
A helpful memory aid: the lateral cord forms an "M" shape with the median nerve and medial cord together with the musculocutaneous and ulnar nerves on either side - visible in dissection as the M/W pattern.
Clinical Notes: Brachial Plexus Injuries
Injury level predicts the clinical syndrome:
| Level injured | Mechanism | Syndrome |
|---|---|---|
| Roots | Cervical spinal cord injury, traction | Avulsion (most severe; loss of nerve conduction on NCS) |
| Trunks | Trauma to rib I | Superior/inferior trunk palsies |
| Cords | Glenohumeral dislocation | Cord-specific deficits |
Erb-Duchenne Palsy (Upper Brachial Plexus - C5, C6)
Caused by forcible widening of the angle between the shoulder and neck (motorcycle fall, difficult delivery). Muscles affected: deltoid, biceps, brachialis, brachioradialis, supinator. Classic posture: "policeman's tip" / "waiter's tip" - arm internally rotated, elbow extended, forearm pronated. Sensory loss over lateral arm and upper lateral forearm.
- S. Das, A Manual on Clinical Surgery 13th Ed, p. 140
Klumpke's Palsy (Lower Brachial Plexus - C8, T1)
Caused by forceful abduction/hyperabduction of the arm (e.g., grabbing a rail while falling). Results in paralysis of intrinsic hand muscles - claw hand with combined median + ulnar palsy features. Sensory loss over medial forearm, hand, and medial 1.5 fingers. Often associated with Horner's syndrome (ptosis, miosis, enophthalmos, anhidrosis) due to disruption of T1 sympathetic fibers.
Complete Plexus Palsy
Severe trauma affecting all roots. Anaesthesia of the whole upper limb (except the upper arm - C3/4 territory). Complete paralysis. Assessment involves nerve conduction studies and EMG. Preganglionic (avulsion) injuries carry a much worse prognosis than postganglionic ones and cannot be repaired directly.
- Gray's Anatomy for Students, p. 867
- S. Das, A Manual on Clinical Surgery 13th Ed, p. 140
Summary Table of Key Nerves
| Nerve | Cord/Root | Key muscles | Key sensory | Injury sign |
|---|---|---|---|---|
| Musculocutaneous | Lateral (C5-C7) | Biceps, brachialis, coracobrachialis | Lateral forearm | Weak elbow flexion |
| Median | Lateral + Medial (C5-T1) | Thenar muscles, anterior forearm | Lateral 3.5 digits | Ape hand, "hand of benediction" |
| Ulnar | Medial (C8-T1) | Intrinsic hand muscles | Medial 1.5 digits | Claw hand |
| Radial | Posterior (C5-T1) | All posterior arm + forearm | Dorsolateral hand | Wrist drop |
| Axillary | Posterior (C5-C6) | Deltoid, teres minor | Over deltoid | Weak shoulder abduction |
| Long thoracic | Roots C5-C7 | Serratus anterior | - | Medial winging of scapula |
| Suprascapular | Superior trunk (C5-C6) | Supraspinatus, infraspinatus | - | Weak shoulder abduction/ER |
This is a shared conversation. Sign in to Orris to start your own chat.