Write in detail for MS opthalmology examination preparation about Pathogenesis and genetics of primary open angle glaucoma from kanski in flowchart and easy understandable form with risk factors negative postive history in concern.. in and optic disc changes in flowchart , and pictorial form... Explaining gonioscopy slit lamp fundus perimetry oct tonometry with initial to recent treatment protocol explain treatment nicely..
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Model call limits exceeded: run limit (20/20)
Write notes for above given prompt
Here are comprehensive MS Ophthalmology examination notes on Primary Open-Angle Glaucoma (POAG) based on Kanski's Clinical Ophthalmology (10th edition):
📋 PRIMARY OPEN-ANGLE GLAUCOMA (POAG)
MS Ophthalmology Examination Notes — Based on Kanski's 10th Edition
SECTION 1: DEFINITION
POAG = Chronic, progressive optic neuropathy of adult onset characterized by:
- Retinal nerve fibre layer (RNFL) thinning
- Glaucomatous optic nerve damage
- Characteristic visual field loss
- Open anterior chamber angle
- Absence of secondary glaucoma signs
- IOP is a key modifiable risk factor
SECTION 2: PATHOGENESIS — FLOWCHART
TRIGGER: Elevated IOP / Vascular insufficiency / Genetic predisposition
│
▼
┌─────────────────────────────────────┐
│ MECHANICAL THEORY │
│ IOP compresses axons at │
│ lamina cribrosa │
│ → Axoplasmic flow disruption │
└──────────────┬──────────────────────┘
│ +
┌──────────────▼──────────────────────┐
│ VASCULAR / ISCHAEMIC THEORY │
│ IOP compresses blood vessels │
│ → Optic nerve head ischaemia │
│ → Low ocular perfusion pressure │
└──────────────┬──────────────────────┘
│
▼
RETINAL GANGLION CELL (RGC) INJURY
│
▼
Ca²⁺ influx into RGC cell body
+ ↑ intracellular nitric oxide
+ Glutamine metabolism disruption
│
▼
RGC DEATH via APOPTOSIS
(Programmed cell death — NOT necrosis)
│
▼
Astrocyte + glial cell proliferation
+ Extracellular matrix changes at lamina cribrosa
│
▼
OPTIC NERVE HEAD REMODELLING
│
▼
RNFL THINNING → OPTIC CUP ENLARGEMENT
→ VISUAL FIELD LOSS
Key point for exam: RGC death = APOPTOSIS. Pre-terminal event = Ca²⁺ influx + ↑ nitric oxide.
SECTION 3: GENETICS — FLOWCHART
POAG GENETICS
│
├─── 127+ loci identified in human genome (Nature Communications, 2021)
│
├─── KEY GENES:
│ │
│ ├── MYOC gene → codes for MYOCILIN protein
│ │ (found in trabecular meshwork)
│ │ • Various mutations described
│ │ • Normal function still undetermined
│ │ • If glaucoma onset <35 yrs in a family member
│ │ → chance of MYOC mutation UP TO 33%
│ │
│ └── OPTN gene → codes for OPTINEURIN
│ • Broadly accepted as causing glaucoma
│
├─── INHERITANCE PATTERN:
│ • Siblings: 4× risk
│ • Offspring: 2× risk
│ • Genetic investigation if ≥3 first-degree relatives
│ from 2 generations affected
│
└─── POLYGENIC RISK SCORE (PRS):
• Predicts glaucoma susceptibility
• Predicts risk of advanced disease
• Future: personalised treatment thresholds
SECTION 4: RISK FACTORS
4A. POSITIVE RISK FACTORS (Increase risk)
| Risk Factor | Detail |
|---|---|
| Elevated IOP | Higher IOP = greater glaucoma risk. Asymmetry ≥4 mmHg significant |
| Age | More common in older individuals |
| Race | Black > White (4× more common, earlier onset, harder to control); Asian ~3% in >70 yrs |
| Family history | 1st-degree relative: siblings 4× risk, offspring 2× risk |
| Myopia | Associated with increased incidence; may increase susceptibility to damage |
| Large optic disc | More vulnerable to damage; thinner lamina cribrosa |
| Thin central corneal thickness (CCT) | Falsely low IOP reading; independent risk factor |
| Vascular disease | Hypertension, cardiovascular disease, diabetes, vasospasm (migraine) |
| Low ocular perfusion pressure | ↑ risk of development and progression |
| Translaminar pressure gradient | Difference between IOP and orbital CSF pressure → lamina cribrosa deformation |
| Anti-VEGF therapy | Sustained IOP elevation especially after repeated bevacizumab injections |
| Calcium-channel blockers | Meta-analysis: higher prevalence in users (monotherapy) |
| Oral contraceptive pill | Several years use associated with increased risk |
| Steroids | Topical, inhaled, or systemic — raise IOP |
4B. NEGATIVE / PROTECTIVE FACTORS (Reduce risk or not proven)
| Factor | Comment |
|---|---|
| Diabetes mellitus | Longitudinal studies show NO increased risk. Earlier clinic-based data showing higher prevalence due to selection bias |
| Oral beta-blockers | May LOWER IOP (systemic effect masks elevation) |
| Controlled IOP | Maintaining IOP <18 mmHg prevents progression (AGIS trial) |
4C. HISTORY TAKING — WHAT TO ASK
HISTORY IN POAG
│
├── SYMPTOMS (usually NONE until advanced)
│ └── Peripheral field loss → tubular vision → central loss (late)
│ Occasionally: symptomatic central field defects early in NTG
│
├── OPHTHALMIC HISTORY
│ ├── Refractive error (myopia → POAG risk; hypermetropia → PACG risk)
│ ├── Previous trauma / inflammation
│ └── Prior eye surgery (affects IOP reading)
│
├── FAMILY HISTORY
│ ├── POAG / Ocular hypertension (OHT)
│ └── Other ocular disease
│
├── PAST MEDICAL HISTORY
│ ├── Asthma / heart failure / heart block / peripheral vascular disease
│ │ (contraindications to beta-blockers)
│ ├── Head injury / stroke / intracranial pathology
│ │ (may mimic VF loss)
│ ├── Vasospasm — migraine / Raynaud phenomenon
│ ├── Diabetes, systemic hypertension, cardiovascular disease
│ └── Oral contraceptive use
│
├── CURRENT MEDICATIONS
│ ├── Steroids (topical skin / inhaled / systemic)
│ ├── Oral beta-blockers (lower IOP)
│ └── Anti-VEGF injections
│
├── SOCIAL HISTORY
│ └── Smoking, alcohol (rule out toxic/nutritional optic neuropathy)
│
└── ALLERGIES
└── Sulfonamide allergy → acetazolamide CONTRAINDICATED
SECTION 5: EXAMINATION FINDINGS
5A. SLIT LAMP EXAMINATION
SLIT LAMP — WHAT TO LOOK FOR IN POAG SUSPECT
│
├── ANTERIOR SEGMENT
│ ├── Cornea: rule out pigment (Krukenberg spindle → pigment dispersion)
│ ├── Anterior chamber: depth (shallow → angle closure risk)
│ ├── Iris: transillumination defects (pigment dispersion)
│ │ pseudoexfoliation deposits at pupil margin
│ └── Lens: pseudoexfoliation material on anterior surface
│
├── PUPILS
│ ├── Check for RAPD (relative afferent pupillary defect)
│ └── If RAPD develops later → indicator of substantial progression
│
├── COLOUR VISION
│ └── Ishihara — if colour loss suggests NON-glaucomatous optic neuropathy
│
└── KEY: Exclude SECONDARY glaucoma causes (pigmentary, pseudoexfoliation)
5B. TONOMETRY
IOP MEASUREMENT
│
├── GOLDMANN APPLANATION TONOMETRY (GAT) — Gold Standard
│ ├── Applied to corneal apex
│ ├── Measures force to flatten 3.06mm diameter area
│ └── Normal IOP: 10–21 mmHg (population mean ~15.5 mmHg)
│
├── PACHYMETRY (CCT) — always do before tonometry interpretation
│ ├── Thin CCT (<555μm) → underestimates IOP → higher true risk
│ ├── Thick CCT (>590μm) → overestimates IOP → lower true risk
│ └── Note time of day — diurnal variation up to 5 mmHg
│
├── NON-CONTACT TONOMETRY (air puff) — screening use
│
├── iCARE REBOUND TONOMETRY — no anaesthesia needed
│
└── ASYMMETRY: ≥4 mmHg difference between eyes is significant
PROGRESSION RISK FACTORS FROM EMGT:
(a) Magnitude of initial IOP reduction
(b) Height of baseline IOP
(c) Pseudoexfoliation syndrome
(d) Bilateral disease
(e) Worse mean deviation
(f) Older age
5C. GONIOSCOPY
GONIOSCOPY IN POAG
│
├── PURPOSE: Confirm OPEN angle (rule out angle closure or secondary causes)
│
├── WHAT YOU SEE (Shaffer grading, nasal to cornea):
│ ├── Schwalbe line (SL) — anterior limit
│ ├── Trabecular meshwork (TM) — pigmented band
│ ├── Scleral spur (SS) — white band
│ ├── Ciliary body band (CBB) — grey/brown
│ └── Iris root
│
├── IN POAG:
│ ├── Angle WIDE OPEN — all structures visible
│ ├── TM may show variable pigmentation
│ └── No peripheral anterior synechiae (PAS)
│
├── LENS OPTIONS:
│ ├── Goldmann 3-mirror (indirect — image inverted)
│ └── Zeiss/Sussman 4-mirror (direct — no mirror inversion)
│
└── KEY EXAM POINT:
• POAG = open angle
• Gonioscopy is MANDATORY before diagnosing ANY glaucoma
• Angle must be open in ALL quadrants
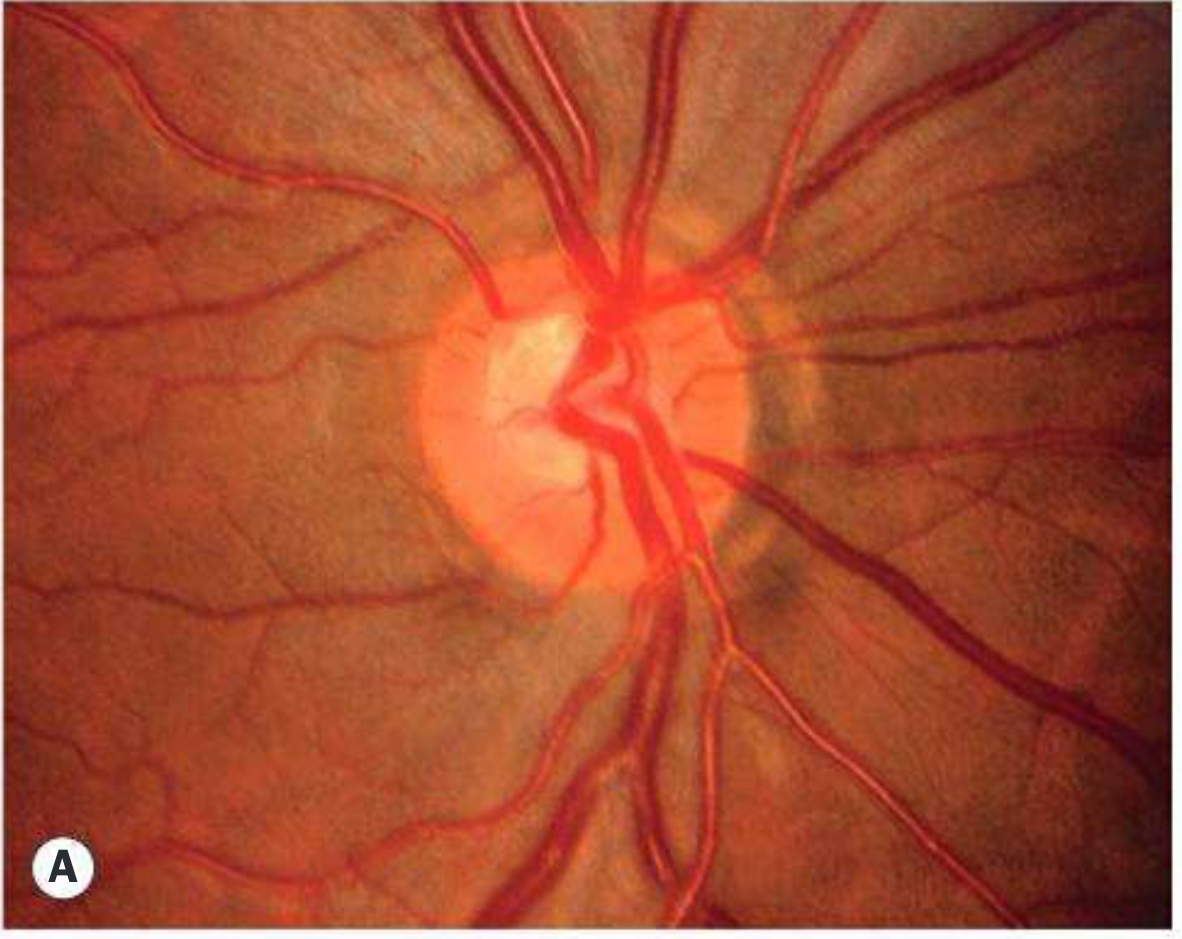
5D. FUNDUS EXAMINATION — OPTIC DISC CHANGES
Normal Optic Disc (Know Before Abnormal)
NORMAL DISC
│
├── Neuroretinal rim (NRR): orange-pink tissue between cup and disc margin
├── ISNT Rule: Inferior > Superior > Nasal > Temporal rim width (broadest to narrowest)
├── Cup/disc (C/D) ratio: vertical C/D ratio used
│ ├── Only 2% population has C/D >0.7
│ └── Asymmetry ≥0.2 between eyes = suspicious
├── Normal disc vertical diameter: 1.5–1.7 mm (white population)
└── Small disc = small cup (may be normal); Large disc = large cup (may be normal)
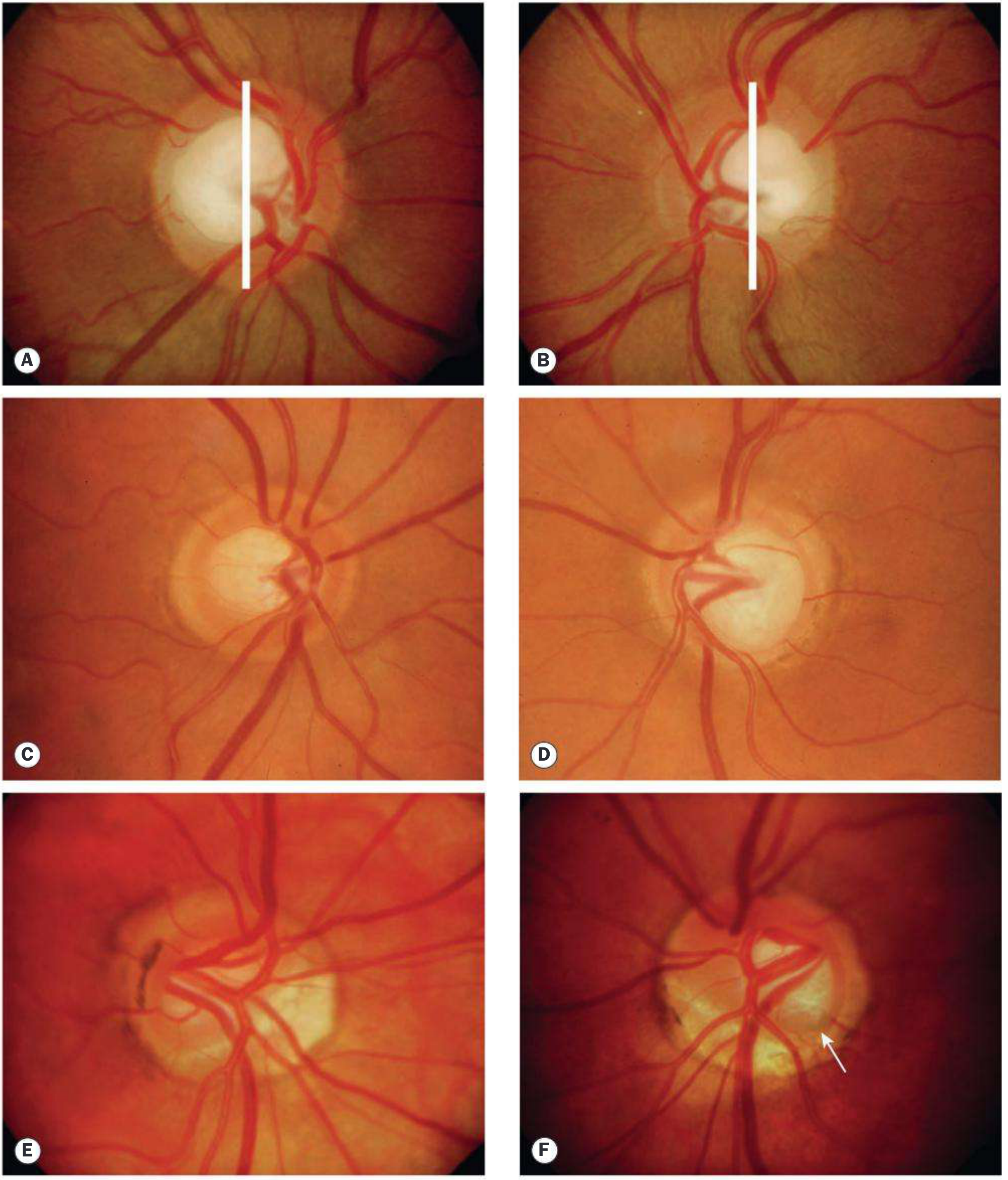
Glaucomatous Optic Disc Changes — FLOWCHART
EARLY CHANGES
│
├── Increased C/D ratio (vertical > horizontal)
├── Focal NRR notching (especially inferior pole — inferotemporal is FIRST affected)
├── ISNT rule VIOLATED
├── Asymmetry of C/D ≥0.2 between eyes
├── RNFL defects (slit/wedge-shaped, superior or inferior arcuate zones)
└── Disc haemorrhage (splinter — infero-temporal, risk factor for progression)
│
▼
PROGRESSIVE CHANGES
│
├── Generalised enlargement of cup (concentric)
├── Bayonetting sign — vessels disappear over rim edge, reappear in cup
├── Vertical elongation of cup
├── NRR becoming thinner
├── Vessel nasalisation (vessels displaced to nasal side)
└── Baring of circumlinear vessels
│
▼
ADVANCED / LATE CHANGES
│
├── Bean-pot cupping (overhanging edges)
├── Cup-disc ratio approaching 1.0
├── Near total NRR loss
├── Pallor of remaining rim
├── Peripapillary atrophy (beta-zone most significant)
└── Disc haemorrhages (more common in NTG)
Pictorial reference from Kanski:
5E. PERIMETRY (Visual Fields)
STANDARD AUTOMATED PERIMETRY (SAP) — Humphrey Field Analyser
│
├── Relatively INSENSITIVE in early disease
├── 25–35% of RGC lost before field defect detected
│
├── EARLY DEFECTS:
│ ├── Increased response variability (before actual defects)
│ ├── Paracentral scotoma — superonasal (most common first defect)
│ ├── Nasal step — sensitivity difference above/below horizontal midline
│ └── Temporal wedge
│
├── PROGRESSIVE DEFECTS:
│ ├── Arcuate (Bjerrum) scotoma — follows RNFL arc above/below fixation
│ ├── Seidel scotoma — comet-shaped extension from blind spot
│ ├── Ring scotoma (double arcuate)
│ └── Central field loss
│
├── ADVANCED DEFECTS:
│ ├── Altitudinal defect
│ └── Tubular/gun-barrel vision (central island + temporal island remaining)
│
├── SPECIAL MODALITIES:
│ ├── FDT (Frequency Doubling Technology) — detects defects EARLIER
│ ├── SWAP (Short Wavelength Automated Perimetry) — earlier defects
│ └── SITA (Swedish Interactive Threshold Algorithm) — fast, standard strategy
│
├── GLOBAL INDICES:
│ ├── Mean Deviation (MD) — average sensitivity loss
│ ├── Pattern Standard Deviation (PSD) — localized loss
│ └── Visual Field Index (VFI) — percentage of normal function
│
└── PROGRESSION: Change in MD >1 dB/year = clinically significant progression
EMGT natural history (untreated):
• HTG: -1.31 dB/year
• NTG: -0.36 dB/year
• PXEG: -3.13 dB/year
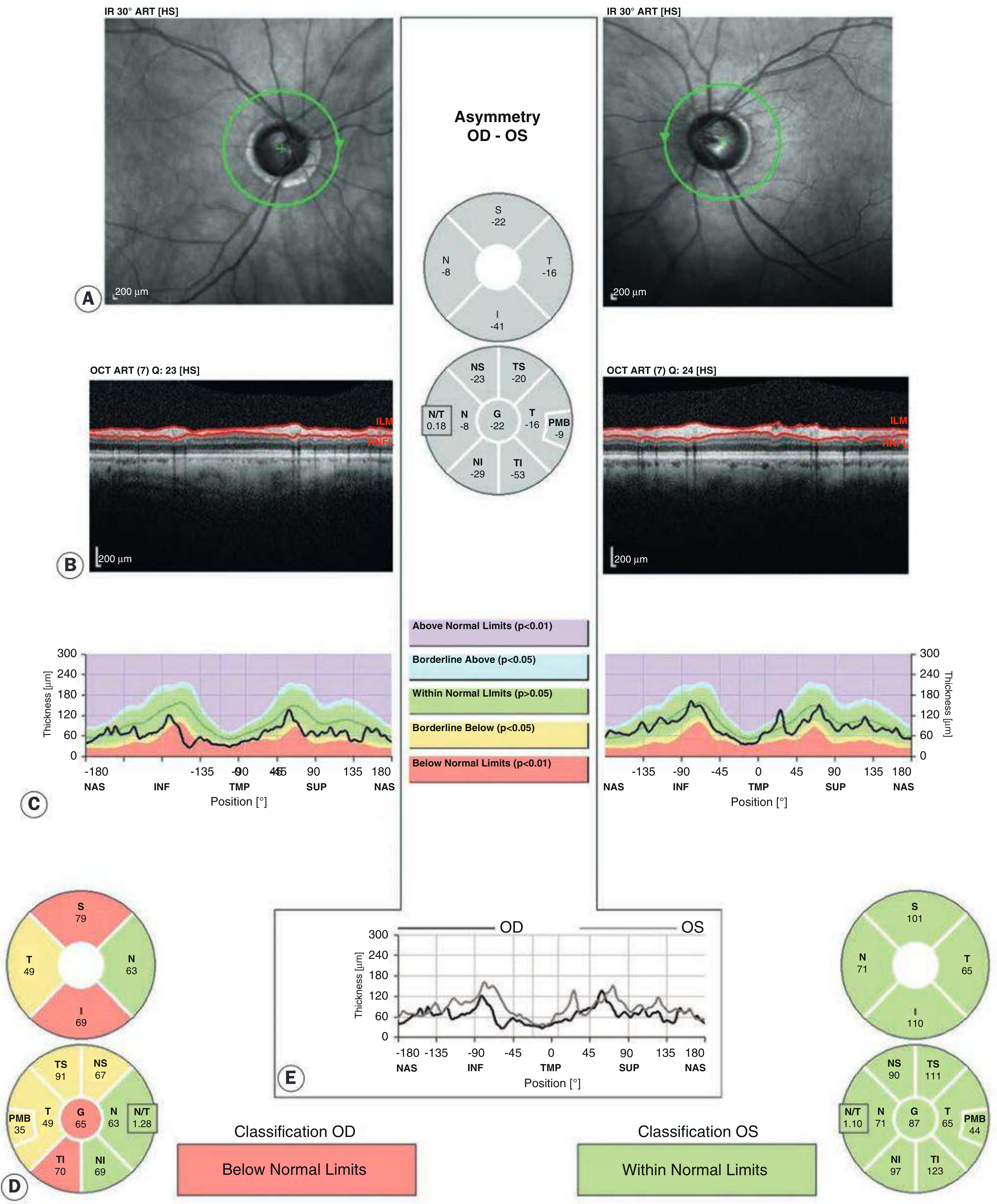
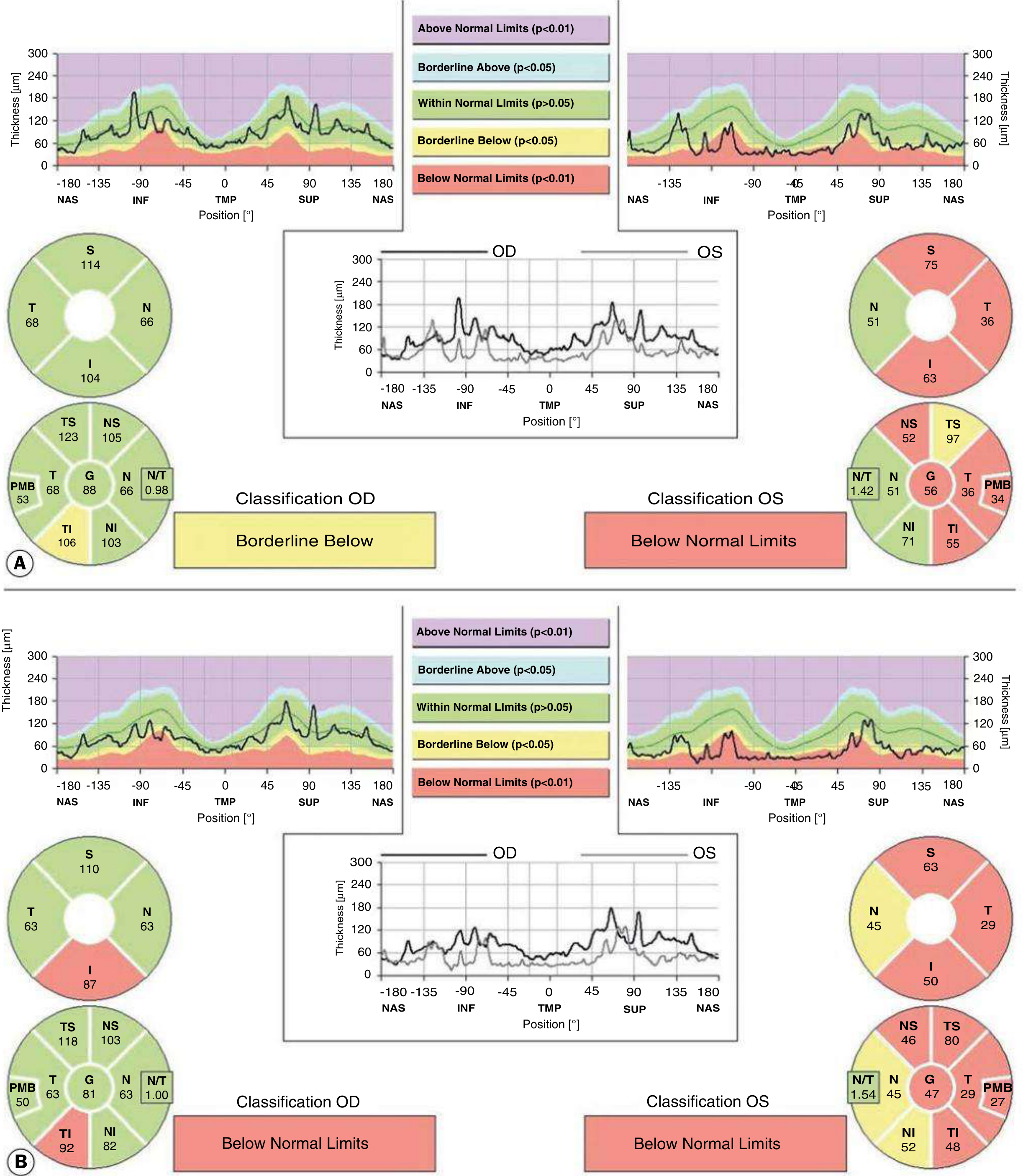
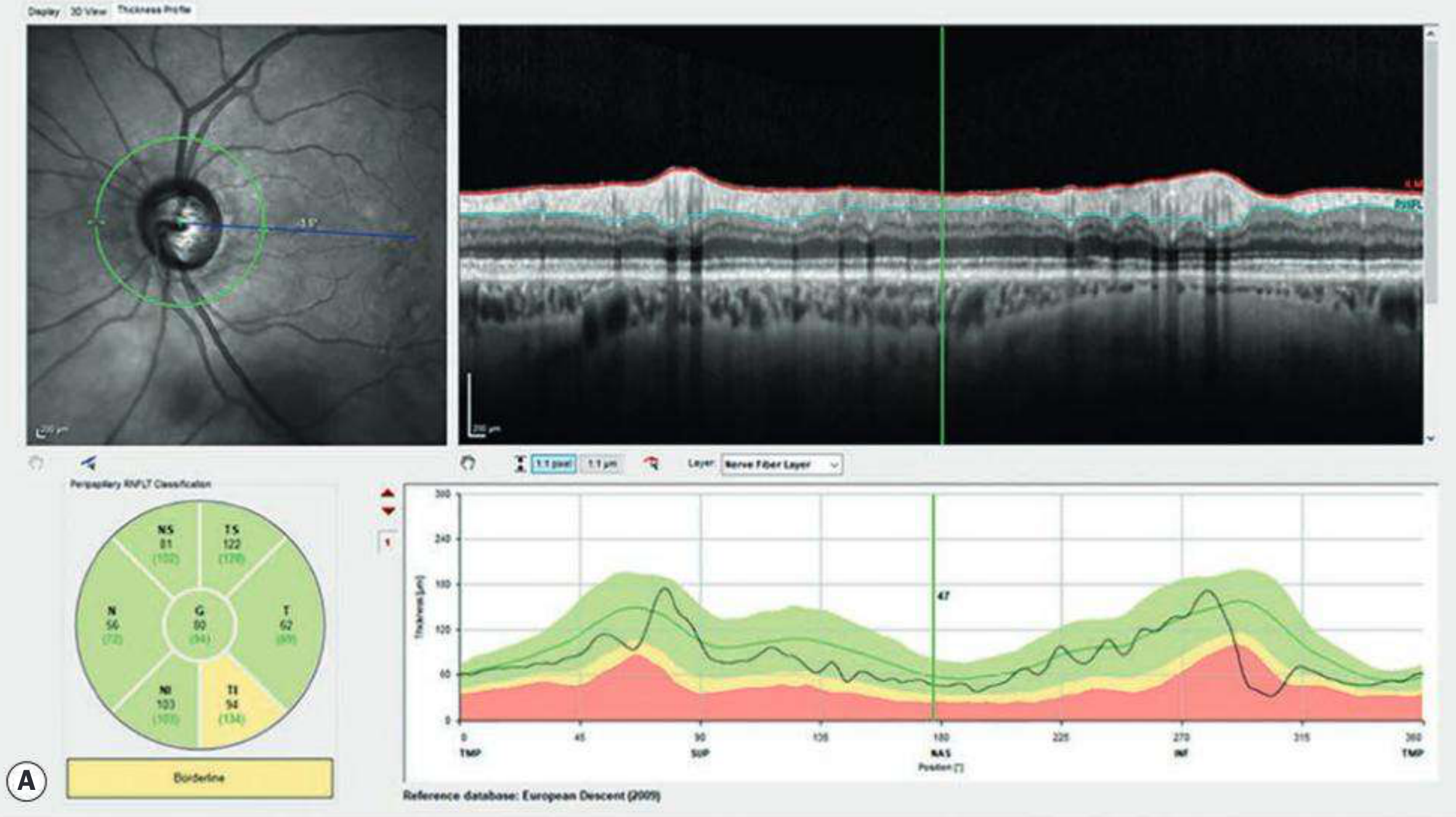
5F. OCT (Optical Coherence Tomography)
OCT IN GLAUCOMA — Has largely superseded other imaging
│
├── WHAT IT MEASURES:
│ ├── RNFL thickness (peripapillary — 3.46mm circle around disc)
│ ├── Optic disc parameters (rim area, C/D ratio)
│ ├── Ganglion cell complex (GCC) / macular GCL thickness
│ └── Bruch's membrane opening — minimum rim width (BMO-MRW)
│
├── TSNIT GRAPH (Temporal-Superior-Nasal-Inferior-Temporal):
│ ├── Normal: "double hump" pattern (superior and inferior peaks)
│ ├── Glaucoma: loss of inferior hump FIRST (inferotemporal RNFL)
│ └── Colour code: GREEN = normal, YELLOW = borderline, RED = abnormal
│
├── EARLY GLAUCOMA FINDINGS:
│ ├── Inferotemporal RNFL thinning (first area affected)
│ ├── Superior RNFL thinning (second)
│ ├── Ganglion cell layer thinning inferior to fovea
│ └── Macular GCL thinning — may detect earlier than perimetry
│
├── PROGRESSION MONITORING:
│ ├── Serial RNFL maps compared over time
│ ├── Trend-based analysis (slope of change)
│ └── Guided progression analysis (GPA)
│
└── IMPORTANT: OCT detects structural changes BEFORE visual field defects
→ "Structure before function" principle
OCT images from Kanski:
SECTION 6: TREATMENT PROTOCOL
6A. TREATMENT GOAL
PRIMARY AIM: Prevent functional vision impairment within patient's lifetime
by REDUCING IOP (only proven method)
TARGET PRESSURE:
├── Based on: severity of damage (C/D ratio, MD on VF), pre-treatment IOP,
│ CCT, rate of progression, age, general health
├── Reasonable initial goal: IOP < 18 mmHg
│ (AGIS trial: visual field progression unlikely if IOP <18 mmHg at ALL times)
└── If target not achieved → adjust target lower
If progression despite target → consider surgery
6B. MEDICAL THERAPY — STEP-BY-STEP
STEP 1 — FIRST LINE: PROSTAGLANDIN ANALOGUES (PGAs)
│
├── Mechanism: ↑ uveoscleral outflow (mainly); some ↑ trabecular outflow
├── IOP reduction: 27–35% from baseline
├── Dosing: ONCE daily (bedtime)
├── Systemic side effects: MINIMAL
│
├── AGENTS:
│ ├── Latanoprost 0.005% — fewest ocular adverse events; used first
│ ├── Travoprost 0.004% — fewer non-responders; Polyquad preservative
│ ├── Bimatoprost 0.03% — greatest IOP reduction; more hyperaemia
│ │ (0.01% — same IOP reduction, less hyperaemia)
│ ├── Tafluprost — preservative-free; good for ocular surface disease
│ └── Omidenepag 0.002% — new EP2 agonist; no periorbitopathy; 5% hyperaemia
│
├── KEY SIDE EFFECTS:
│ ├── Conjunctival hyperaemia (most common)
│ ├── Increased iris pigmentation (irreversible)
│ ├── Eyelash growth (hypertrichosis)
│ ├── Periorbital fat atrophy (periorbitopathy — deepened upper lid sulcus)
│ └── CMO (cystoid macular oedema) — in aphakic/pseudophakic eyes
│
└── NOTE: Never use 2 PGAs together → paradoxical IOP RISE
│ If IOP inadequate
▼
STEP 2 — ADD: BETA-BLOCKER
│
├── Timolol 0.25% or 0.5% — twice daily (or gel-forming — once daily)
├── Betaxolol — cardioselective (safer in mild asthma)
├── Mechanism: ↓ aqueous humour production
├── IOP reduction: 20–25%
│
└── CONTRAINDICATIONS:
├── Asthma / COPD
├── Heart failure
├── Heart block (2nd/3rd degree)
└── Peripheral vascular disease
│ If IOP still inadequate
▼
STEP 3 — ADD: CARBONIC ANHYDRASE INHIBITOR (CAI)
│
├── TOPICAL: Dorzolamide 2% (TDS) / Brinzolamide 1% (BD-TDS)
├── SYSTEMIC: Acetazolamide 250–500 mg (short-term only)
│ (Contraindicated if sulfonamide allergy)
├── Mechanism: ↓ aqueous production by inhibiting CA-II in ciliary epithelium
└── IOP reduction: 15–20%
│ If IOP still inadequate
▼
STEP 4 — ADD: ALPHA-2 AGONIST
│
├── Brimonidine 0.15–0.2% (BD-TDS)
├── Mechanism: ↓ aqueous production + ↑ uveoscleral outflow
├── IOP reduction: 20–25%
├── Additional: possible neuroprotective effect
└── SIDE EFFECTS: allergy/follicular conjunctivitis (15%), fatigue, dry mouth
AVOID in children <2 yrs (CNS depression)
│ If IOP still inadequate
▼
STEP 5 — FIXED COMBINATIONS (improve adherence)
│
├── Timolol + Dorzolamide (Cosopt)
├── Timolol + Brimonidine (Combigan)
├── Timolol + Latanoprost (Xalacom)
└── Timolol + Bimatoprost (Ganfort)
│ If max medical therapy fails
▼
STEP 6 — LASER / SURGICAL THERAPY
6C. LASER TREATMENT
SELECTIVE LASER TRABECULOPLASTY (SLT)
│
├── Laser: Q-switched Nd:YAG, 532 nm
├── Target: Pigmented TM cells selectively
├── Energy: 0.4–1.2 mJ; 50 spots over 180° or 360°
├── IOP reduction: 20–30%
├── Repeatable (unlike ALT)
├── Can be used as FIRST LINE (LiGHT trial: SLT = first-line drops at 3 yrs)
└── Side effects: transient IOP spike, mild iritis
ARGON LASER TRABECULOPLASTY (ALT) — older, largely replaced by SLT
├── Burns TM, causing mechanical stretching
└── Not easily repeatable (scarring)
LASER IRIDOTOMY — for angle closure, NOT POAG (but know it)
6D. SURGICAL TREATMENT
TRABECULECTOMY — Gold standard filtering surgery
│
├── Creates new aqueous drainage pathway (fistula) under conjunctival bleb
├── Anti-metabolites:
│ ├── Mitomycin C (MMC) — more potent, longer effect
│ └── 5-Fluorouracil (5-FU) — less potent, multiple injections
├── Target IOP: <15 mmHg achievable
├── Complications:
│ ├── Bleb failure (fibrosis)
│ ├── Hypotony (over-drainage)
│ ├── Bleb-related infection (blebitis → endophthalmitis)
│ └── Cataract progression
GLAUCOMA DRAINAGE DEVICES (GDD) — Tube surgery
├── Ahmed, Baerveldt, Molteno implants
├── Used when trabeculectomy failed or high risk
└── IOP reduction reliable, moderate
NON-PENETRATING FILTERING SURGERY
├── Deep sclerectomy — Descemet window created; collagen implant + goniopuncture
└── Viscocanalostomy — Schlemm canal dilated with viscoelastic
MINIMALLY INVASIVE GLAUCOMA SURGERY (MIGS) — Most Recent
│
├── GROUP 1 — Schlemm canal procedures (NO bleb):
│ ├── Trabectome — electro-ablation of TM (ab interno)
│ ├── Kahook Dual Blade — excise TM strip
│ ├── iStent inject — 2 titanium stents bypassing TM
│ └── Hydrus Microstent — scaffold to dilate Schlemm canal
│
├── GROUP 2 — Subconjunctival drainage (BLEB-forming):
│ ├── Xen Gel Stent — 45-micron lumen gelatin tube
│ ├── Preserflo MicroShunt — SIBS polymer
│ └── (± MMC injection at time of insertion)
│
└── GROUP 3 — Supraciliary/suprachoroidal drainage (NO bleb):
└── MINIject — silicone implant into supraciliary space
INDICATIONS FOR MIGS:
├── Mild to moderate glaucoma
├── Target IOP: 15–17 mmHg
└── Often combined with phacoemulsification (cataract + glaucoma together)
CYCLODIODE LASER (CYCLOABLATION)
├── Destroys ciliary body epithelium → ↓ aqueous production
└── Reserved for end-stage / pain relief
6E. TREATMENT ALGORITHM — SUMMARY FLOWCHART
NEWLY DIAGNOSED POAG
│
▼
CONFIRM DIAGNOSIS (IOP, gonioscopy, disc, VF, OCT)
│
▼
SET TARGET IOP (based on damage severity, CCT, age)
│
▼
START: PROSTAGLANDIN ANALOGUE (once daily bedtime)
│
IOP at target? ──YES──→ MONITOR (every 3–6 months)
│NO
▼
ADD: BETA-BLOCKER (or CAI if contraindicated)
│
IOP at target? ──YES──→ MONITOR
│NO
▼
ADD: 3rd AGENT or FIXED COMBINATION
│
IOP at target? ──YES──→ MONITOR
│NO
▼
CONSIDER: SLT LASER (can also use as 1st line — LiGHT trial)
│
IOP at target? ──YES──→ MONITOR
│NO
▼
SURGICAL OPTIONS:
├── Mild-Moderate → MIGS (especially if combined with cataract surgery)
├── Moderate-Severe → TRABECULECTOMY ± MMC
└── Failed trabeculectomy / High risk → TUBE (GDD)
│
Still progressing despite target IOP?
│
▼
LOWER TARGET FURTHER + Consider cyclodiode (end-stage)
SECTION 7: MONITORING PROTOCOL
MONITORING IN POAG
│
├── FREQUENCY:
│ ├── Newly diagnosed / medication change: 4–6 weeks (IOP check)
│ ├── Stable, controlled: every 3–6 months
│ └── Visual fields: at least annually (more often if progressing)
│
├── EACH VISIT:
│ ├── VA, IOP (note time of day)
│ ├── Slit lamp (disc appearance, bleb if post-op)
│ ├── VF (annual or biannual)
│ └── OCT RNFL (annual or biannual)
│
└── PROGRESSION CRITERIA:
├── VF: MD change >1 dB/year, confirmed on ≥2 tests
├── OCT: Significant RNFL thinning on serial measurements
└── Disc: New haemorrhage, notch enlargement, NRR loss
SECTION 8: SCREENING
WHO TO SCREEN (High-risk case finding):
│
├── Age >40 yrs with 1st-degree family history of POAG
├── All individuals >60 yrs (especially African descent from age 40)
├── African / Afro-Caribbean racial background
└── Myopes, OHT patients
SCREENING COMPONENTS (tonometry alone is INSUFFICIENT):
├── Tonometry (IOP)
├── Visual field assessment
├── Ophthalmoscopy (disc evaluation)
└── Ideally: pachymetry + gonioscopy for high-risk individuals
QUICK EXAM REVISION TABLE
| Feature | Detail |
|---|---|
| RGC death mechanism | Apoptosis (NOT necrosis) |
| Pre-terminal event | Ca²⁺ influx + ↑ nitric oxide |
| Key gene | MYOC (myocilin) + OPTN (optineurin) |
| First VF defect | Paracentral scotoma (superonasal) |
| First OCT change | Inferotemporal RNFL thinning |
| ISNT rule | Inferior > Superior > Nasal > Temporal (NRR width) |
| Target IOP (AGIS) | <18 mmHg for no significant progression |
| 1st line drug | Prostaglandin analogue (once daily bedtime) |
| PGA IOP reduction | 27–35% |
| Beta-blocker IOP reduction | 20–25% |
| Laser 1st line option | SLT (LiGHT trial proven) |
| Gold standard surgery | Trabeculectomy ± MMC |
| Newest surgery group | MIGS |
| C/D >0.7 | Only 2% of normal population |
| C/D asymmetry | ≥0.2 between eyes — suspicious |
| Disc haemorrhage site | Inferotemporal (most common) |
| EMGT untreated HTG | -1.31 dB/year loss |
Source: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition — Chapter 11: Glaucoma
This is a shared conversation. Sign in to Orris to start your own chat.