Bundle pacing
Reading File
Finding Sources
Finding Sources
Searching PubMed
"left bundle branch area pacing" OR "His bundle pacing"
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative sources. Let me compile the full answer.
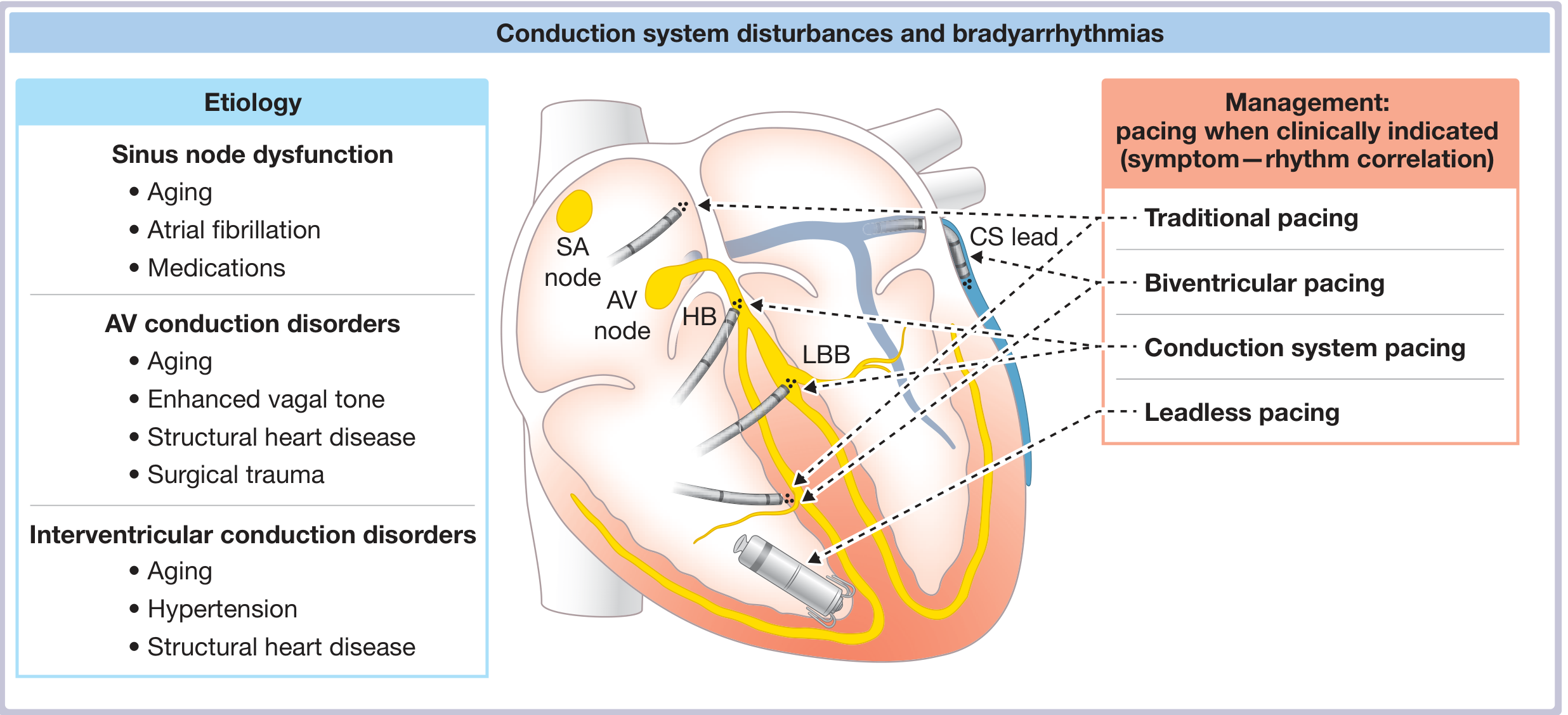
Conduction System (Bundle) Pacing
Conduction system pacing (CSP) is an umbrella term for pacing modalities that engage the His-Purkinje system to produce physiologic ventricular activation, avoiding the dyssynchrony caused by conventional right ventricular (RV) apex pacing. The two main forms are His bundle pacing (HBP) and left bundle branch area pacing (LBBAP/LBBP).
Why It Matters: The Problem with RV Pacing
Conventional RV apical pacing activates the ventricles in a non-physiologic, myocyte-to-myocyte wavefront, creating interventricular and intraventricular dyssynchrony. With prolonged RV pacing burden (>40% of beats), this can lead to:
- Pacing-induced cardiomyopathy (PICM)
- Deterioration of LV systolic function
- Increased risk of heart failure and AF
Conduction system pacing preserves or restores normal electrical activation by recruiting the His-Purkinje system. - Fuster and Hurst's The Heart, 15th Ed., p. 1237
Anatomy Relevant to CSP
- The His bundle is a cylindrical fascicle extending inferiorly and leftward from the AV node. It has two segments: a penetrating portion (~5-10 mm, over the atrial membranous septum) and a branching portion (~5-10 mm, where the left bundle branch [LBB] begins to fan out).
- The LBB fans out beneath the LV subendocardium - a wider target than the narrow His bundle. It divides into anterior and posterior fascicles, each heading toward the corresponding papillary muscle head.
- Purkinje fibers arborize from the fascicles into the ventricular myocardium. - Fuster & Hurst, p. 1237
1. His Bundle Pacing (HBP)
First described for permanent pacing in 2000 (Deshmukh et al.), HBP directly stimulates the bundle of His, engaging the downstream His-Purkinje system.
Types of His Bundle Capture
| Type | Mechanism | ECG Features |
|---|---|---|
| Selective HBP (S-HBP) | His bundle only; ventricular activation entirely via HPS | S-QRS = native H-QRS; paced QRS = native QRS morphology; isoelectric interval between spike and QRS; discrete local ventricular EGM on lead |
| Nonselective HBP (NS-HBP) | His bundle + adjacent RV myocardium fused | S-QRS = 0 (no isoelectric interval); wider QRS than S-HBP due to fusion; no discrete local ventricular EGM |
In patients with His-Purkinje conduction disease (HPCD, e.g. BBB or HV block), HBP can correct the bundle branch block by capturing latent fascicular tissue distal to the site of block - in this setting, the paced QRS may be narrower than the native QRS, and two distinct capture thresholds may be observed (with and without BBB correction). - Fuster & Hurst, p. 1238
Limitations of HBP
- Technically demanding (small target)
- Pacing thresholds are sometimes high (~1-2 V) and may rise over time
- Lead revisions required in ~6.7% of cases
- Undersensing of ventricular signals and atrial oversensing can occur
- In infranodal block, backup pacing safety is a concern if the lead is above the site of block - Fuster & Hurst, p. 1239
2. Left Bundle Branch Area Pacing (LBBAP / LBBP)
Introduced by Huang et al. (2017), LBBAP emerged to overcome the limitations of HBP. The lead is screwed deep into the proximal interventricular septum from the RV side until it crosses the septum and engages the LBB or its proximal fascicles.
Definition: Direct capture of the LBB or one of its fascicles along with the LV septal myocardium at low output (<1 V at 0.5 ms pulse width). - Fuster & Hurst, p. 1240
LBBAP vs. HBP - Key Advantages
| Feature | HBP | LBBAP |
|---|---|---|
| Target size | Small (His bundle, ~1-2 mm) | Larger (LBB fan, ~10-15 mm wide) |
| Pacing threshold | Often higher, can rise | Lower and more stable |
| Sensing (R-wave) | Often lower | Higher |
| Lead stability | Less predictable | More reliable |
| BBB correction | Can correct supra-Hisian block | Corrects LBBB by pacing distal to the block |
| Safety backup | Concern in infranodal block | Lead position distal to AV node provides backup |
ECG Criteria for LBBAP
- Right bundle branch block (RBBB) morphology in V1 (current flowing away from RV lead toward LV)
- Narrow or normal QRS duration (when LBB is captured)
- Short R-wave peak time (RWPT) in V5-V6 (<80 ms) confirming fast LV activation
- A "W" pattern may be seen in V6 if only septal myocardium is captured without true LBB capture
Indications for Conduction System Pacing
CSP is particularly preferred over RV pacing in:
- Patients with LVEF <50% and AV block who are expected to require >40% ventricular pacing - to prevent heart failure. - Harrison's Principles of Internal Medicine, 22nd Ed., p. 1974
- Patients with existing or anticipated pacing-induced cardiomyopathy
- Patients with LBBB and heart failure who need cardiac resynchronization therapy (CRT) - as an alternative to biventricular pacing
- AV node ablation for AF - to prevent RV pacing-induced dyssynchrony
- Patients where biventricular pacing (CRT) has failed or coronary sinus lead placement is not feasible
Harrison's states: "The selection of pacing lead location should be individualized based on expected pacing requirements, underlying heart disease, and level of conduction block." - Harrison's 22nd Ed., p. 1974
Goldman-Cecil notes: "Cardiac resynchronization therapy requires synchronized pacing of both ventricles or physiologic pacing by means of His-bundle pacing or left bundle branch pacing." - Goldman-Cecil Medicine
Clinical Outcomes (from Fuster & Hurst Tables 38-9 and 38-10)
HBP outcomes (selected studies):
- Deshmukh 2000: 18 patients with AF + AV node ablation; 66% success; improved LVEF, NYHA, LV dimensions at 36 months
- Deshmukh 2004: 54 patients; 72% success; improved LVEF, NYHA, peak VO₂ at 42 months
- Multicenter registry (Vijayaraman 2018): Success rates improved to >90% with dedicated tools; long-term thresholds generally stable
LBBAP outcomes (selected studies):
- Implant success rates: 80-100% across studies
- Paced QRS duration: 110-140 ms (near-normal)
- Pacing thresholds: 0.5-0.8 V at 0.5 ms - stable
- R-wave sensing: 9-18 mV - excellent
- Lead revision rates: 0-3%
Recent Evidence (2024-2026)
Three recent meta-analyses reinforce the role of LBBAP:
-
El Iskandarani et al. (2024) - Systematic review & meta-analysis in heart failure found LBBAP achieves significant improvement in LVEF and NYHA class in heart failure patients. [PMID: 38812213]
-
Ellenbogen KA et al. (2024) - Meta-analysis of lumenless leads for LBBAP: confirmed favorable pacing parameters with lumenless (SelectSecure-type) leads. [PMID: 38664898]
-
Chen X & Dong J (2024) - Stylet-driven vs. lumenless leads for LBBAP: both lead types are feasible, each with distinct implant characteristics. [PMID: 39462327]
Practical Summary
| Aspect | HBP | LBBAP |
|---|---|---|
| Physiologic? | Yes (most physiologic) | Yes (near-physiologic) |
| Technical difficulty | High | Moderate |
| Threshold stability | Variable (can rise) | Generally stable and low |
| BBB correction | Yes (for supra-Hisian block) | Yes (for LBBB) |
| Preferred when | Normal His-Purkinje, mild HPCD | LBBB, high HBP threshold, failed HBP |
| Backup safety | Concern in infranodal block | Better (distal to AV node) |
Both modalities represent a major advance over conventional RV pacing. LBBAP has largely supplanted HBP at many centers due to its more favorable lead parameters, but HBP remains the reference standard for true physiologic (complete His-Purkinje system) activation.
This is a shared conversation. Sign in to Orris to start your own chat.