Differential diagnosis of acute diarrhoea and points to rule out that differential diagnosis
Reading File
Finding Sources
Finding Sources
Searching PubMed
"acute diarrhea" AND "differential diagnosis"
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive data from Harrison's 22E, Sleisenger & Fordtran, Goldman-Cecil, and the Washington Manual. Let me compile the full answer.
Differential Diagnosis of Acute Diarrhoea
Acute diarrhoea is defined as the passage of 3 or more loose/watery stools per day lasting <14 days (some sources use <4 weeks). Over 80-90% of cases are infectious in origin; the remaining 10-20% are due to drugs, toxins, ischemia, and other causes.
Diagnostic Algorithm
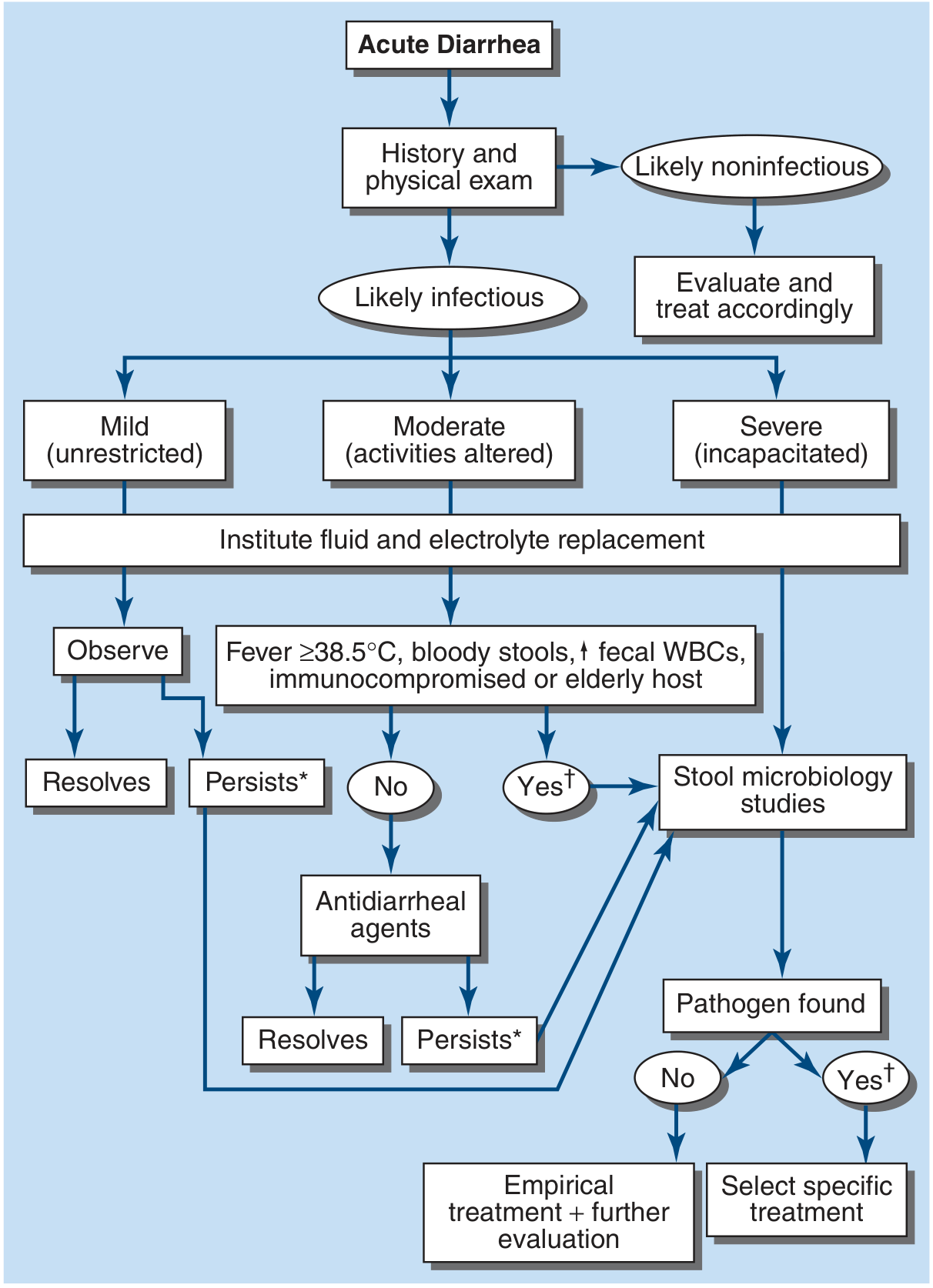
Figure 49-3 from Harrison's Principles of Internal Medicine 22E - Algorithm for management of acute diarrhea
Classification Framework
Acute diarrhoea is best classified into three syndromes, which guide the differential:
| Syndrome | Character | Mechanism |
|---|---|---|
| Watery / Non-inflammatory | Large volume, no blood/pus | Secretory or osmotic |
| Inflammatory / Dysenteric | Small volume, blood, pus, fever, tenesmus | Mucosal invasion or cytotoxin |
| Food poisoning | Abrupt onset (1-6 h), vomiting-predominant | Preformed toxin |
1. INFECTIOUS CAUSES (>80%)
A. Viral
| Agent | Key Clinical Features | Rule-Out Points |
|---|---|---|
| Norovirus (Norwalk) | Most common cause of outbreaks; 12-48 h incubation; explosive watery diarrhoea + vomiting; resolves 24-72 h; cruise ship/closed settings | Stool PCR multiplex or antigen assay; outbreak context; no blood |
| Rotavirus | Predominantly infants/children (winter); watery diarrhoea + vomiting + fever; adults (especially elderly) can be affected | Stool rotavirus antigen; age group; seasonal pattern |
| Adenovirus | Children; prolonged (>7 days); less vomiting than rotavirus | Stool PCR; prolonged duration |
| Cytomegalovirus (CMV) | Immunocompromised (HIV, transplant); bloody diarrhoea | CMV PCR/pp65 antigen; colonoscopy showing ulcers; low CD4 count |
| SARS-CoV-2 | Diarrhoea may be an early/sole symptom | SARS-CoV-2 nasopharyngeal/stool PCR; concurrent respiratory symptoms |
To rule out viral cause: Stool multiplex PCR (sensitivity >90%). Patients with pure viral illness have normal or lymphocyte-predominant WBC and no fecal leukocytes.
B. Bacterial - Non-invasive (Watery, No Fever)
These organisms produce toxins or colonise without invading the mucosa.
| Agent | Key Clinical Features | Incubation | Rule-Out Points |
|---|---|---|---|
| Enterotoxigenic E. coli (ETEC) | #1 cause of traveller's diarrhoea; profuse watery diarrhoea; no fever; self-limited | 1-3 days | Travel history; stool PCR/culture; no fecal leukocytes |
| Vibrio cholerae | Rice-water stools, massive fluid loss; cholera-endemic area; no fever | Hours-2 days | Travel to endemic area; dark-field microscopy; stool culture on TCBS agar |
| Staphylococcus aureus | Sudden onset, predominantly vomiting, mayonnaise/cream foods, resolves <24h | 1-6 hours | Food history (preformed toxin); no fever; short incubation; stool toxin assay |
| Bacillus cereus | Two syndromes: emetic (fried rice, 1-6h) and diarrhoeal (meat/vegetables, 8-16h) | 1-16 hours | Reheated rice/food; short duration; no fever; culture food source |
| Clostridium perfringens | Watery diarrhoea + cramps; vomiting rare; banquet/institutional food | 8-16 hours | Large-group outbreak after meat/gravy; no fever; stool culture; spore count |
C. Bacterial - Invasive (Inflammatory/Dysenteric - Fever, Blood, Pus)
| Agent | Key Clinical Features | Incubation | Rule-Out Points |
|---|---|---|---|
| Salmonella (non-typhoidal) | Fever + bloody diarrhoea; poultry, eggs, reptiles; may cause bacteremia in sickle cell | 12-48 h | Stool culture; blood culture if systemic; CBC shows leukocytosis with neutropenia possible |
| Shigella | Classic dysentery; high fever, tenesmus, small bloody stools; very low inoculum; person-to-person | 1-3 days | Stool culture; fecal leukocytes; seizures in children; Reiter's syndrome post-infection |
| Campylobacter jejuni | Most common bacterial cause in many countries; bloody diarrhoea; "prodrome" of fever/myalgia; poultry; reactive arthritis | 2-5 days | Stool culture (special conditions, 42°C, microaerophilic); Guillain-Barre syndrome association |
| Enterohemorrhagic E. coli (EHEC O157:H7) | Bloody diarrhoea WITHOUT fever (distinguishing feature); undercooked hamburger; complication: HUS | 3-8 days | Stool culture on SMAC agar; Shiga toxin assay; do NOT use antibiotics (HUS risk) |
| Yersinia enterocolitica | Right lower quadrant pain mimicking appendicitis; fever; bloody diarrhoea; pork; cold climates | 4-7 days | Cold enrichment culture; serology; mesenteric lymphadenitis on CT |
| Clostridioides difficile | Recent antibiotic use or hospitalisation; profuse watery ± bloody diarrhoea; pseudomembranes on sigmoidoscopy | Variable | Stool toxin A/B EIA + PCR (two-test approach); colonoscopy shows pseudomembranes; hyperleukocytosis |
| Vibrio parahaemolyticus | Seafood (raw shellfish/oysters); watery to bloody; fever | 4-96 h | Seafood history; stool culture on TCBS agar |
| Aeromonas/Plesiomonas | Untreated water, aquatic exposure; traveller's diarrhoea | 1-2 days | Stool culture (often not routinely done - special request) |
| Listeria monocytogenes | Pregnant women, elderly, immunocompromised; soft cheeses, cold cuts; bacteremia | 9-48 h (GI) | Blood/stool culture; CBC (monocytosis); maternal exposure history |
D. Parasitic
| Agent | Key Clinical Features | Rule-Out Points |
|---|---|---|
| Giardia lamblia | Most common parasitic cause; hikers/campers (contaminated water); foul-smelling, greasy stools; bloating; NO blood; may persist | Stool antigen (ELISA/PCR); ova and parasites (3 samples); string test/duodenal aspirate |
| Entamoeba histolytica | Travellers, MSM; flask-shaped ulcers; bloody diarrhoea; RUQ pain (liver abscess); progressive | Stool antigen assay (distinguish from non-pathogenic E. dispar); serology; colonoscopy |
| Cryptosporidium | Immunocompromised (HIV with CD4 <200); also immunocompetent with large-volume watery diarrhoea; waterborne | Modified acid-fast stain of stool; stool PCR; CD4 count |
| Cyclospora cayetanensis | Travellers; imported produce (raspberries, basil); relapsing watery diarrhoea | Modified acid-fast stain (cyclospora oocysts are larger than Cryptosporidium); UV autofluorescence |
| Isospora (Cystoisospora) belli | AIDS patients; prolonged watery diarrhoea; tropical regions | Modified acid-fast stain; stool ova and parasites |
| Microsporidia | AIDS (CD4 <100); watery diarrhoea; wasting | Modified trichrome stain; electron microscopy; PCR |
2. NON-INFECTIOUS CAUSES (~10-20%)
A. Medication-Induced
Common culprits:
- Antibiotics (almost any; particularly clindamycin, broad-spectrum penicillins) - also trigger C. difficile
- Laxatives (osmotic/stimulant)
- Antacids (Mg-containing)
- NSAIDs (mucosal damage)
- Metformin (secretory, dose-dependent)
- Colchicine (enterocyte membrane damage)
- Digoxin, quinidine
- Immune checkpoint inhibitors (anti-CTLA-4, anti-PD-1/PD-L1) - colitis in up to 40%
- Olmesartan (sprue-like enteropathy)
- Cancer chemotherapy (5-FU, irinotecan, oxaliplatin)
To rule out: Medication reconciliation; resolution with drug withdrawal; fecal calprotectin and endoscopy for checkpoint inhibitor colitis.
B. Ischemic Colitis
Acute ischemia of the colon presents as sudden crampy left lower quadrant pain followed by bright red blood per rectum (often not truly "diarrhoea" but haematochezia). Risk factors: older age, atherosclerosis, hypotension, post-aortic surgery, vasopressors, cocaine use.
To rule out:
- CT abdomen (colonic wall thickening, "thumb printing")
- Flexible sigmoidoscopy/colonoscopy (pale mucosa, submucosal haemorrhage at watershed areas - splenic flexure, rectosigmoid junction)
- Serum lactate (elevated in transmural ischemia)
C. Inflammatory Bowel Disease (IBD) - First Presentation
Crohn's disease or ulcerative colitis can first manifest as acute bloody diarrhoea mimicking infection.
To rule out:
- Stool cultures and C. difficile assay (must exclude infection first)
- Fecal calprotectin (markedly elevated in IBD)
- Colonoscopy with biopsies (contiguous involvement with crypt abscesses in UC; skip lesions in Crohn's)
- CRP, ESR, CBC
D. Diverticulitis
Acute diverticular inflammation/infection causes LIF pain, fever, altered bowel habit (diarrhoea or constipation), and occasionally rectal bleeding.
To rule out:
- CT abdomen/pelvis with contrast (pericolonic fat stranding, pericolic abscess, air)
- Avoid colonoscopy in the acute phase
E. Acute Appendicitis
Early appendicitis or atypical presentations (pelvic appendix, retrocaecal) can cause diarrhoea as a predominant symptom alongside RIF pain and fever.
To rule out:
- CT abdomen (non-compressible appendix >6mm, periappendiceal fat stranding)
- USS (especially in children and pregnant women)
- Alvarado/MANTRELS score
F. Food Allergy / Intolerance
Lactase deficiency, fructose intolerance, or allergic reactions can produce acute watery diarrhoea (osmotic gap positive). Onset closely follows specific food intake.
To rule out:
- Dietary history; resolution on elimination
- Stool osmotic gap >125 mOsmol/kg suggests osmotic diarrhoea
- Lactose breath test
G. Toxic Ingestion / Poisoning
Heavy metal poisoning (arsenic, mercury), mushroom toxins, organophosphates can cause acute diarrhoea with systemic features.
To rule out:
- Detailed exposure history
- Urine/blood heavy metal levels
- Toxicology screen
H. Other Conditions Mimicking Acute Diarrhoea
| Condition | Distinguishing Feature | Investigation |
|---|---|---|
| Partial bowel obstruction | Colicky pain, distension; "overflow diarrhoea" around impaction | Plain AXR (air-fluid levels); CT |
| Pelvic inflammatory disease | Lower abdominal pain + vaginal discharge; altered bowel habit | Pelvic USS; cervical swabs |
| Graft-vs-host disease | Post-bone marrow transplant; bloody diarrhoea | Sigmoidoscopy + biopsy |
| Runner's diarrhoea | Marathon/endurance athletes; exercise-induced | Exercise history; exclusion of other causes |
Key Distinguishing Clinical Features at a Glance
| Feature | Suggests |
|---|---|
| Onset within 1-6 h of eating | Preformed toxin (S. aureus, B. cereus emetic) |
| Onset 8-16 h after eating | C. perfringens, B. cereus diarrhoeal type |
| Travel to developing world | ETEC, Campylobacter, Shigella, Giardia, E. histolytica |
| Watery, no fever, no blood | Viral (norovirus), ETEC, osmotic/drug causes |
| Bloody + high fever + tenesmus | Shigella, Campylobacter, EHEC (no fever), E. histolytica |
| Bloody diarrhoea WITHOUT fever | EHEC O157:H7 (HUS risk) |
| Recent antibiotics/hospitalisation | C. difficile |
| Foul greasy stools, bloating, no fever | Giardia |
| HIV/immunocompromised | CMV, Cryptosporidium, Microsporidia, Mycobacterium, Isospora |
| Elderly + LIF pain + fever | Diverticulitis, ischemic colitis |
| Post-antibiotic + hyperleukocytosis | C. difficile (check WBC >15,000 as alarm sign) |
| RIF pain + fever | Yersinia (mimics appendicitis), Crohn's, appendicitis |
| Associated with seafood (raw) | Vibrio parahaemolyticus, hepatitis A, Salmonella |
Indications for Stool Microbiological Workup
Per Harrison's 22E, evaluate (stool studies, bloods, possibly imaging) when:
- Profuse diarrhoea with dehydration
- Overtly bloody stools
- Fever ≥38.5°C
- Duration >48 h without improvement
- Recent antibiotic use
- New community outbreak
- Severe abdominal pain in patients >50 years
- Elderly (≥70 years) or immunocompromised patients
Sources
- Harrison's Principles of Internal Medicine 22E (2025), Chapter 49
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Box 16.3 and Chapter 16
- Goldman-Cecil Medicine International Edition, Chapter 126
- The Washington Manual of Medical Therapeutics, Chapter on GI emergencies
This is a shared conversation. Sign in to Orris to start your own chat.