Open cholecystectomy operative notes
Reading File
Finding Sources
Searching the Web
open cholecystectomy operative notes template procedure steps
Reading File
Reading File
Reading Web Page
https://www.mtsamples.com/site/pages/sample.asp?Type=85-Surg…
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive textbook content from multiple authoritative surgical sources. Here is the full operative note for open cholecystectomy:
Open Cholecystectomy - Operative Notes
Preoperative Preparation
- Full blood count, renal and liver function tests, prothrombin time
- Coagulation screen; chest X-ray and ECG if clinically indicated
- DVT prophylaxis: subcutaneous heparin + antiembolic stockings
- Antibiotic prophylaxis: second-generation cephalosporin (e.g., cefuroxime) administered within 30 minutes of skin incision
- Informed consent obtained; risks, benefits, and alternatives (including laparoscopic approach) discussed with the patient
- Bladder emptied preoperatively (urinary catheterization generally not required)
- Orogastric tube placed if stomach is distended; removed at end of operation
- US-guided subcostal transversus abdominis plane (TAP) block may be considered for postoperative pain reduction
- Sequential compression devices to lower extremities
Patient Positioning
- Supine, arms abducted and supported on arm boards
- Fluoroscopy-compatible operating table (in case intraoperative cholangiogram is needed)
- Arm tucked on right side if cholangiogram is planned, to allow C-arm maneuvering
Incision
- Kocher (right subcostal) incision is the preferred approach - oblique, 2.5-5 cm inferior to and parallel to the right subcostal margin; extends from xiphoid laterally as needed to accommodate the working hand
- Carried through subcutaneous fat, external oblique, internal oblique, transversus abdominis, and peritoneum
- Alternative: Upper midline incision through skin, subcutaneous fat, and linea alba - preferred in emergencies or when wider abdominal access may be required
(Fischer's Mastery of Surgery, 8th ed.)
Abdominal Exploration & Exposure
- On entry, inspect the right upper quadrant for additional pathology
- A hand is swept over the right lobe of the liver to allow air to enter the subphrenic space
- Lap pads packed:
- Posterolaterally to right lobe of liver (to deliver gallbladder into the wound)
- Inferiorly to displace the hepatic flexure of the colon
- To the left to displace the stomach from the field
- Costal margin retracted - a fixed mechanical retractor (e.g., Thompson or Balfour) is used to free the assistant's hands
- Retractors placed over the superior liver edge and gastroduodenal area to put the triangle of Calot on stretch
(Fischer's Mastery of Surgery, 8th ed.; Maingot's Abdominal Operations)
Gallbladder Decompression (if tense/acutely inflamed)
- A trocar inserted through the center of a 3-0 PDS purse-string suture placed at the fundus
- Gallbladder contents aspirated; trocar withdrawn and purse-string tied
- Alternatively, a large-gauge needle + syringe can decompress the fundus; puncture site closed with a PDS stitch and used as a handle for traction
- Presence of clear thick fluid = long-standing cystic duct obstruction
(Fischer's Mastery of Surgery, 8th ed.)
Dissection of the Triangle of Calot
- Retraction: A Kelly clamp is placed on the fundus (retracted cranially), and a second clamp is placed on Hartmann's pouch (retracted laterally and inferiorly) - this opens the triangle of Calot
- Adhesiolysis: Adhesions between the gallbladder and omentum, duodenum, or transverse colon are divided with electrocautery or sharp dissection. A small moist swab is placed in the subhepatic space behind the gallbladder to prevent bile/stone spillage
- Peritoneal incision: The peritoneum overlying the cystic duct and artery is opened, staying close to the gallbladder
- Identify structures in Calot's triangle:
- Cystic artery: identified running within the triangle; Lund's node sits superficial to the artery and is a reliable landmark. The artery is skeletonized using right-angle dissection and electrocautery
- Cystic duct: cleared of peritoneum and surrounding fat; its junction with the common bile duct (CBD) is identified; dissection confirms only two structures enter the gallbladder (critical view of safety equivalent)
- The surgeon introduces the left index finger into the foramen of Winslow and palpates the CBD for calculi
(Maingot's Abdominal Operations; Fischer's Mastery of Surgery, 8th ed.)
Ligation and Division
- Cystic artery: Ligated and divided near the surface of the gallbladder (reduces bleeding during liver bed dissection). Double ligation is standard (two 2-0 silk or absorbable ties or clips)
- Cystic duct: A clip or 2-0 suture tie is placed proximally (close to the gallbladder); the duct is divided distally. Ligation does NOT need to be flush with the CBD. Cystic duct stump length is not a critical factor in postcholecystectomy syndrome
- Caution: Short cystic duct - close dissection + high ligation near the gallbladder to avoid CBD injury; short cystic artery - identify the right hepatic artery first
(Maingot's Abdominal Operations; Bailey and Love's, 28th ed.)
Intraoperative Cholangiogram (Selective or Routine)
- Indicated to clarify biliary anatomy, identify injuries, or detect CBD stones
- A small incision is made in the anterior surface of the cystic duct 1-2 cm from its junction with the CBD; a cholangiogram catheter is passed in and secured with a clip or balloon
- Half-strength iodinated contrast is injected under live fluoroscopy
- Complete study shows: right and left hepatic ducts, common hepatic duct, CBD, cystic duct junction, and flow into the duodenum
- CBD stones = filling defects; strictures = ductal narrowing
- Glucagon (1 mg IV) or cholecystokinin may be given to relax the sphincter of Oddi if contrast does not flow freely
(Fischer's Mastery of Surgery, 8th ed.)
Gallbladder Dissection from the Liver Bed
Antegrade (fundus-down) Approach - Standard
- After securing the cystic duct and artery, dissect the gallbladder off the liver bed from the fundus downward
- Enter the submucosal plane (superficial to small vessels) - avoids injury to the liver and branches of the middle hepatic vein or intrahepatic ductules
- Incise the peritoneum with electrocautery using a right-angle clamp; displace the gallbladder side to side to expose and incise attachments
- Continue downward until the peritoneal incision over the gallbladder is continuous with the dissection made previously in Calot's triangle
- In a diseased/fibrotic gallbladder: avoid the cystic plate - dissection deep to it risks injury to the right portal pedicle, right hepatic duct, and right hepatic artery
- Avoid excessive unipolar diathermy close to the common hepatic duct (diathermy current can conduct through remaining gallbladder attachments)
Retrograde (fundus-first / top-down) Approach
- Used when acute inflammation or chronic scarring makes approaching the infundibulum first difficult
- Gallbladder is dissected from the liver before dissecting within the triangle of Calot
- A finger can be inserted into the gallbladder lumen to guide dissection when tissue planes are not apparent
- Cystic duct and artery then ligated as above
(Fischer's Mastery of Surgery, 8th ed.; Maingot's Abdominal Operations)
Gallbladder Removal & Hemostasis
- Gallbladder removed from the operative field and sent for histopathology
- Gallbladder bed hemostasis with electrocautery
- Persistent hemorrhage: oxidized regenerated cellulose (Surgicel), TachoSil, or EVARREST fibrin sealant patch
- Portal structures re-examined - cystic duct stump inspected
- Subhepatic space irrigated with warm saline; all irrigant evacuated
- Specimen bag used if bile/stone spillage occurred; retrieve any spilled stones
(Fischer's Mastery of Surgery, 8th ed.)
Drain Placement
- Drains are not mandatory - placed only if the surgeon is concerned about possible bile leak
- If placed: closed suction drain (e.g., Blake or Jackson-Pratt) in the subhepatic space/Morrison's pouch
Special Situations
| Situation | Management |
|---|---|
| Severe inflammation obliterating planes | Consider subtotal cholecystectomy - leave a portion of the infundibulum in situ, remove all stones, suture-ligate mucosal side of cystic duct origin |
| Unintentional gallbladder puncture | Apply second clamp or purse-string suture to prevent bile/stone spillage |
| Mirizzi's syndrome / cholecystoenteric fistula | High risk for bile duct injury; consider expert referral |
| Short cystic artery | Identify right hepatic artery before ligation |
| CBD stones found on cholangiogram | Proceed to CBD exploration (transcystic or choledochotomy) |
Closure
- Subhepatic space re-inspected; all swabs/packs counted and confirmed retrieved
- Incision closed in one or two layers using mass closure technique (loop PDS or nylon for fascial layer)
- Skin closed with sutures or staples
- Subcutaneous layer closed if significant fat depth
Postoperative Notes
- Antibiotic course continued per unit protocol (usually single-dose prophylaxis is sufficient)
- Resume DVT prophylaxis postoperatively
- Expect 2-3 day hospital stay (vs. same-day for uncomplicated laparoscopic)
- Wound inspection at 5-7 days
- Histopathology result followed up
Sources:
- Fischer's Mastery of Surgery, 8th ed., Chapters 164 & 286
- Maingot's Abdominal Operations
- Bailey and Love's Short Practice of Surgery, 28th ed.
- Schwartz's Principles of Surgery, 11th ed.
Hydrocorle jabolouys procedure operative notes
Reading File
Finding Sources
Searching the Web
Jaboulay procedure hydrocele operative notes eversion tunica vaginalis
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading Web Page
https://www.pawanlal.org/home/index.php/diseases-and-surgeri…
Reading File
Loading Image
Loading Image
I now have comprehensive textbook content from Bailey & Love, Campbell-Walsh Wein Urology, and Fischer's Mastery. Here is the full operative note:
Hydrocele - Jaboulay's Procedure (Eversion of the Tunica Vaginalis)
Background
A hydrocele is an abnormal collection of serous fluid between the parietal and visceral layers of the tunica vaginalis. The Jaboulay procedure (also called the Winkelman technique) is an eversion/excisional technique - the gold standard for large, chronic, thick-walled, or multiloculated hydroceles where Lord's plication would be insufficient.
Three main surgical options for hydrocele:
| Technique | Indication | Principle |
|---|---|---|
| Lord's plication | Small, thin-walled sac | Plicate sac with radial sutures - no excision |
| Jaboulay's procedure | Large, chronic, thick-walled sac | Excise portion of sac + evert behind testis |
| Bottleneck procedure | Large sacs | Trim to 2-cm rim, leave sac open |
Preoperative Preparation
- Confirm diagnosis clinically: painless scrotal swelling, transilluminates, get above the swelling (distinguishes from hernia), testis palpable separately
- Scrotal ultrasound to exclude secondary hydrocele (tumor, epididymo-orchitis, trauma)
- Do NOT aspirate if malignancy is suspected (risk of malignant needle-track implantation)
- Routine bloods, clotting screen
- Mark the correct side
- DVT prophylaxis per patient risk
- Prophylactic antibiotics: single dose of a broad-spectrum antibiotic at induction
- Consent: discuss risk of hematoma (most common), infection, recurrence, injury to vas deferens/testicular vessels, chronic pain, subfertility
Anaesthesia
- General anaesthesia (GA) is standard
- Alternatively: spinal/regional anaesthesia or local anaesthesia with spermatic cord block
- Spermatic cord block reduces postoperative pain
Patient Positioning
- Supine
- Legs slightly apart
- Genitalia and perineum prepared with antiseptic and draped
Incision
- Transverse scrotal incision (preferred): placed directly over the hydrocele in the anterior scrotum, approximately 5-7 cm in length
- Alternatively: vertical midline (median raphe) incision
- The incision is deepened through skin, dartos muscle, and external spermatic fascia layer by layer
Delivery of the Hydrocele Sac
- Skin, dartos, and fascial layers incised in turn down to the parietal layer of the tunica vaginalis
- The hydrocele sac is mobilised bluntly from the surrounding scrotal tissues by sweeping the fascial layers off the tunica vaginalis
- Haemostasis secured at each layer
- The hydrocele sac is delivered through the incision intact - care taken not to rupture the sac at this stage
- If the sac is very tense, preliminary aspiration of fluid with a needle can decompress it to aid delivery
Opening the Sac
- The tunica vaginalis (parietal layer) is incised along its anterior surface with scissors or scalpel
- The hydrocele fluid is evacuated (straw-coloured/amber fluid in primary hydroceles; turbid or bloodstained fluid suggests secondary cause - send for cytology/culture if indicated)
- The testis, epididymis, and cord are inspected carefully - note any abnormality such as epididymal cysts, thickening, or testicular irregularity. Send any suspicious tissue for biopsy.
The Jaboulay Eversion (Key Step)
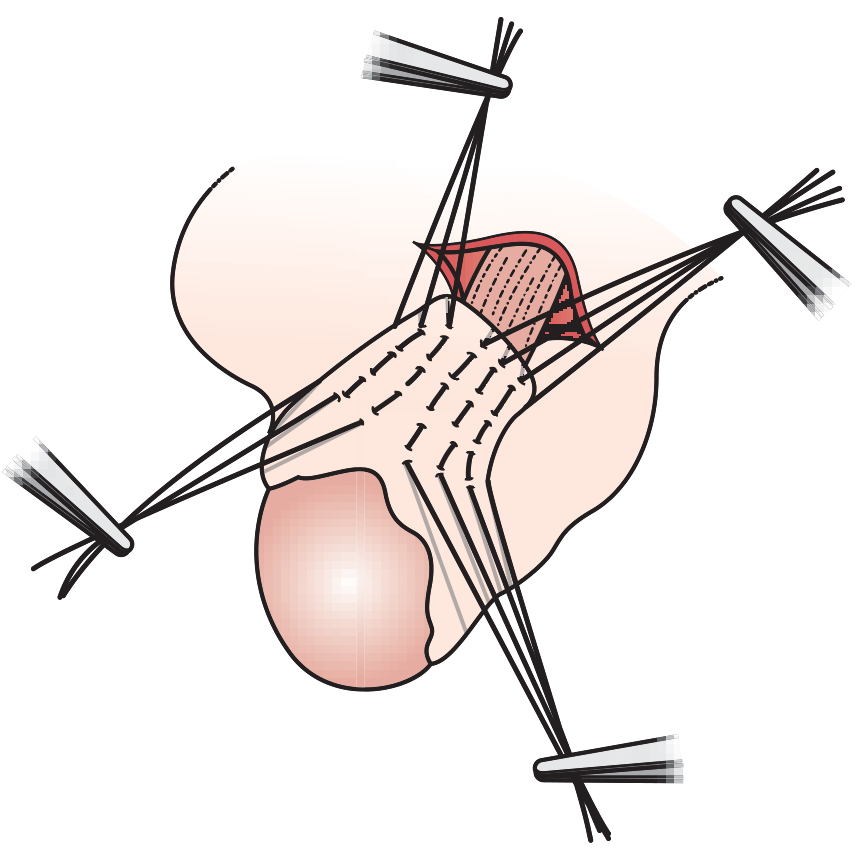
- The cut edges of the tunica vaginalis are held with Allis clamps or haemostats
- A portion of the parietal tunica vaginalis is excised - the amount excised is sufficient to allow easy eversion without leaving excessive redundant tissue behind the testis
- The remaining parietal layer is everted (turned inside-out) behind the testis and epididymis - the raw (mesothelial) surface now faces outward, away from the testis
- The testis is placed into a dartos pouch created by blunt dissection in the fascial planes of the scrotum - this holds the testis in position
- The opposing edges of the everted tunica are approximated with interrupted or continuous absorbable sutures (3-0 chromic catgut or Vicryl) behind the cord, taking care not to compress the spermatic cord (Fig. 86.10b)
- Alternatively: the cut edges of the tunica are oversewn with a running 3-0 chromic suture to achieve haemostasis from the cut edge - this is important, as bleeding from the raw cut edge is the main cause of postoperative haematoma
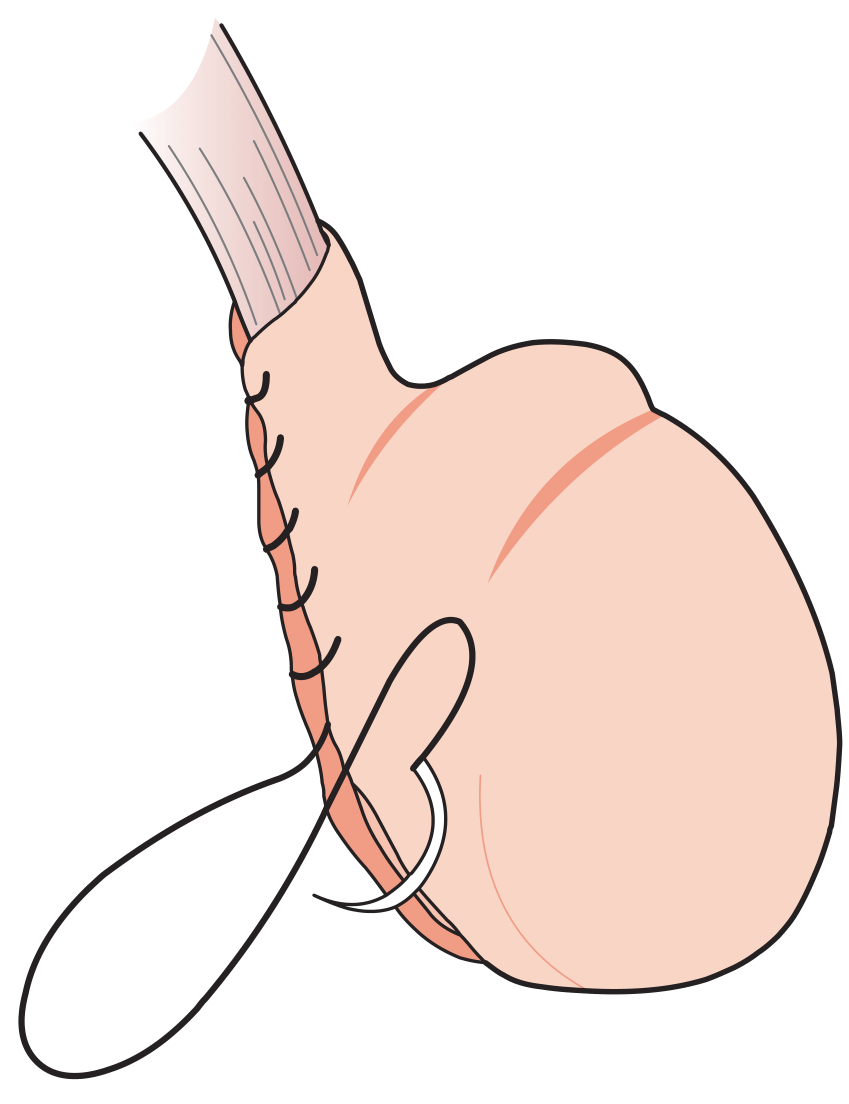
Jaboulay's procedure: the hydrocele sac is everted and the cut edges oversewn/anchored with sutures behind the testis and cord - Bailey & Love's, 28th ed.
Lord's plication (for comparison): interrupted absorbable sutures plicate the redundant tunica - Bailey & Love's, 28th ed.
Haemostasis
- Meticulous haemostasis of the cut tunical edges is essential - haematoma is the most common postoperative complication
- Bleeding points on the cut edge are controlled with bipolar diathermy
- The cut edge is oversewn with a continuous absorbable suture if bleeding persists
Drain Placement
- A small corrugated or closed-suction drain may be placed in the scrotal cavity and brought out through a separate stab incision
- Drain is not mandatory in all cases; reserved for cases with significant ooze or large dead space
Testicular Replacement & Closure
- The testis (now with the everted, sutured tunica around it) is placed back into the scrotum in a natural position
- Fascial layers closed with absorbable sutures (2-0 Vicryl)
- Dartos layer closed with interrupted absorbable sutures (2-0 or 3-0 Vicryl)
- Skin closed with subcuticular absorbable sutures (3-0 Vicryl Rapide or Monocryl) or interrupted mattress sutures
- Firm supportive scrotal dressing applied - fluffed gauze within a scrotal support (jockstrap)
Postoperative Care
- Adequate analgesia (NSAIDs + paracetamol; opioids rarely needed)
- Scrotal support worn for 2-4 weeks to reduce oedema and discomfort
- Drain removed at 24-48 hours if placed
- Ice packs to the scrotum for the first 24-48 hours
- Avoid strenuous activity and sexual intercourse for 2-4 weeks
- Wound review at 1-2 weeks
- Advise patient to report: increasing pain, swelling, fever (suggests haematoma or infection)
Complications
| Complication | Notes |
|---|---|
| Haematoma (most common) | Due to bleeding from cut tunical edges; usually resorbs spontaneously; may need surgical evacuation |
| Wound infection | Uncommon; treat with antibiotics |
| Recurrence | Low with Jaboulay (lower than aspiration alone; higher with plication vs. excision) |
| Injury to vas deferens | Avoided by careful identification |
| Injury to testicular vessels | Can cause testicular atrophy |
| Chronic scrotal pain | Rare; usually resolves with time |
Key Anatomical Points
- Triangle of Calot equivalent: In the scrotal approach, identify the epididymis and cord before applying any ties
- The spermatic cord must not be compressed by the everted tunical suture line
- The right hepatic artery equivalent here is the testicular artery - identify and preserve it throughout
- Secondary hydrocele: always inspect the testis and epididymis - a firm testicular nodule needs urgent biopsy
Sources:
- Bailey and Love's Short Practice of Surgery, 28th ed., Chapter 86
- Campbell-Walsh-Wein Urology, Chapter 83 (Hydrocelectomy)
This is a shared conversation. Sign in to Orris to start your own chat.