Explain Hepatitis C under proper headings
Reading File
Finding Sources
Searching PubMed
"hepatitis C" treatment
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Excellent - I now have comprehensive data from multiple authoritative textbooks. Let me compile the full, well-structured response.
Hepatitis C
1. Overview
Hepatitis C is a blood-borne infectious disease caused by the Hepatitis C virus (HCV), a member of the Flaviviridae family. It is one of the leading causes of chronic liver disease worldwide, affecting approximately 170 million individuals globally. The disease is characterized by a high rate of chronicity - approximately 80-90% of infected persons develop persistent infection - and a significant long-term risk of cirrhosis and hepatocellular carcinoma (HCC). With the advent of direct-acting antivirals (DAAs), over 95% of infections are now curable.
- Robbins & Kumar Basic Pathology, p. 602
- Henry's Clinical Diagnosis and Management by Laboratory Methods
2. The Virus
Structure
HCV is an enveloped, positive-sense, single-stranded RNA virus with a genome approximately 9.6 kilobases in length. The genome contains:
- Highly conserved 5' and 3' untranslated regions (UTRs)
- A single large open reading frame (ORF) encoding a polyprotein of ~3000 amino acids
The polyprotein is cleaved by cellular and viral proteases into 10 functional proteins:
- Structural proteins: Core protein (nucleocapsid), E1 and E2 (envelope glycoproteins)
- Non-structural proteins: p7 (viroporin), NS2 (metalloproteinase), NS3 (serine protease + RNA helicase), NS4A (NS3 cofactor), NS4B (membranous web formation), NS5A (essential for virion assembly; also an interferon-resistance protein), NS5B (RNA-dependent RNA polymerase)
Genotypes
Due to the high mutation rate of NS5B RNA polymerase (which lacks proofreading), HCV has evolved into 7 major genotypes (1-7) and multiple subtypes. Clinically important facts:
- Genotype 1a: Most common in North America
- Genotype 1b: Predominates in Europe; associated with fibrosing cholestatic hepatitis post-transplant
- Genotypes 4 and 5: Unique to Africa
- Genotypes 1 and 4: More resistant to interferon-based therapy (required 48 weeks vs. 24 weeks for genotypes 2/3)
Patients typically harbor a heterogeneous population of closely related variants called quasispecies, which contributes to immune evasion and chronicity.
- Yamada's Textbook of Gastroenterology, p. 1885-1886
- Henry's Clinical Diagnosis and Management by Laboratory Methods
3. Life Cycle
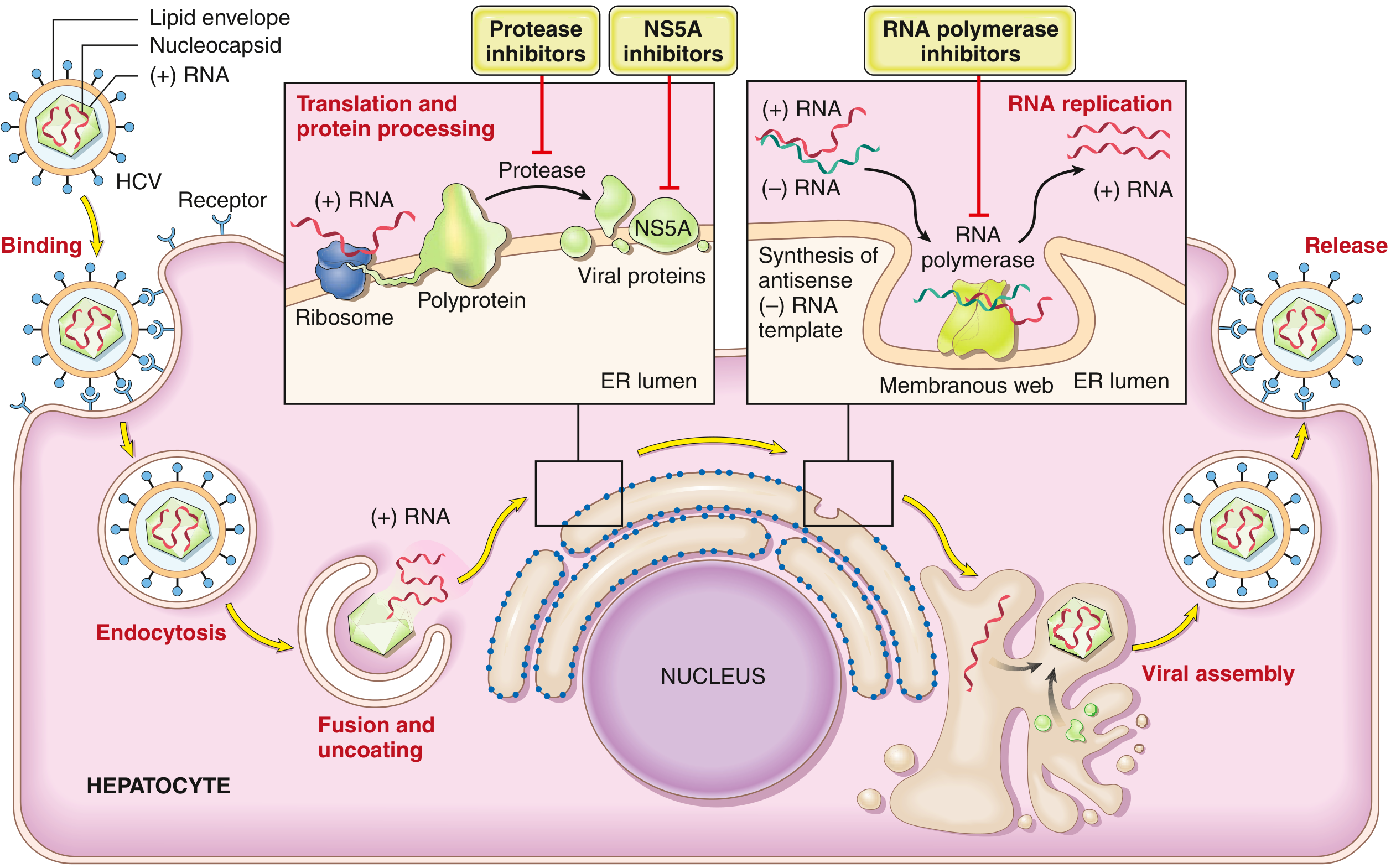
- Binding: HCV attaches to multiple hepatocyte surface receptors - CD81, claudin-1, scavenger receptor SR-B1, LDL receptor, and occludin
- Endocytosis and fusion: Followed by uncoating and release of viral genome into the cytoplasm
- Translation: The 5' internal ribosomal entry site (IRES) directs ribosomal translation of the polyprotein in the rough endoplasmic reticulum
- Replication: NS5B RNA polymerase synthesizes a negative-strand RNA intermediate within ER-derived "membranous web" double-membrane vesicles, which then serves as template for new positive-strand genomes
- Assembly: Core protein interacts with viral genomes at lipid droplets; E1/E2 envelope glycoproteins are incorporated with help of ApoE/B lipoprotein metabolism
- Release: Mature virions are released from the hepatocyte
- Yamada's Textbook of Gastroenterology, p. 1886
- Robbins & Kumar Basic Pathology, p. 603
4. Epidemiology and Transmission
Global Burden
- ~170 million individuals affected worldwide
- ~2.7 million Americans with chronic HCV infection
- Annual new infections in the US dropped from >230,000 (mid-1980s peak) to ~17,000 - largely due to blood supply screening
- Recent resurgence linked to the opioid epidemic and injection drug use
Routes of Transmission
| Route | Notes |
|---|---|
| Intravenous drug use | Leading cause of new infections |
| Needlestick injury | Risk ~1.8% per exposure (6x higher than HIV) |
| Blood transfusion | Risk now near zero in the US due to screening |
| Perinatal | ~5-6% in infants of HCV-infected mothers |
| Sexual intercourse | Low efficiency of transmission |
| Household contact | Low risk |
| Unknown | ~1/3 of cases have no identifiable risk factor |
- Robbins & Kumar Basic Pathology, p. 601-602
5. Pathogenesis
HCV primarily infects hepatocytes. Liver damage is believed to result largely from the host immune response rather than direct cytopathic effect:
-
HCV-specific CD8+ cytotoxic T lymphocytes (CTLs) attack infected hepatocytes
-
NS5A protein resists interferon signaling, aiding immune evasion
-
The virus generates quasispecies variants that escape neutralizing antibodies, explaining why 90% of patients with chronic infection have detectable HCV RNA despite the presence of antibody
-
Factors that accelerate fibrosis progression include: older age, male gender, alcohol use, immunosuppression, HBV/HIV coinfection, obesity, type 2 diabetes, metabolic syndrome, and insulin resistance
-
Robbins & Kumar Basic Pathology, p. 602-603
6. Clinical Features
Incubation Period
4 to 26 weeks (mean ~9 weeks).
Acute Hepatitis C
- ~85% of acute infections are asymptomatic and go unrecognized
- When symptomatic (20-30%): jaundice, anorexia, malaise, nausea, right upper quadrant pain, fatigue
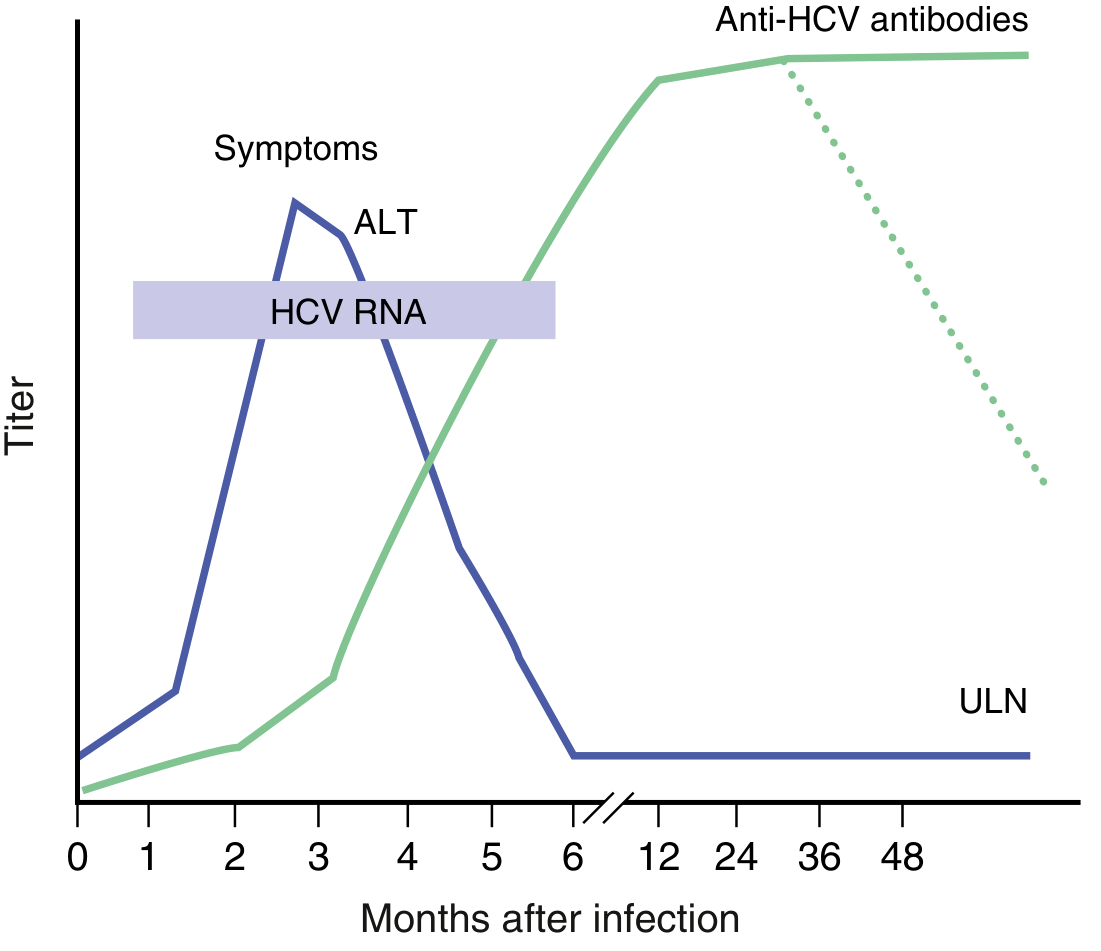
- HCV RNA detectable in blood within 1-3 weeks of infection, coinciding with elevated serum transaminases (ALT/AST)
- Severe acute hepatitis is rare
- Spontaneous clearance occurs in only ~10-20% of cases
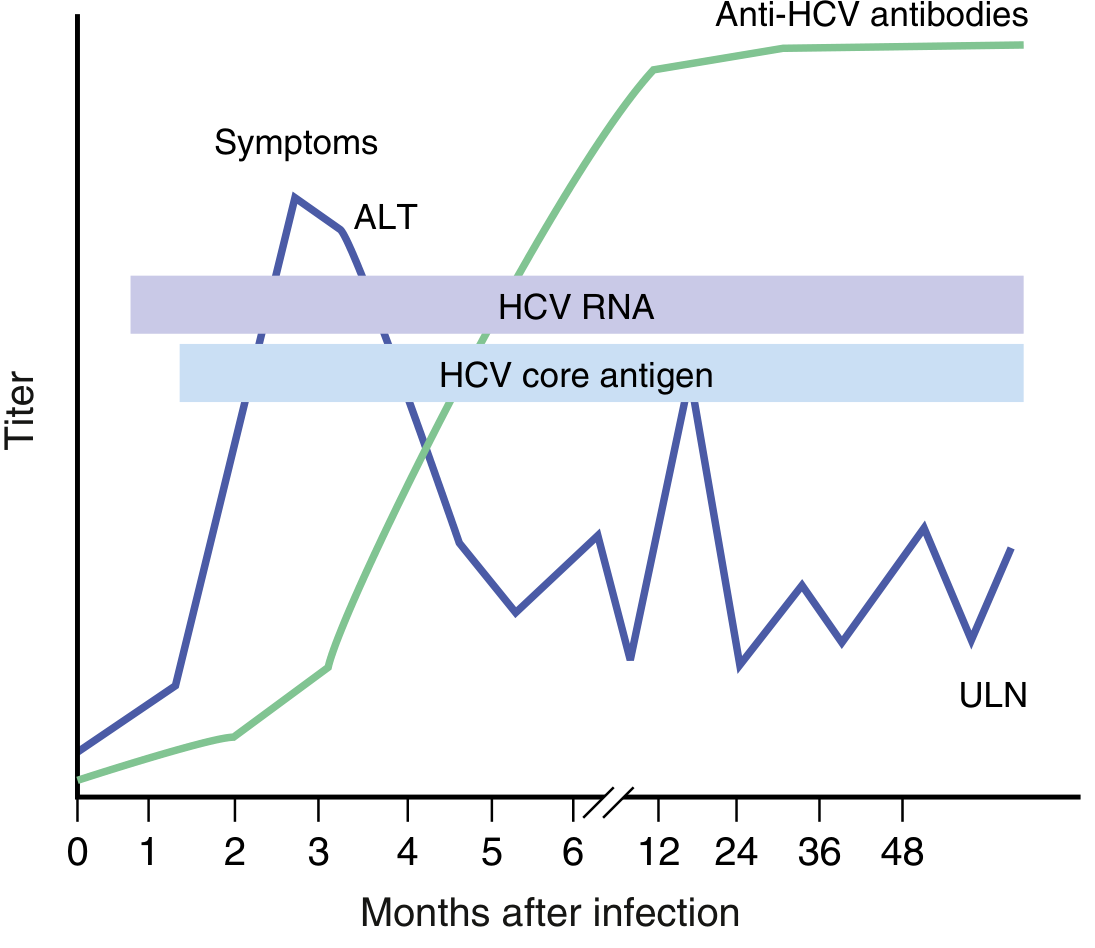
Chronic Hepatitis C
- Chronicity in 80-90% of infected individuals
- A characteristic feature is episodic elevations in serum aminotransferase separated by periods of normal enzyme levels
- Even patients with normal transaminases may sustain progressive liver damage and need treatment
- Cirrhosis develops in approximately 20% over 20-30 years
- Those with cirrhosis are at significant risk of hepatocellular carcinoma (HCC) - HCV accounts for ~1/3 of liver cancer cases in the US
Extrahepatic Manifestations
HCV has associations beyond the liver, including:
-
Mixed cryoglobulinemia (vasculitis, purpura, arthralgia, glomerulonephritis)
-
Membranoproliferative glomerulonephritis
-
Porphyria cutanea tarda
-
Lichen planus
-
B-cell non-Hodgkin lymphoma
-
Thyroid disease
-
Robbins & Kumar Basic Pathology, p. 602-603
-
Jawetz Melnick & Adelberg's Medical Microbiology 28E, p. 524-525
7. Diagnosis
Serological Testing
- Anti-HCV antibodies (3rd-generation ELISA): Detectable in 50-70% at symptom onset; in others, antibody appearance delayed 3-6 weeks. Antibodies target core, envelope, and NS3/NS4 proteins. Does not distinguish acute from chronic or resolved infection.
- In high-risk populations: positive predictive value >99%
- In low-risk populations (e.g., blood donors): positive predictive value only ~25%
Nucleic Acid Testing (NAT)
- Qualitative HCV RNA PCR: Confirms active viremia; positive within 1-2 weeks of infection (earlier than antibodies). Used to confirm active infection.
- Quantitative HCV RNA: Measures viral load (IU/mL by WHO standard); used to monitor treatment response. Real-time PCR has a detection range of 5 to 200 million IU/mL.
- HCV RNA is the primary test for confirming persistent infection in chronic hepatitis C
- As many as 15% of those with acute HCV infection can have transiently negative HCV RNA
Genotyping
- Nucleic acid-based assays used to genotype HCV
- Genotyping guides treatment regimen selection and duration
Liver Assessment
-
Liver biopsy or non-invasive fibrosis scores (FIB-4, APRI) to stage fibrosis
-
Elevated ALT/AST, with fluctuating pattern in chronic disease
-
Henry's Clinical Diagnosis and Management by Laboratory Methods, p. 1545-1589
-
Jawetz Melnick & Adelberg's Medical Microbiology 28E, p. 524
8. Treatment
Direct-Acting Antivirals (DAAs)
The treatment of HCV was revolutionized by DAAs, modeled after HIV combination therapy. These drugs target specific steps in the viral lifecycle:
| Drug Class | Target | Examples |
|---|---|---|
| NS3/4A Protease Inhibitors | Cleave viral polyprotein | Simeprevir, Grazoprevir, Glecaprevir, Voxilaprevir |
| NS5A Inhibitors | Block virion assembly and replication | Ledipasvir, Daclatasvir, Elbasvir, Pibrentasvir, Velpatasvir |
| NS5B Polymerase Inhibitors | Block RNA replication | Sofosbuvir (nucleotide), Dasabuvir (non-nucleoside) |
Key combination regimens:
- Sofosbuvir/Velpatasvir (Epclusa) - pan-genotypic, once daily
- Glecaprevir/Pibrentasvir (Mavyret) - pan-genotypic, 8 weeks for treatment-naive non-cirrhotic
- Ledipasvir/Sofosbuvir (Harvoni) - genotypes 1, 4, 5, 6
Treatment Goal
Sustained Virologic Response (SVR): Undetectable HCV RNA 12 weeks after completing therapy. SVR is considered a cure. Currently, over 95% of HCV infections are curable.
Older Therapies (Largely Obsolete)
- Pegylated Interferon (PEG-IFN) + Ribavirin: The former standard of care. Major side effects included flu-like symptoms, depression, hemolytic anemia, neutropenia, thrombocytopenia, and significant teratogenicity. Ribavirin carries a black box warning for hemolytic anemia. These are no longer first-line.
Post-Liver Transplant Treatment
-
Recurrent HCV post-transplant was a major concern leading to accelerated graft fibrosis
-
DAA-based, interferon-free regimens have transformed outcomes in this population
-
SVR after transplant prevents graft cirrhosis and markedly improves outcomes
-
Fibrosing cholestatic hepatitis (FCH), a rare but severe form of recurrence (5-10% in some series), requires prompt reduction of immunosuppression plus antiviral therapy
-
Henry's Clinical Diagnosis and Management by Laboratory Methods, p. 1548-1552
-
Robbins & Kumar Basic Pathology, p. 603
-
Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 1886
9. Prevention
No Vaccine Available
Unlike Hepatitis A and B, there is currently no approved vaccine for HCV. Barriers include:
- High mutation rate and quasispecies diversity
- Limited understanding of protective immunity
- Failure of neutralizing antibodies to prevent re-infection
Several vaccine candidates have reached human trials (recombinant adenoviral NS-region vaccine, recombinant E1/E2 glycoprotein vaccine, prime-boost chimpanzee adenovirus approach), but none have demonstrated sufficient efficacy to gain approval.
Post-Exposure Prophylaxis
- Immunoglobulin is NOT recommended for HCV post-exposure prophylaxis - evidence is insufficient
- No antiviral post-exposure regimen is currently approved
Preventive Measures
-
Screening of blood supply (has nearly eliminated transfusion-related HCV)
-
Universal precautions for healthcare workers
-
Harm reduction programs for injection drug users (needle exchange, opioid substitution therapy)
-
Testing and treatment of infected individuals ("treatment as prevention")
-
Yamada's Textbook of Gastroenterology, p. 1415-1422
10. Complications and Prognosis
| Complication | Approximate Risk |
|---|---|
| Chronic infection | 80-90% of acute cases |
| Cirrhosis (20-30 years) | ~20% of chronic cases |
| Hepatocellular carcinoma | Risk primarily in cirrhotic patients; HCV accounts for ~1/3 of liver cancer in the US |
| Liver failure / liver transplantation | Subset of cirrhotic patients |
Factors that accelerate progression to cirrhosis include: alcohol use, male gender, older age at infection, HIV/HBV co-infection, metabolic syndrome, and immunosuppression.
With effective DAA treatment achieving SVR, disease progression halts, fibrosis can partially reverse, and the risk of HCC significantly decreases - though patients with established cirrhosis still require ongoing HCC surveillance.
- Robbins & Kumar Basic Pathology, p. 602-603
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 1885-1886
Recent evidence note: A 2024 systematic review and meta-analysis (PMID 39361017) examined drug resistance-associated substitutions after pan-genotypic DAA failure, confirming that resistance remains uncommon with first-line regimens but is a consideration in re-treatment settings.
Now generate by referring standard medicine textbooks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Reading File
Hepatitis C
Sources: Harrison's Principles of Internal Medicine 22E (2025) | Goldman-Cecil Medicine, International Edition
1. Definition and the Pathogen
Hepatitis C is an infectious liver disease caused by the Hepatitis C virus (HCV), a member of the Flaviviridae family, genus Hepacivirus. The genome is a single-stranded, positive-sense, linear RNA molecule. Key structural features include:
- A 5' internal ribosome entry site (IRES) that mediates polyprotein translation
- A single open reading frame encoding a polyprotein of ~3000 amino acids
- A short 3' noncoding region involved in replication
- The RNA genome is encased in a protein core (nucleocapsid), surrounded by a lipid bilayer envelope containing two inserted viral glycoproteins (E1, E2) that mediate hepatocyte entry
The polyprotein is cleaved into 10 functional proteins by cellular and viral proteases:
- Structural: Core, E1, E2 (envelope glycoproteins), p7 (viroporin)
- Non-structural: NS2 (metalloproteinase), NS3 (serine protease + RNA helicase), NS4A (NS3 cofactor), NS4B (membranous web formation), NS5A (virion assembly; IFN-resistance), NS5B (RNA-dependent RNA polymerase - the replication engine)
Because of the low fidelity of NS5B polymerase (no proofreading), HCV mutates rapidly, generating 7 major genotypes (1-7) and closely related intrahost variants called quasispecies. This genetic plasticity allows the virus to evade immune responses and is the primary reason no vaccine yet exists.
Goldman-Cecil Medicine, Ch. 134
2. Epidemiology
Global Burden
- An estimated 8 million individuals are chronically infected worldwide (Goldman-Cecil)
- HCV causes approximately 290,000 deaths per year globally
- In the United States, ~2.4 million individuals are chronically infected (prevalence ~0.7%)
- HCV still causes more deaths in the US than HIV, largely because most cases remain undiagnosed
Geographic Prevalence
| Region | Estimated Prevalence |
|---|---|
| United States | ~0.7% |
| Europe | ~1.3% |
| Southeast Asia | ~0.5% |
| Africa | ~0.9% |
| Egypt | ~9% overall (up to 40% in rural areas) - highest worldwide |
Egypt's extraordinary prevalence resulted from mass intramuscular injection campaigns for schistosomiasis treatment in the 1950s-1960s.
Routes of Transmission
HCV is transmitted almost exclusively through infected blood. In industrialized countries, the principal route is now injection drug use, accounting for 60-80% of new cases (incidence as high as 39 per 100 person-years in people who inject drugs).
| Route | Notes |
|---|---|
| Injection drug use | Leading cause in high-income countries; imprisonment is a key risk factor |
| Blood transfusion | Theoretical risk now <1 in 2 million donations in the US; <1 in 34 million in France |
| Nosocomial | Improperly decontaminated equipment; contaminated hands/gloves of HCWs |
| Needlestick (HCW) | Risk <1%; slightly higher HCV prevalence than general population |
| Tattooing/piercing | If standard precautions not implemented |
| Sexual intercourse | Low efficiency; outbreaks reported in MSM with high-risk sexual practices |
| Perinatal | <5%; related to blood exposure at delivery; cesarean section NOT recommended routinely; breastfeeding NOT contraindicated (unless nipple lesions present) |
| Household (shared instruments) | Scissors, razors, combs |
| No identifiable risk | 10-30% of cases |
Goldman-Cecil Medicine, Ch. 134
3. Pathobiology
Viral Entry
HCV entry into hepatocytes is a coordinated, sequential process involving multiple receptor molecules:
Glycosaminoglycans → CD81 → Scavenger receptor B1 (SR-B1) → Claudin-1 → Occludin
Following receptor binding: fusion with the endosomal membrane → decapsidation → release of positive-strand RNA into the cytoplasm.
Replication
The viral genome is translated in the rough endoplasmic reticulum via the IRES. Replication occurs in ER-derived "membranous web" double-membrane vesicles, where NS5B synthesizes a negative-strand RNA intermediate, then produces new positive-strand genomes. Viral assembly begins at lipid droplets, involving ApoE/B lipoprotein metabolism.
Immune Evasion and Chronicity
HCV is not a cytopathic virus - liver injury results from the host immune response. Key mechanisms of chronicity:
- A qualitatively and quantitatively deficient CD4+ T-helper and CD8+ CTL response that fails to clear infection
- NS5A protein inhibits multiple steps of the JAK-STAT interferon signaling pathway
- Continuous generation of quasispecies variants that escape neutralizing antibodies
- Patients who spontaneously recover and maintain anti-HCV antibodies are not protected against re-infection
Fibrogenesis
Chronic necroinflammation triggers fibrogenesis through activation of hepatic stellate cells. Fibrosis progresses at non-linear rates, accelerated by: older age, male sex, chronic alcohol use, viral coinfections (HBV/HIV), immunosuppression, and metabolic factors (steatosis, insulin resistance, type 2 diabetes, obesity). Notably, the severity of chronic hepatitis is independent of HCV RNA level and genotype.
Goldman-Cecil Medicine, Ch. 135
4. Clinical Features
Acute Hepatitis C
Incubation period: 2 weeks to 6 months (mean 6-7 weeks).
- Acute HCV is most often asymptomatic and undiagnosed
- When symptomatic (minority): fatigue, anorexia, nausea, right upper quadrant discomfort, jaundice
- HCV RNA appears in serum within 1-2 weeks of infection
- ALT rises coinciding with peak viremia, then may fall
- Spontaneous clearance occurs in 20-50% of patients
Chronic Hepatitis C
Chronic infection follows acute hepatitis C in 50-85% of cases (Harrison's notes up to 85%; Goldman-Cecil notes 50-80% depending on age at acquisition).
- Most cases are identified in asymptomatic patients (found incidentally on blood donation screening, insurance testing, or routine labs)
- The most common symptom is fatigue, which may persist for years
- ALT levels are characteristically episodic - fluctuating, with periods of near-normal values even during active hepatitis. Approximately one-third of patients have persistently normal aminotransferase activity
- Even patients with normal ALT may have hepatitis and fibrosis on biopsy and remain at risk for progression
Extrahepatic Manifestations
HCV is the main cause of type II and type III mixed cryoglobulinemia:
- Low levels of circulating cryoglobulins (containing HCV RNA, anti-HCV, rheumatoid factor, low complement) found in 50-70% of chronic HCV patients
- Elevated rheumatoid factor in ~70%
- Fewer than 1% develop symptomatic cryoglobulinemic vasculitis: fatigue, myalgias, arthralgias, purpura, leukocytoclastic vasculitis, peripheral neuropathy, membranoproliferative glomerulonephritis
Other extrahepatic associations:
- Porphyria cutanea tarda
- Lichen planus
- Thyroid disorders
- B-cell non-Hodgkin lymphoma
- Diabetes mellitus (type 2)
Autoantibodies (including anti-LKM1, directed against cytochrome P450 IID6) may be found in chronic hepatitis C, occasionally causing diagnostic confusion with autoimmune hepatitis type 2.
Harrison's Principles of Internal Medicine 22E, Ch. 338; Goldman-Cecil Medicine, Ch. 135
5. Natural History and Complications
| Outcome | Approximate Frequency |
|---|---|
| Chronic infection after acute HCV | 50-85% |
| Spontaneous clearance (influenced by IL28B/IFNL3 genotype) | 15-50% |
| Cirrhosis after 20-30 years of chronic infection | ~20-25% |
| Cirrhosis prevalence in referred research cohorts | Up to 50% |
| Hepatic decompensation over 10 years | ~15% |
| Hepatocellular carcinoma (annual incidence in cirrhosis) | 1-5% per year |
| Patients remaining asymptomatic and well-compensated (20 years) | ~60% |
Host factors modifying spontaneous clearance: A single nucleotide polymorphism (SNP) on chromosome 19, IL28B (IFNL3), strongly predicts both spontaneous resolution and response to IFN-based therapy. Genotype C/C confers 53% spontaneous clearance, C/T 30%, and T/T only 23%.
Important context: Despite the significant minority who progress to cirrhosis and end-stage liver disease, the overall 10-20 year mortality in most patients with chronic HCV does not differ from a matched transfused control population without HCV. However, hepatitis C was the most frequent indication for liver transplantation in the US until recently - a position now being displaced by alcoholic liver disease and NAFLD, largely thanks to highly effective DAA therapy.
Harrison's Principles of Internal Medicine 22E, Ch. 338
6. Diagnosis
Screening Recommendations
In the United States, HCV screening is recommended once for all adults aged 18-79 years. Rapid diagnostic tests using fingerstick whole blood or saliva can improve access in resource-limited or at-risk settings.
Diagnostic Algorithm
Step 1 - Anti-HCV antibody testing (3rd-generation ELISA)
- Detects exposure (past or present); does not distinguish acute, chronic, or resolved infection
- Positive result must be confirmed with HCV RNA
Step 2 - HCV RNA (molecular confirmation)
- Reflex testing on the same sample is recommended to improve linkage to care
- Confirms active viremia; detectable 1-2 weeks after infection (before antibodies appear)
| Anti-HCV Antibody | HCV RNA | Interpretation |
|---|---|---|
| Negative | Negative | Not acute hepatitis C |
| Negative | Positive | Acute hepatitis C (window period - antibodies not yet detectable) |
| Positive | Negative | Probable past/resolved infection (retest in a few weeks; may be a false-positive EIA) |
| Positive | Positive | Difficult to differentiate acute from chronic hepatitis C |
Source: Goldman-Cecil Medicine, Table 134-5
Quantitative HCV RNA: Used to monitor treatment response; lower limit of detection should be 10-20 IU/mL. The HCV RNA level does NOT correlate with disease severity or risk of cirrhosis/HCC.
HCV Genotyping: Previously essential to guide interferon-based treatment duration and selection. With current pan-genotypic DAA regimens, genotyping is no longer routinely recommended (Goldman-Cecil).
Liver Fibrosis Assessment: Non-invasive methods (transient elastography/FibroScan, FIB-4 index, APRI) or liver biopsy are required before therapy to stage fibrosis, identify cirrhosis, and guide post-treatment follow-up for HCC surveillance.
Additional labs: Elevated rheumatoid factor, cryoglobulins (types II and III), and occasionally anti-LKM1 autoantibodies may be found.
Goldman-Cecil Medicine, Ch. 135; Harrison's Principles of Internal Medicine 22E, Ch. 338
7. Treatment
Goals of Therapy
The goal of therapy is Sustained Virologic Response (SVR) - undetectable HCV RNA at 12 weeks (and possibly 24 weeks) after completing therapy. SVR is considered equivalent to a definitive virologic cure. It is associated with:
- Durable suppression of HCV replication
- Reduced all-cause and liver-related mortality
- Regression of liver fibrosis
- Significantly reduced risk of hepatocellular carcinoma (though HCC surveillance must continue in those with established cirrhosis)
Currently, >95% of HCV infections are curable with DAA therapy.
Who Should Be Treated?
All treatment-naive and previously treated patients with chronic HCV infection should be treated without delay, regardless of fibrosis stage or extrahepatic manifestations, except in highly unusual situations with contraindications to available drugs. (Goldman-Cecil; Harrison's)
The Interferon Era (1991-2013) - Historical Context
(Per Harrison's 22E)
- IFN-α monotherapy (1991): SVR <10%
- IFN-α + ribavirin: SVR ~40%
- Pegylated IFN + ribavirin: SVR 55% overall; ~40% in genotypes 1/4 (48 weeks); >80% in genotypes 2/3 (24 weeks)
- First-generation protease inhibitors (telaprevir, boceprevir, 2011) + PEG-IFN/ribavirin: SVR ~65-75% in genotype 1
IFN-based therapy carried significant toxicity: flu-like symptoms, severe fatigue, depression, hemolytic anemia (ribavirin black-box warning), neutropenia, thrombocytopenia, autoimmune disorders, and significant teratogenicity. These regimens are now obsolete.
The DAA Era (2013-Present)
Three classes of DAAs form the basis of curative regimens, targeting specific viral proteins:
| Drug Class | Target | Mechanism |
|---|---|---|
| NS5B Nucleotide Analogues | NS5B RNA polymerase | Sofosbuvir - acts as a chain terminator; prevents RNA replication |
| NS3/4A Protease Inhibitors | NS3/4A protease | Block polyprotein processing (Glecaprevir, Voxilaprevir, Simeprevir) |
| NS5A Inhibitors | NS5A protein | Block virion assembly and replication (Ledipasvir, Velpatasvir, Pibrentasvir, Daclatasvir) |
Current Recommended Pan-Genotypic Regimens (Harrison's 22E; Goldman-Cecil)
| Regimen | Genotype Coverage | Duration | SVR Rate | Key Notes |
|---|---|---|---|---|
| Sofosbuvir/Velpatasvir (Epclusa) | 1-6 (pan-genotypic) | 12 weeks | >95% | Can be used in decompensated cirrhosis; add ribavirin for genotype 3 with cirrhosis |
| Glecaprevir/Pibrentasvir (Mavyret) | 1-6 (pan-genotypic) | 8 weeks (treatment-naive, no cirrhosis) / 12 weeks (compensated cirrhosis) | >95-99% | No dose adjustment needed in renal impairment |
| Ledipasvir/Sofosbuvir (Harvoni) | 1, 4, 5, 6 | 8-12 weeks | 99% (GT1) | Avoid antacids and amiodarone co-administration; 8 weeks if HCV RNA <6 million IU/mL |
| Sofosbuvir/Velpatasvir/Voxilaprevir | 1-6 (pan-genotypic) | 12 weeks | >95% | Reserved for re-treatment after DAA failure |
Acute Hepatitis C Treatment
- Treat all patients with 8 weeks of pan-genotypic oral DAA combination (sofosbuvir/velpatasvir OR glecaprevir/pibrentasvir)
- Although 20-50% spontaneously clear, immediate treatment is cost-effective and provides higher clearance rates
Re-treatment After Failure
- Glecaprevir/pibrentasvir or sofosbuvir/velpatasvir/voxilaprevir are approved for re-treatment
- Extension of treatment course or addition of ribavirin may be needed in cases with resistance-associated variants (RAVs) or cirrhosis
- Expert consultation is recommended after second treatment failure
Important Safety Considerations (Harrison's 22E)
- HBV reactivation warning: All DAAs carry a black-box warning - HBV reactivation can occur in HBsAg-positive patients (and, to a lesser extent, in isolated anti-HBc patients) when HCV is suppressed. Fatal fulminant hepatitis has been reported. HCV treatment should NOT be deferred because of HBV co-infection, but co-infection must be actively managed.
- Drug-drug interactions: Must be checked before initiating any DAA regimen (www.hep-druginteractions.org)
- General tolerability is excellent: headache and fatigue are the most frequently reported side effects
Harrison's Principles of Internal Medicine 22E, Ch. 196 and Ch. 338; Goldman-Cecil Medicine, Ch. 135 and Ch. 328
8. Prevention
No Vaccine Available
There is currently no approved vaccine for HCV. Barriers include the high mutation rate, quasispecies diversity, inadequate neutralizing antibody responses, and incomplete understanding of protective immunity. Several candidates are in human trials but none have achieved sufficient efficacy.
Post-Exposure Prophylaxis
After accidental needlestick exposure:
- Neither immunoglobulin nor antiviral post-exposure prophylaxis is recommended
- Patients should be monitored with HCV RNA and ALT at baseline, week 2, and at 4 and 6 months after exposure
- Documented infection should be treated promptly with 8-week DAA therapy
Public Health Measures
- Universal screening of blood supply (risk now <1 in 2 million donations in the US)
- Harm reduction programs for injection drug use: needle and syringe exchange programs, opioid substitution therapy
- Universal precautions for healthcare workers
- Standard precautions for tattooing, piercing, acupuncture
- Breast-feeding is not contraindicated (unless cutaneous nipple lesions)
- Caesarean section is NOT recommended solely to prevent mother-to-infant transmission
Goldman-Cecil Medicine, Ch. 134
9. Prognosis
With effective DAA therapy achieving SVR:
- Disease progression halts
- Fibrosis can partially reverse (even in advanced cases)
- Risk of HCC is markedly reduced (though not eliminated in established cirrhotics)
- Patients with compensated cirrhosis who achieve SVR still require lifelong HCC surveillance (ultrasound ± AFP every 6 months)
- Patients with decompensated cirrhosis may need liver transplantation even after SVR; however, DAA-based treatment post-transplant is highly effective and prevents graft cirrhosis from recurrent HCV
The long-term prognosis for most patients with chronic hepatitis C, in the absence of treatment, is relatively benign over 1-2 decades - with ~60% of patients remaining asymptomatic and well-compensated. However, approximately one-fourth will progress eventually to end-stage cirrhosis, and HCV-related HCC is a major cause of liver cancer deaths worldwide.
Harrison's Principles of Internal Medicine 22E, Ch. 338; Goldman-Cecil Medicine, Ch. 135
References:
- Harrison's Principles of Internal Medicine, 22nd Edition (2025), McGraw Hill - Chapters 196, 338
- Goldman-Cecil Medicine, International Edition - Chapters 134, 135, 328
This is a shared conversation. Sign in to Orris to start your own chat.