Hi
Hi there! How can I help you today?
Hyperbilirubinemia
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have rich, comprehensive content from multiple authoritative textbooks. Let me compile the full answer.
Hyperbilirubinemia - General Overview
Definition
Hyperbilirubinemia is a blood bilirubin level exceeding 1 mg/dL (17 µmol/L). When it reaches 2-2.5 mg/dL, bilirubin diffuses into tissues producing the yellow discoloration known as jaundice (icterus). Scleral icterus typically appears at serum bilirubin >5 mg/dL. - Harper's Illustrated Biochemistry, 32nd Ed
Bilirubin Metabolism (Quick Review)
Bilirubin is a breakdown product of hemoglobin. The sequence:
- Production: Heme from RBC breakdown is converted to unconjugated (indirect) bilirubin
- Transport: Unconjugated bilirubin travels bound to albumin in blood
- Conjugation: In hepatocytes, UDP-glucuronosyltransferase 1A1 (UGT1A1) conjugates bilirubin with glucuronic acid → water-soluble conjugated (direct) bilirubin
- Excretion: Conjugated bilirubin is secreted into bile via MRP2 (canalicular transporter) → enters GI tract
- Enterohepatic circulation: Gut bacteria convert bilirubin to urobilinogen (excreted in urine) or passed in feces (gives stool its yellow-brown color)
Classification: Two Major Types
1. Unconjugated (Indirect) Hyperbilirubinemia
Also called retention hyperbilirubinemia - due to overproduction or impaired conjugation.
Key features:
- Bilirubin is hydrophobic → cannot appear in urine → acholuric jaundice
- Can cross the blood-brain barrier → risk of kernicterus (bilirubin encephalopathy)
Causes:
| Category | Examples |
|---|---|
| Overproduction | Hemolytic anemias (ABO/Rh incompatibility, G6PD deficiency, sickle cell), ineffective erythropoiesis |
| Impaired hepatic uptake | Gilbert syndrome, some drugs |
| Impaired conjugation | Crigler-Najjar types I & II, Gilbert syndrome, physiologic neonatal jaundice, breast milk jaundice, drugs (novobiocin, chloramphenicol, atazanavir) |
Note: Even with extensive hemolysis, bilirubinemia is usually modest (<4 mg/dL) because a healthy liver has high capacity to metabolize bilirubin. - Harper's Illustrated Biochemistry
2. Conjugated (Direct) Hyperbilirubinemia
Also called regurgitation hyperbilirubinemia - due to reflux into the bloodstream from biliary obstruction or hepatocellular failure.
Key features:
- Conjugated bilirubin is water-soluble → appears in urine → choluric jaundice (dark urine)
- Does NOT cross the blood-brain barrier (no kernicterus risk in adults)
- Associated with pale/acholic stools when biliary obstruction is present
Causes:
| Category | Examples |
|---|---|
| Hepatocellular disease | Viral hepatitis, alcoholic hepatitis, cirrhosis, drug-induced liver injury |
| Biliary obstruction (intrahepatic) | Primary biliary cholangitis, primary sclerosing cholangitis, intrahepatic cholestasis of pregnancy |
| Biliary obstruction (extrahepatic) | Choledocholithiasis, pancreatic head cancer, cholangiocarcinoma, biliary strictures |
| Hereditary | Dubin-Johnson syndrome, Rotor syndrome |
Hereditary Hyperbilirubinemia Syndromes
(Source: Robbins Pathologic Basis of Disease; Harrison's Principles)
| Syndrome | Type | Defect | Bilirubin Level | Clinical Features |
|---|---|---|---|---|
| Gilbert Syndrome | Unconjugated | Reduced UGT1A1 activity (~30% of normal); impaired hepatic uptake. Affects ~5% of Caucasians | Mild, fluctuates 1-3 mg/dL | Benign; exacerbated by fasting, infection, stress; no treatment needed |
| Crigler-Najjar Type I | Unconjugated | Complete absence of UGT1A1; autosomal recessive | Very high: 20-45 mg/dL | Fatal without treatment (kernicterus); phototherapy 10-12 hrs/day; liver transplant curative |
| Crigler-Najjar Type II | Unconjugated | Residual UGT1A1 activity; autosomal recessive | Moderate: 7-20 mg/dL | Milder; responds to phenobarbital (induces UGT1A1) |
| Dubin-Johnson Syndrome | Conjugated | MRP2 gene mutation → impaired canalicular excretion of conjugated bilirubin; autosomal recessive | Mild-moderate | Benign; striking black liver due to melanin-like pigment deposition |
| Rotor Syndrome | Conjugated | Defective hepatic storage/re-uptake of conjugated bilirubin | Mild-moderate | Benign; clinically innocuous; no pigment in liver |
Pathophysiologic Classification at a Glance
PRE-HEPATIC HEPATIC POST-HEPATIC
(overproduction) (hepatocellular) (obstructive)
↓ ↓ ↓
Hemolysis Hepatitis/Cirrhosis Bilestones
G6PD deficiency Gilbert/Crigler-Najjar Pancreatic cancer
Ineffective Alcoholic liver Cholangiocarcinoma
erythropoiesis disease Biliary stricture
↓ ↓ ↓
UNCONJUGATED MIXED/UNCONJUGATED CONJUGATED
Key Distinguishing Points
| Feature | Unconjugated | Conjugated |
|---|---|---|
| Urine bilirubin | Absent (acholuric) | Present (dark urine) |
| Urine urobilinogen | Increased (hemolysis) | Decreased/absent (obstruction) |
| Stool color | Normal/dark | Pale/acholic (if obstruction) |
| Kernicterus risk | Yes | No |
| Crosses BBB | Yes (lipid-soluble) | No (water-soluble) |
| Albumin binding | Yes | No |
Clinical Progression / Complications
- Kernicterus: Unconjugated bilirubin deposits in basal ganglia and brainstem nuclei → irreversible neurological damage (choreoathetosis, sensorineural deafness, intellectual disability). Primarily a neonatal risk.
- Biliary cirrhosis: Persistent cholestatic obstruction → portal fibrosis → cirrhosis
- Ascending cholangitis: Bacterial infection of biliary tree secondary to obstruction - presents with Charcot's triad (fever, right upper quadrant pain, jaundice)
- Gallstone formation: Chronic hemolysis → pigment (bilirubin) gallstones
Sources: Harrison's Principles of Internal Medicine 22E | Harper's Illustrated Biochemistry 32nd Ed | Robbins & Cotran Pathologic Basis of Disease | Tintinalli's Emergency Medicine
Saltatory conduction Physiology in flow chart
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive flowchart-style physiology answer. Here it is:
Saltatory Conduction - Physiology in Flowchart
Structural Basis First
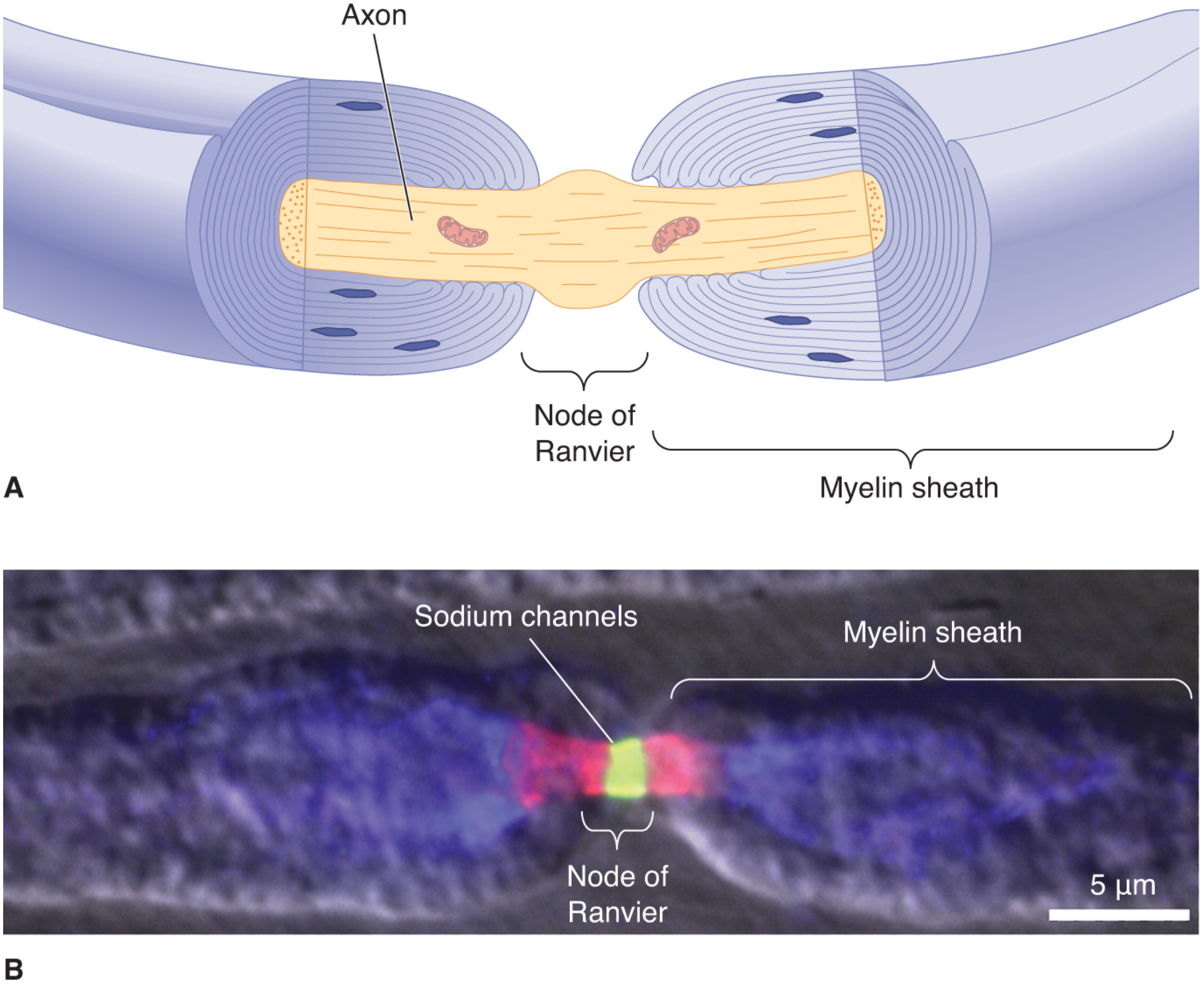
Fig: Node of Ranvier. (A) Axon wrapped in myelin with exposed node. (B) Voltage-gated Na⁺ channels (green/red) densely concentrated at the node. - Neuroscience: Exploring the Brain, 5th Ed
Physiology Flowchart
PREREQUISITE ANATOMY
─────────────────────────────────────────────────────────────
Schwann cell (PNS) / Oligodendrocyte (CNS)
│
▼
Wraps axon in multiple lipid bilayer layers
│
▼
Forms MYELIN SHEATH (sphingomyelin-rich)
• Electrically insulating
• Reduces ion flow ~5,000-fold through membrane
• Decreases membrane capacitance ~50-fold
│
▼
Gaps between adjacent Schwann cells = NODES OF RANVIER
• Only 1-2 μm long
• Spaced every 0.2 - 2.0 mm (internodal distance)
• Dense concentration of voltage-gated Na⁺ channels
• K⁺ channels also present at/near nodes
• Ion flow occurs ONLY here
STEP 1 — STIMULUS ARRIVES AT NODE 0
─────────────────────────────────────────────────────────────
Action potential initiated at one node (Node 0)
│
▼
Depolarization: Node 0 reaches threshold (~-55 mV)
│
▼
Voltage-gated Na⁺ channels OPEN at Node 0
│
▼
Na⁺ rushes IN → membrane depolarizes to ~+30 mV
│
▼
Local current generated INSIDE axoplasm (intracellular)
AND OUTSIDE in extracellular fluid simultaneously
STEP 2 — CURRENT JUMPS ACROSS THE INTERNODE
─────────────────────────────────────────────────────────────
Current flows from Node 0 → toward Node 1
• Myelin = high membrane resistance → prevents ion leak
• Forces current to travel longitudinally down axoplasm
• Current arrives at Node 1 with minimal loss
│
▼
Node 1 is depolarized by this arriving current
│
▼
Threshold reached at Node 1
STEP 3 — ACTION POTENTIAL REGENERATED AT NODE 1
─────────────────────────────────────────────────────────────
Voltage-gated Na⁺ channels open at Node 1
│
▼
New action potential fires at Node 1
│
▼
Process REPEATS: Node 1 → Node 2 → Node 3 → ...
│
▼
Impulse "LEAPS" (Latin: saltare) from node to node
= SALTATORY CONDUCTION
STEP 4 — REPOLARIZATION & UNIDIRECTIONALITY
─────────────────────────────────────────────────────────────
At each node after firing:
│
▼
Voltage-gated Na⁺ channels INACTIVATE (absolute refractory)
│
▼
K⁺ channels OPEN → K⁺ flows OUT → membrane repolarizes
│
▼
Refractory period at prior node prevents backward propagation
│
▼
Signal travels UNIDIRECTIONALLY forward only
FINAL RESULT
─────────────────────────────────────────────────────────────
Fast, efficient, energy-saving nerve impulse conduction
Why Saltatory Conduction is Advantageous
| Advantage | Mechanism | Magnitude |
|---|---|---|
| Speed | AP jumps long internodal distances instead of creeping step-by-step | Up to 120 m/s in myelinated vs ~0.5-2 m/s in unmyelinated |
| Energy conservation | Only nodes depolarize; far fewer ions cross membrane | ~100x less ion movement needed |
| Space efficiency | A thin myelinated axon (~20 µm) conducts as fast as an unmyelinated squid giant axon (1000 µm) | Same velocity in 1/50th the volume |
| Less metabolic cost | Fewer ions displaced = less Na⁺/K⁺-ATPase pump activity required to restore gradients | Conserves ATP |
Source: Guyton & Hall Textbook of Medical Physiology; Medical Physiology (Boron & Boulpaep)
Conduction Velocity by Fiber Type
| Fiber Type | Myelination | Diameter | Velocity | Function |
|---|---|---|---|---|
| Aα | Thick myelin | 12-20 µm | 70-120 m/s | Motor, proprioception |
| Aβ | Thick myelin | 5-12 µm | 30-70 m/s | Touch, pressure |
| Aδ | Thin myelin | 2-5 µm | 5-30 m/s | Fast pain, temperature |
| C | Unmyelinated | 0.2-1.5 µm | 0.5-2 m/s | Slow pain, postganglionic autonomic |
What Happens When Myelin is Lost?
DEMYELINATION (e.g., Multiple Sclerosis, Guillain-Barré)
│
▼
Myelin sheath degraded or absent between nodes
│
▼
Current leaks through internode → cannot jump to next node
│
▼
Saltatory conduction FAILS
│
▼
Either:
├─ Slowed conduction (partial demyelination)
└─ Complete conduction block (severe demyelination)
│
▼
Clinical: Weakness, sensory loss, visual disturbance,
lack of coordination
Key Concept Summary:
Myelin acts like insulating tape on a leaky hose - it forces current to travel fast and far down the axoplasm, regenerating the action potential only at exposed nodes, achieving high-speed conduction at a fraction of the metabolic cost.
Sources: Guyton & Hall Textbook of Medical Physiology | Neuroscience: Exploring the Brain, 5th Ed | Medical Physiology (Boron & Boulpaep)
This is a shared conversation. Sign in to Orris to start your own chat.