Pathologicsl changes that scrotal ultrasound can show
Reading File
Finding Sources
Finding Sources
Searching the Web
scrotal ultrasound pathological findings radiology
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compile a thorough, well-organized response.
Pathological Changes Detectable on Scrotal Ultrasound
Scrotal ultrasound (high-frequency 5-15 MHz with color Doppler) is the first-line imaging for acute and chronic scrotal conditions, capable of identifying both intra- and extra-testicular pathology with high accuracy.
1. Testicular Torsion
The most time-critical diagnosis. US has ~95% diagnostic accuracy when combined with Doppler.
Grayscale findings:
- "Whirlpool sign" - a twisted spermatic cord seen above the testis (pathognomonic)
- Testicular enlargement and edema (early)
- Heterogeneous parenchymal echotexture - indicates late/advanced torsion with non-viability
- Homogeneous echotexture = favorable viability sign
Doppler findings:
- Absent/reduced intratesticular blood flow (white box in the image below shows no flow)
- Degree of twisting determines the pattern:
- 180° or less: only venous flow ceases; arterial flow persists (can be falsely reassuring)
-
180°: both arterial and venous flow cease - no Doppler signal

Important caveat: Up to 24-26% of confirmed torsion cases can show preserved intratesticular flow on Doppler. US should never delay urologic consultation when torsion is clinically suspected.
- Rosen's Emergency Medicine, p. 1402; Campbell-Walsh-Wein Urology
2. Epididymo-Orchitis
Gray-scale:
- Enlarged epididymis (focal or diffuse) with heterogeneous or hypoechoic echotexture
- Enlarged, hypoechoic testis in orchitis
- Skin thickening and scrotal wall edema
- Reactive hydrocele (fluid between tunica layers)
- Scrotal abscess: complex fluid collection with thick walls (rare)
Doppler:
- Markedly increased vascular flow to the epididymis and/or testis ("hyperemia")
- This is the opposite of torsion - hyperemia favors infection over ischemia
Complication: Scrotal/testicular abscess appears as a complex, heterogeneous fluid collection - detectable on US and requires urologic consultation.
- Smith & Tanagho's General Urology, p. 728; Rosen's Emergency Medicine
3. Germ Cell Tumors (Testicular Cancer)
- Discrete hypoechoic intratesticular mass (most common appearance)
- Heterogeneous echotexture - more common in non-seminomatous GCT (NSGCT) due to mixed elements
- Homogeneous echotexture - favors pure seminoma
- Two or more discrete lesions may be present
- Increased color Doppler flow within the lesion suggests malignancy (absence does not exclude it)
- High-frequency transducers (5-10 MHz) can detect lesions as small as a few millimeters
- Both testes must be scanned (bilateral GCT occurs in ~2%)
- Campbell-Walsh-Wein Urology, p. 2248
4. "Burned-Out" Primary Testicular Tumor
In men with advanced GCT and a normal testicular exam, US is used to identify:
- Small impalpable stellate scar
- Coarse intratesticular calcification
- Discrete nodule
These findings indicate a "burned-out" primary tumor (spontaneous regression, most commonly seminoma). Radical orchiectomy is still indicated if any of these sonographic signs are present.
- Campbell-Walsh-Wein Urology, p. 2248
5. Small Impalpable Intratesticular Lesions (<10 mm)
US increasingly detects incidental lesions. The differential includes:
| Finding | Likelihood of malignancy |
|---|---|
| Lesion <1 cm | ~50% |
| Lesion 1-2 cm | 80%+ |
| Testicular cysts | Benign |
| Small infarcts | Benign |
| Leydig/Sertoli cell nodules | Usually benign |
Management options range from inguinal orchiectomy to testis-sparing surgery or serial US surveillance.
6. Varicocele
The most important indication in infertile males. Color Doppler US is the standard diagnostic tool.
Findings:
- Dilated pampiniform plexus veins appearing as tubular echo-free (anechoic) structures adjacent to the testis
- Venous diameter >3 mm = abnormal
- Retrograde venous flow on Valsalva maneuver is the hallmark radiologic feature
- Both resting and Valsalva views are obtained (as shown in the image below)
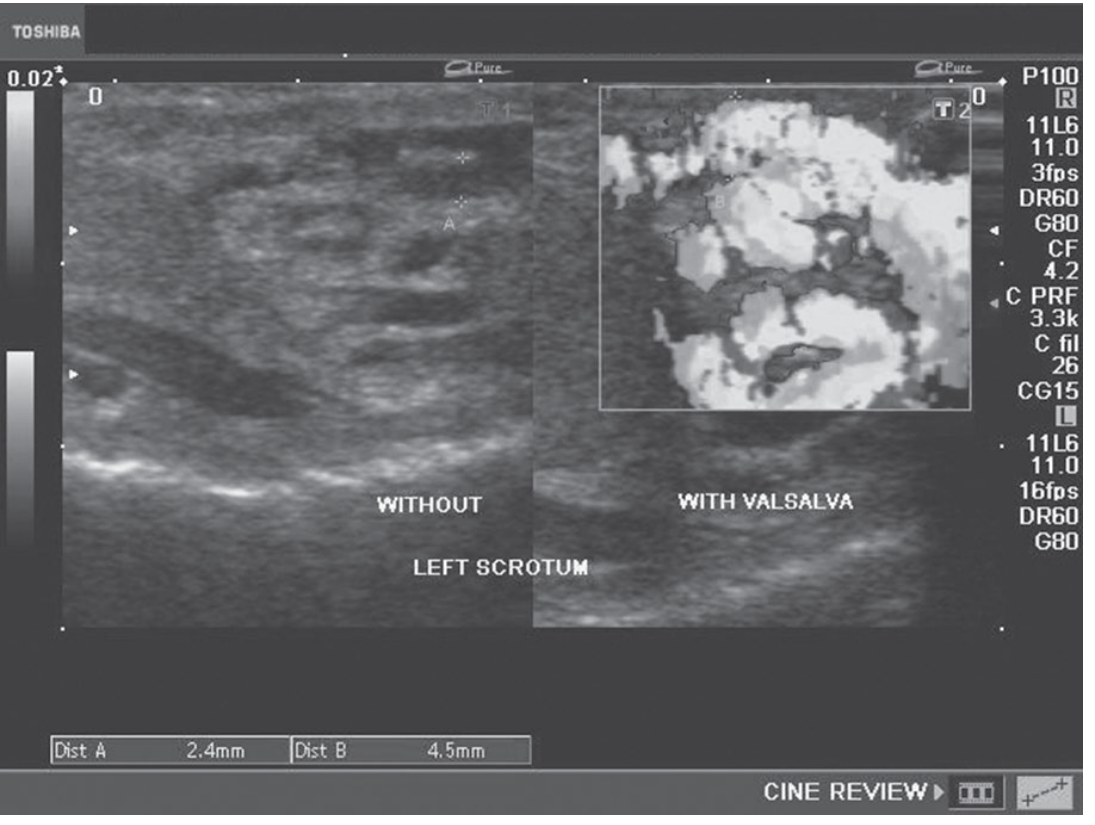
Can detect subclinical varicoceles (not palpable on physical exam).
- Smith & Tanagho's General Urology, p. 728
7. Hydrocele
- Anechoic (echo-free) fluid collection surrounding the testis between the layers of the tunica vaginalis
- Simple hydrocele: purely anechoic
- Complex hydrocele: echoes within fluid (suggests infection, hemorrhage, or tumor)
- US is indicated when hydrocele prevents testicular palpation on exam
8. Epididymal Cyst / Spermatocele
- Smooth, well-defined anechoic or hypoechoic cystic structure in the epididymis
- Spermatocele: typically in the head of the epididymis, contains spermatozoa
- Both are benign extratesticular findings
9. Testicular Microlithiasis
- Multiple small echogenic foci (<3 mm) scattered within the testicular parenchyma
- Bilateral in many cases
- Association with GCT is debated; current evidence suggests the finding alone should not prompt further evaluation without other risk factors
- Campbell-Walsh-Wein Urology, p. 2248
10. Scrotal Trauma
- Hematocele: complex fluid with echoes between tunica layers (hemorrhage)
- Testicular rupture: disruption of the tunica albuginea, heterogeneous parenchyma, irregular contour
- Hematoma: heterogeneous intratesticular or extratesticular collection
- Doppler helps assess residual blood flow / viability
11. Appendix Testis / Appendix Epididymis Torsion
- Small echogenic or hypoechoic nodule at the upper pole of the testis or epididymis
- Reactive hydrocele and epididymal hyperemia may be present
- "Blue dot sign" is a clinical correlate
12. Inguinal Hernia into Scrotum
- Bowel loops or omentum visible in the scrotal sac
- Peristalsis may be seen in real-time US
Summary Table
| Condition | Key US Finding |
|---|---|
| Testicular torsion | Absent Doppler flow, whirlpool sign, heterogeneous echo |
| Epididymo-orchitis | Enlarged epididymis/testis, increased Doppler flow |
| Germ cell tumor | Hypoechoic intratesticular mass, ± increased Doppler |
| Varicocele | Dilated veins >3mm, retrograde flow on Valsalva |
| Hydrocele | Anechoic peritesticular fluid |
| Epididymal cyst | Anechoic extratesticular cyst, epididymal head |
| Microlithiasis | Scattered small echogenic foci in parenchyma |
| Trauma/hematocele | Complex fluid, disrupted tunica, hematoma |
| Burned-out tumor | Scar, coarse calcification, small nodule |
| Scrotal hernia | Bowel/omentum with peristalsis |
Sources:
- Campbell-Walsh-Wein Urology, 3-Volume Set - Scrotal Ultrasonography section
- Smith and Tanagho's General Urology, 19th Edition - Scrotal Ultrasound & Varicocele
- Rosen's Emergency Medicine - Testicular Torsion, Epididymitis/Orchitis chapters
This is a shared conversation. Sign in to Orris to start your own chat.