Defibrillator
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
All the content and images are in hand. Here is the full explanation:
How a Defibrillator Works
The Problem: Ventricular Fibrillation
The target rhythm for defibrillation is ventricular fibrillation (VF) - a chaotic, disorganized electrical activity where individual cardiac muscle fibers contract asynchronously, producing no effective pumping. On an ECG it looks like this:
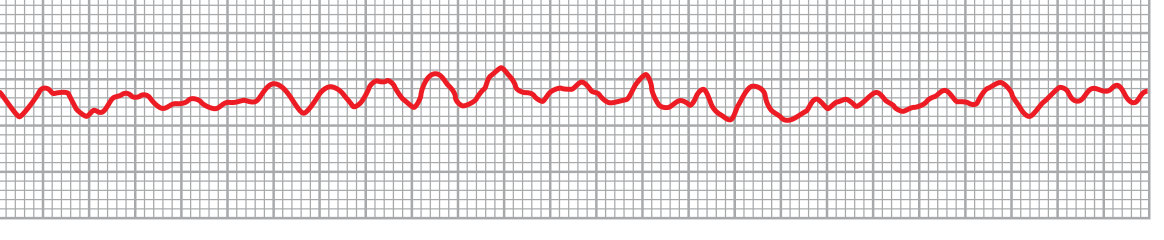
Ventricular fibrillation (lead II) - Guyton and Hall Textbook of Medical Physiology
The fibrillation is self-sustaining because multiple reentrant electrical circuits keep recycling through different patches of myocardium, each at different stages of excitability. No single circuit is in charge; the sinus node loses control.
The Core Mechanism
The fundamental principle is simultaneous mass depolarization of the ventricular myocardium.
"A strong high-voltage electrical current passed through the ventricles for a fraction of a second can stop fibrillation by throwing all the ventricular muscle into refractoriness simultaneously. This is accomplished by passing intense current through large electrodes placed on two sides of the heart. The current penetrates most of the fibers of the ventricles at the same time, thus stimulating essentially all parts of the ventricles simultaneously and causing them all to become refractory. All action potentials stop, and the heart remains quiescent for 3 to 5 seconds, after which it begins to beat again, usually with the sinus node or some other part of the heart becoming the pacemaker."
- Guyton and Hall Textbook of Medical Physiology
In short: the shock does not "restart" the heart - it stops it completely by forcing every muscle fiber into simultaneous refractory state. With all re-entrant circuits extinguished, the sinus node can then resume as the dominant pacemaker.
The Physics: Capacitor Discharge
The defibrillator works by charging a large electrical capacitor to several thousand volts, then discharging it in a very brief pulse (a few milliseconds) through electrodes placed across the chest wall. The current path passes through the chest and heart.
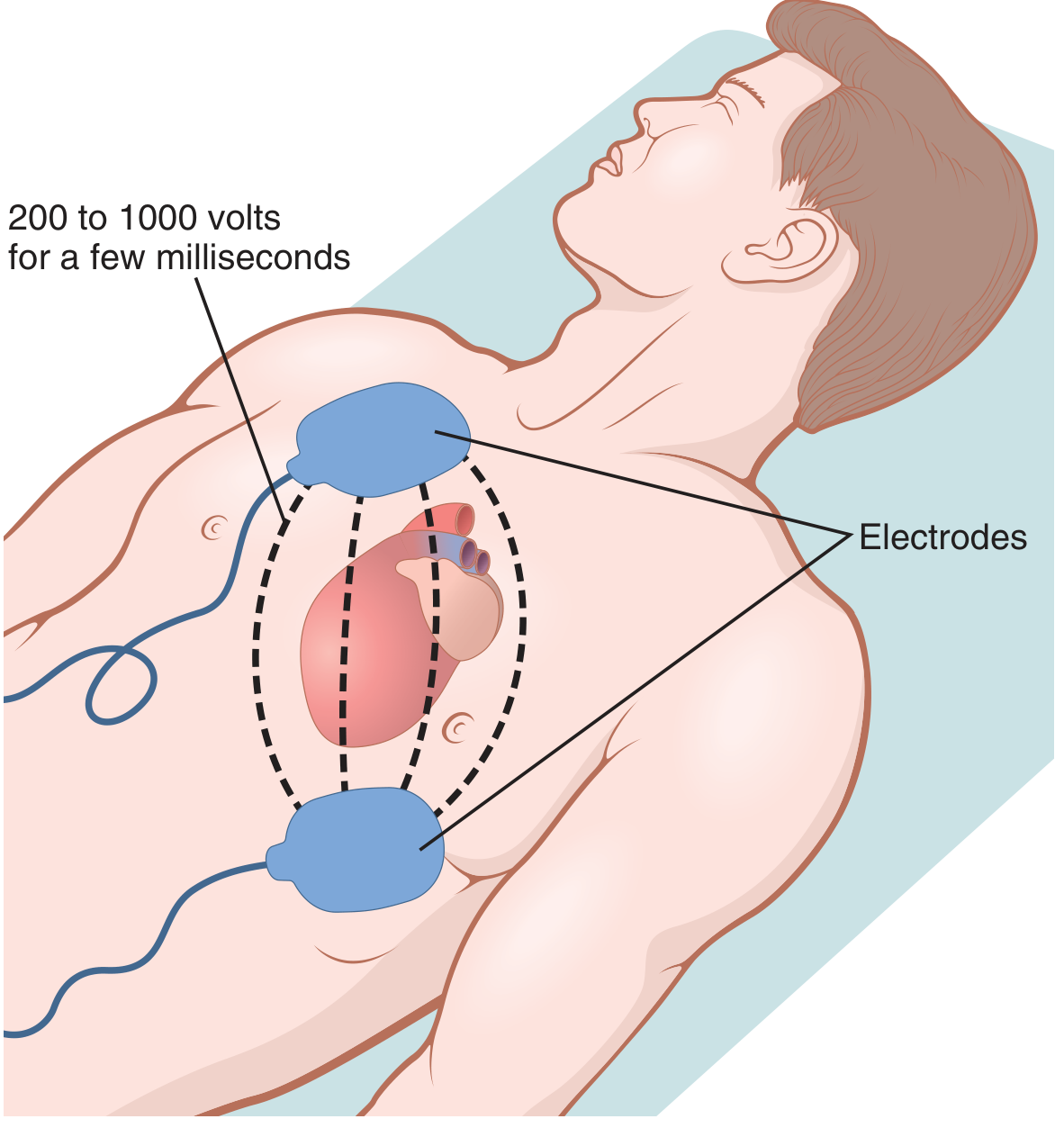
External defibrillation - electrodes placed on the chest wall, current passes through the heart - Guyton and Hall
- Direct cardiac electrodes (e.g. in surgery): 200-1000 V
- External chest electrodes: Several thousand volts, discharged through the chest wall to deliver ~120-360 J to the heart
Monophasic vs. Biphasic Waveforms
| Feature | Monophasic | Biphasic |
|---|---|---|
| Current direction | One direction only | Reverses direction mid-shock |
| Energy required | 200-360 J | 120-200 J |
| Myocardial injury | Higher risk | Lower risk |
| Current standard? | Older devices | All modern devices |
"In most cases, defibrillation current is delivered to the heart in biphasic waveforms, alternating the direction of the current pulse through the heart. This form of delivery substantially reduces the energy needed for successful defibrillation, thereby decreasing the risk for burns and cardiac damage."
- Guyton and Hall Textbook of Medical Physiology
Biphasic waveforms work better because reversing current direction exploits the asymmetric ion channel properties of cardiac membranes, achieving the same depolarization threshold with less total energy. Two subtypes exist: biphasic truncated exponential (BTE) and rectilinear biphasic (RBW).
Transthoracic Impedance
Not all delivered energy reaches the heart - the chest wall, lungs (full of air), and tissues all resist current flow. Modern AEDs use impedance-compensating technology: they sense the patient's transthoracic impedance and automatically adjust the current delivered so the actual energy reaching the heart is consistent regardless of body habitus.
Electrode pad placement matters for minimizing impedance and maximizing current through the heart:
- One pad: upper right sternal border, just below the clavicle
- Other pad: just lateral to the left nipple, top of pad a few inches below the axilla
Why Timing is Everything
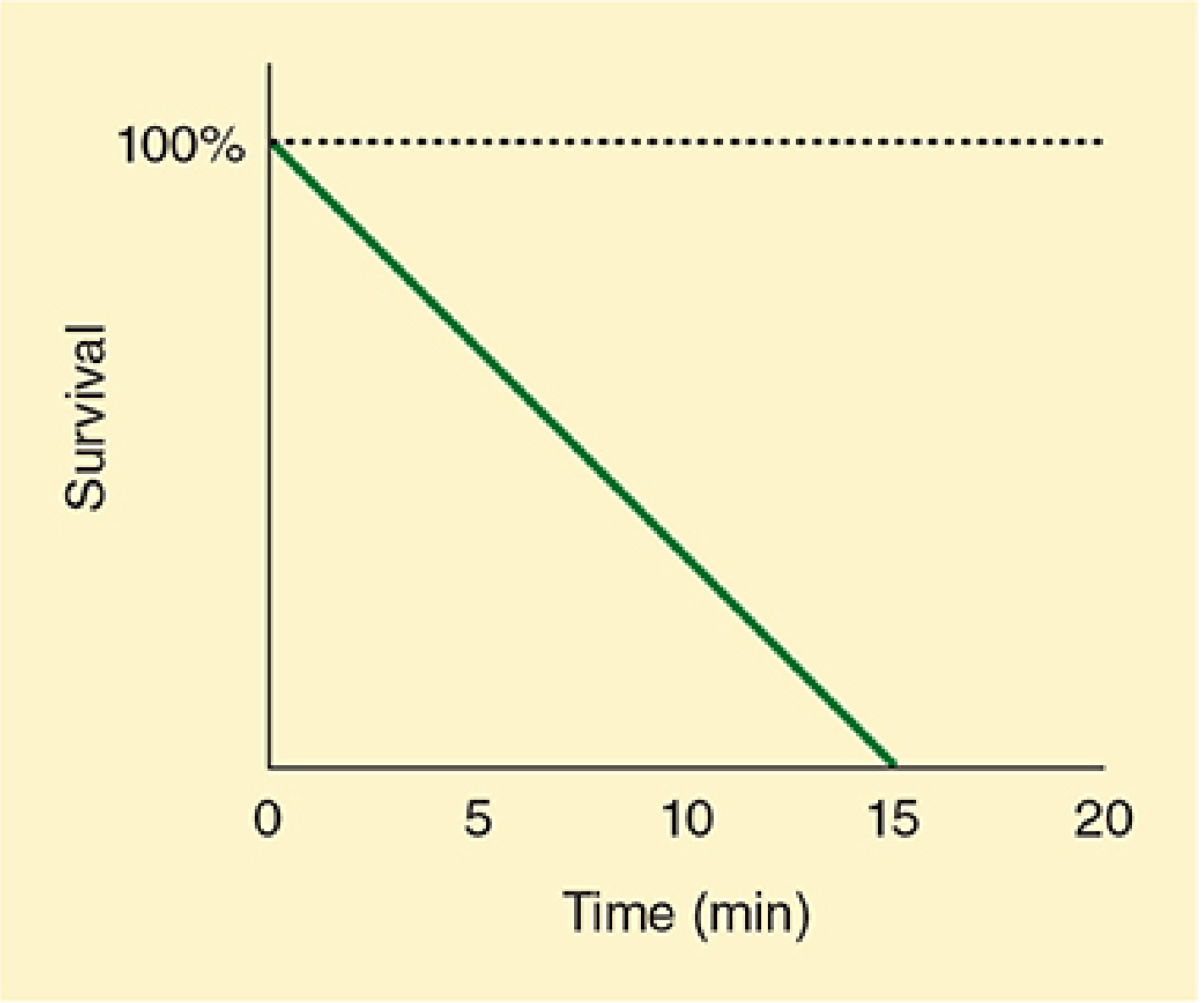
Survival declines 7-10% for every minute without defibrillation - Morgan and Mikhail's Clinical Anesthesiology
As VF persists, the myocardium becomes progressively depleted of ATP (energy stores), acidotic, and hypoxic. After about 4-5 minutes the fibrillating muscle is too metabolically compromised to respond to a shock - "fine" VF degenerates into asystole. This is why the chain of survival places defibrillation within the first 3-5 minutes as the highest-priority intervention.
AEDs: Automating the Decision
Automated External Defibrillators (AEDs) add a layer of intelligence on top of the basic physics:
- ECG analysis: Microprocessor algorithms analyze the rhythm with high sensitivity and specificity, distinguishing shockable (VF, pulseless VT) from non-shockable (asystole, PEA) rhythms
- Impedance measurement: Auto-adjusts energy delivery
- Voice prompts: Guide untrained bystanders step-by-step
- Biphasic shock delivery: All modern AEDs deliver biphasic waveforms at 120-200 J
ICDs: Miniaturizing the Principle
Implantable cardioverter-defibrillators (ICDs) apply the same mechanism internally. A battery-powered device is implanted subcutaneously or in the chest, with electrode leads placed in the right ventricle. It continuously monitors rhythm; when VF is detected, it fires a brief electrical impulse directly to the myocardium - requiring far less energy than external defibrillation because there is no chest wall impedance.
Sources:
- Guyton and Hall Textbook of Medical Physiology - Ventricular Defibrillation, p. 174
- Morgan and Mikhail's Clinical Anesthesiology, 7e - Defibrillation, p. 2393-2394
- Braunwald's Heart Disease - Defibrillation-Cardioversion, p. 669-670
This is a shared conversation. Sign in to Orris to start your own chat.