Testicular torsion ..differential diagnosis and signs
Reading File
Finding Sources
Finding Sources
Searching the Web
testicular torsion differential diagnosis clinical signs
Reading File
Reading File
Reading File
Reading File
Searching Images
testicular torsion bell clapper deformity anatomy
I now have comprehensive information. Let me compile a thorough, well-structured answer.
Testicular Torsion: Differential Diagnosis & Clinical Signs
Pathophysiology
Testicular torsion occurs when the spermatic cord twists, occluding arterial blood supply to the testis. The underlying anatomical predisposition is the bell-clapper deformity — failure of the tunica vaginalis to anchor the posterior scrotal wall, allowing the testis to rotate freely. This occurs in ~12% of males bilaterally.
- Intravaginal torsion: peaks at puberty (adolescent surge in testicular size)
- Extravaginal torsion: occurs in neonates/perinatal period
- Time is critical: irreversible damage begins at 4–6 hours; salvage approaches 100% if corrected <6 h, but drops sharply thereafter
Clinical Signs & Symptoms
Symptoms
| Feature | Description |
|---|---|
| Pain onset | Sudden, severe; does not require trauma (only ~4–8% trauma-related) |
| Pain location | Lower abdominal quadrant, inguinal canal, or scrotum |
| Nausea/vomiting | Present in ~50% — increases suspicion significantly |
| Dysuria | Usually absent (helps distinguish from epididymitis) |
| Fever | Usually absent early |
Physical Examination Signs
| Sign | Finding |
|---|---|
| Absent cremasteric reflex | Most diagnostically useful sign — elicited by stroking medial thigh causing ipsilateral testicular elevation; absence strongly suggests torsion (sensitivity 73–96%) |
| High-riding testis | Testis elevated in scrotum due to cord shortening from twisting |
| Transverse (horizontal) lie | Testis rotated to lie horizontally rather than vertically |
| Tender testis | Diffuse, severe tenderness; firmness on palpation |
| Epididymis displaced | Not in normal posterolateral position (may be anterior) |
| Prehn's sign | Pain relief with scrotal elevation — classically associated with epididymitis (positive), but unreliable for distinguishing torsion from epididymitis |
| Reactive hydrocele | May be present, especially in late presentation |
| Scrotal erythema/edema | Develops as torsion progresses to infarction |
TWIST Score (Clinical Risk Stratification)
Five clinical features scored to stratify risk:
- Testicular swelling (+2)
- Hard testis (+2)
- Absent cremasteric reflex (+1)
- Nausea/vomiting (+1)
- High-riding testis (+1)
Score ≥5: High risk → immediate surgical exploration (no imaging needed)
Score 2–4: Intermediate → urgent Doppler ultrasound
Score 0–1: Low risk → ultrasound to evaluate further
Score 2–4: Intermediate → urgent Doppler ultrasound
Score 0–1: Low risk → ultrasound to evaluate further
Differential Diagnosis of Acute Scrotum
The table below is adapted from Tintinalli's Emergency Medicine (Table 93-1):
| Feature | Testicular Torsion | Epididymitis | Appendage Torsion |
|---|---|---|---|
| Peak age | Neonates, adolescents | Adolescents, young adults | Prepubertal (7–12 yrs) |
| Pain onset | Sudden | Gradual, progressive | Variable |
| Nausea/vomiting | More likely | Less likely | Less likely |
| Dysuria | Less likely | More likely | Less likely |
| Fever | Less likely | More likely | Less likely |
| Cremasteric reflex | Absent | Present | Present |
| Tenderness location | Entire testis → diffuse hemiscrotal | Epididymis → diffuse | Localized to superior pole (head of testis) |
| Prehn's sign | Negative (pain not relieved) | Positive (pain relieved) | Variable |
| "Blue dot" sign | Absent | Absent | Pathognomonic — visible blue-black nodule at superior pole |
| Urinalysis | Normal | Often pyuria/bacteriuria | Normal |
Full Differential Diagnosis List
- Torsion of testicular appendage (appendix testis/epididymis) — most common mimic; indolent onset, superior pole tenderness, "blue dot" sign visible through scrotal skin; does NOT require emergency surgery
- Epididymitis / Epididymo-orchitis — gradual onset; STI (gonorrhea, chlamydia) in young adults; enteric bacteria in older men; fever, pyuria, Prehn's sign positive; increased vascularity on Doppler
- Orchitis — viral (mumps classically), bilateral; parotitis may be present; intact cremasteric reflex
- Incarcerated/strangulated inguinal hernia — bowel sounds in scrotum; inguinal swelling; bowel obstruction features
- Trauma — history of direct injury; however, torsion can be triggered by trauma and must not be excluded solely on this basis
- Henoch-Schönlein Purpura (HSP) — purpuric rash, arthralgia, abdominal pain, haematuria in children; scrotal involvement possible
- Testicular tumour — painless mass usually; may have dull ache; associated hydrocele; cryptorchidism history
- Hydrocele — transilluminates; non-tender; may be secondary to cancer
- Varicocele — "bag of worms" appearance; worse on standing; usually left-sided; often asymptomatic
- Fournier's gangrene — necrotising fasciitis of perineum; systemic sepsis; crepitus; diabetic/immunocompromised patients — life-threatening
- Referred pain — ureteric colic (stone at VUJ), retroperitoneal haematoma
Imaging
Scrotal Doppler Ultrasound is the test of choice for equivocal cases:
- Torsion: absent or markedly reduced intratesticular blood flow; heterogeneous echotexture in late torsion; horizontal lie; "whirlpool sign" of twisted cord
- Epididymitis: increased hyperaemia of epididymis ± testis
- Appendage torsion: small avascular ovoid structure near superior pole with surrounding hyperaemia
⚠️ Do not delay surgical exploration to await imaging if clinical suspicion is high. Sensitivity of Doppler US is only 83–90% — partial torsion can show preserved flow.
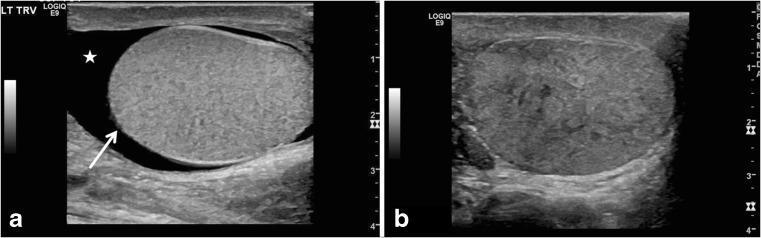
Scrotal ultrasound: (a) horizontal lie of testis with reactive hydrocele (★) — classic bell-clapper sign; (b) heterogeneous parenchymal echotexture indicating late-stage torsion with non-viability.
Management Summary
- High suspicion → Emergent urologic consultation → Scrotal exploration
- Manual detorsion can be attempted ("open book" maneuver — rotate outward like opening a book) while awaiting theatre, but should not delay surgery
- Bilateral orchiopexy is performed at the same setting (contralateral bell-clapper deformity is present in 80%)
- Non-viable testis → orchiectomy
Sources: Tintinalli's Emergency Medicine (9e), Rosen's Emergency Medicine, Sabiston Textbook of Surgery, Campbell-Walsh Urology
Prehn sign deming sign and angel sign
Finding Sources
Finding Sources
Searching the Web
Prehn sign Deming sign angel wing sign testicular torsion epididymitis
Finding Sources
Reading File
Searching the Web
"Deming sign" testicular torsion scrotum clinical sign
Searching the Web
"angel sign" OR "angel wing sign" testicular torsion
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC10643379/
Now I have enough information to give a thorough, accurate answer on all three signs.
Prehn's Sign, Deming Sign & Angel Sign in Testicular/Scrotal Disease
1. Prehn's Sign
What it is: A bedside clinical maneuver to help differentiate epididymitis from testicular torsion.
How to elicit it:
Gently lift and support the scrotum on the affected side (elevating the testicle toward the pubic symphysis) while observing the patient's pain response.
Interpretation:
| Response | Interpretation |
|---|---|
| Positive Prehn's sign — pain relieved with elevation | Suggests epididymitis (venous drainage improved, inflammatory congestion relieved) |
| Negative Prehn's sign — pain unchanged or worsened with elevation | Suggests testicular torsion (ischemic pain unaffected or worsened by repositioning) |
Anatomical basis: In epididymitis, the pain arises from inflammatory congestion. Elevating the scrotum improves venous/lymphatic drainage and partially decompresses the inflamed epididymis, relieving pain. In torsion, the pain is ischemic — elevation does nothing to restore arterial flow.
Clinical value — IMPORTANT CAVEAT:
Prehn's sign is notoriously unreliable and should NOT be used to rule in or rule out torsion. Studies have found it positive (pain relieved) in up to 91% of torsion cases in some series. It is a supporting clue only — it must never delay surgical exploration if torsion is suspected.
"Relief of pain with elevation of the affected testicle (Prehn's sign-positive for epididymitis) does not reliably distinguish torsion from epididymitis." — Tintinalli's Emergency Medicine, 9e
2. Deming Sign (Sign of Deming)
What it is: A physical examination sign described in testicular torsion, specifically relating to the position and orientation of the epididymis.
How to elicit it:
On palpation of the scrotum, the epididymis is found to have rotated anteriorly (to the front of the testis) rather than occupying its normal posterolateral position.
Interpretation:
- Normal: Epididymis is palpable posterolaterally
- Deming sign positive: Epididymis is displaced anteriorly (or superiorly), indicating that the spermatic cord has twisted and rotated the entire testis-epididymis unit
Significance: This anterior displacement of the epididymis indicates intravaginal torsion — the cord has twisted, rotating the testis so the epididymis no longer sits in its normal anatomical position. It is a useful confirmatory sign when present, especially early in the course before reactive swelling obscures anatomy. Once significant scrotal edema develops, palpating the epididymis position becomes impossible.
3. Angel Sign (Angel Wing Sign)
What it is: A clinical or ultrasound sign associated with epididymitis/epididymo-orchitis, not torsion — helping differentiate it from torsion.
How described:
The "angel sign" refers to the symmetric bilateral enlargement and hyperaemia of the epididymides on scrotal Doppler ultrasound, creating a wing-like appearance on either side of the midline — resembling "angel wings." In the context of clinical examination, a positive angel sign along with positive Prehn's sign points toward epididymitis rather than testicular torsion.
Significance: As noted in the PMC literature: "a positive Prehn's sign and angel sign" point toward epididymitis as the diagnosis, effectively helping exclude torsion. The angel sign on ultrasound shows increased bilateral epididymal flow (even if the contralateral side is subclinically inflamed), contrasting sharply with the absent/reduced unilateral flow seen in torsion.
Summary Comparison Table
| Feature | Torsion | Epididymitis |
|---|---|---|
| Prehn's sign | Negative (pain not relieved) | Positive (pain relieved) |
| Deming sign | Positive (anterior epididymis displacement) | Negative (normal epididymis position) |
| Angel sign | Negative | Positive (hyperaemic epididymides, wing-like on USS) |
| Cremasteric reflex | Absent | Present |
| Pain onset | Sudden | Gradual |
| Doppler USS | Absent/reduced flow | Increased flow |
Key Clinical Pearl
All three signs have limited individual reliability. The absent cremasteric reflex remains the single most sensitive physical sign for torsion. The TWIST score integrating multiple findings is the most validated clinical tool. When torsion cannot be excluded, do not wait — proceed to scrotal exploration.
Sources: Tintinalli's Emergency Medicine (9e), Gray's Anatomy for Students, Rosen's Emergency Medicine, PMC [PMID 10643379]
This is a shared conversation. Sign in to Orris to start your own chat.