Selective aortic arch perfusion (SAAP) technique as emergency physician
Reading File
Finding Sources
Finding Sources
Searching PubMed
"selective aortic arch perfusion" emergency resuscitation
Searching the Web
selective aortic arch perfusion SAAP emergency physician technique procedure
Reading File
Reading Article
PMID: 38087352
Reading Article
PMID: 42062049
Reading Article
PMID: 33791103
Reading File
Reading Article
PMID: 31348400
Reading Article
PMID: 26766760
Loading Image
Finding Sources
Reading Web Page
https://www.stemlynsblog.org/selective-aortic-arch-perfusion
Excellent - I now have comprehensive information to write a thorough answer. Let me compile everything.
Selective Aortic Arch Perfusion (SAAP) for the Emergency Physician
What Is SAAP?
SAAP is an advanced endovascular resuscitation technique that combines descending thoracic aortic occlusion (like REBOA) with active extracorporeal perfusion of the proximal aorta - simultaneously restoring perfusion pressure to the heart and brain while limiting ischemia to sub-diaphragmatic organs. It was originally described by James Manning, MD (emergency physician, University of North Carolina) in 1992 and has been under active development ever since.
Conceptually it sits one step beyond REBOA in the endovascular resuscitation ladder:
REBOA (occlusion only) → SAAP (occlusion + perfusion) → Full ECPR/ECMO
Mechanism & Physiology
The key physiological goals are:
| Goal | Mechanism |
|---|---|
| Restore coronary perfusion pressure | Balloon in descending aorta isolates arch; infused flow is directed to coronary ostia |
| Restore cerebral perfusion | Carotid and vertebral arteries fed directly from the arch |
| Reduce sub-diaphragmatic ischemia-reperfusion injury | Occlusion limits injury to abdominal viscera during arrest |
| Achieve ROSC | Direct myocardial oxygen delivery restores electrical and mechanical activity |
| Bridge to ECMO or damage control surgery | Short-term perfusion buys time for definitive intervention |
With balloon inflation in the descending thoracic aorta and a competent aortic valve, all infused oxygenated blood is directed retrograde into the aortic arch, then forward into the coronary arteries, carotid arteries, and vertebral arteries. The abdominal aorta is excluded.
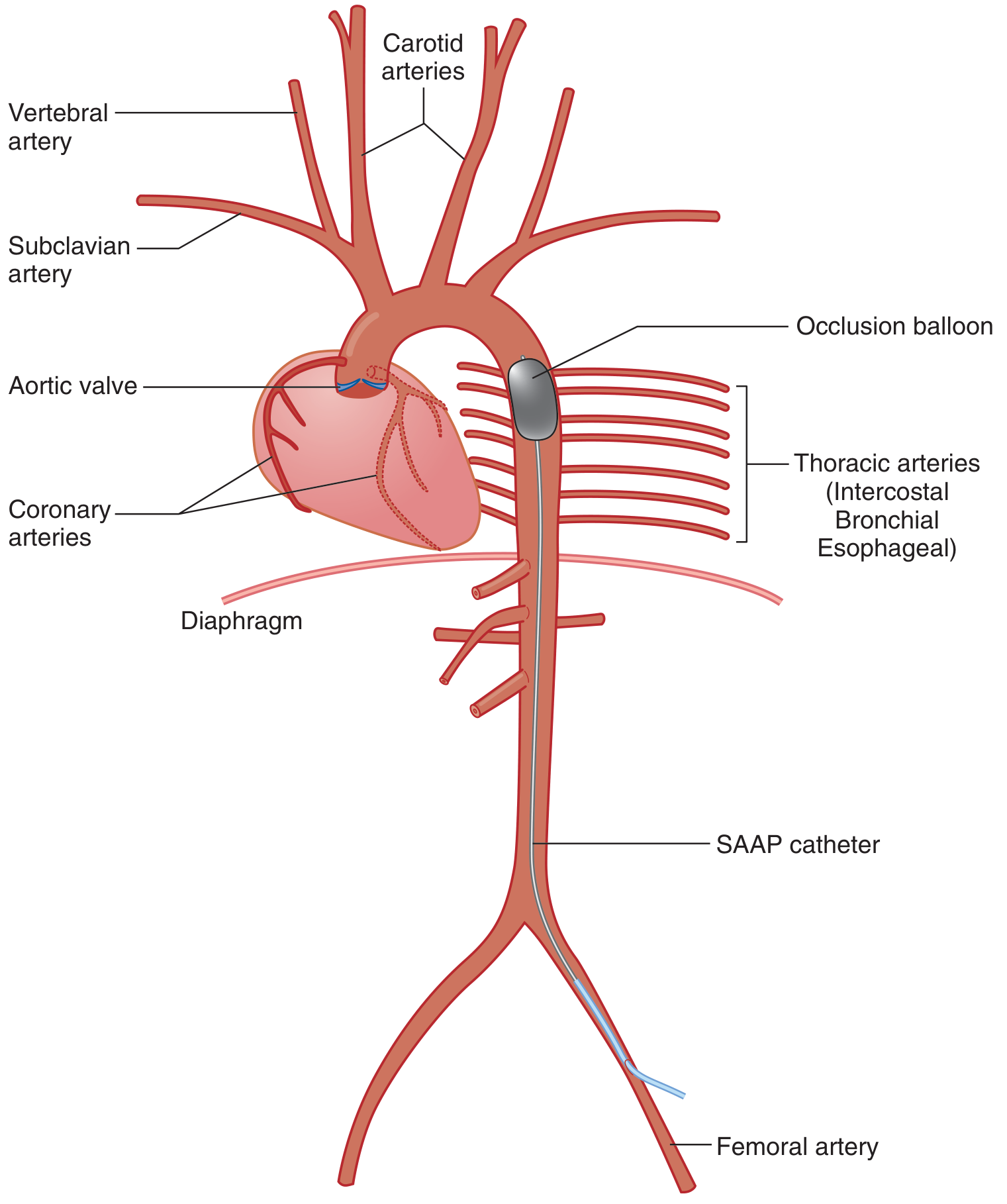
Figure: SAAP catheter inserted via femoral artery; occlusion balloon inflated in descending thoracic aorta isolates the arch, directing oxygenated perfusate to coronary, carotid, and vertebral arteries. [Manning JE, used with permission - Tintinalli's Emergency Medicine]
Indications
SAAP has been studied in two main clinical scenarios:
-
Cardiac arrest (medical or traumatic)
- Non-compressible torso hemorrhage leading to hemorrhage-induced traumatic cardiac arrest (HiTCA)
- Medical cardiac arrest refractory to standard CPR and ACLS (particularly where coronary ischemia is the cause)
-
Hemorrhagic shock with impending arrest
- Acts like an enhanced REBOA - provides occlusion AND active organ perfusion
- Particularly useful when REBOA alone cannot maintain coronary/cerebral perfusion pressure
"SAAP can be used for cardiac arrest and hemorrhage-induced traumatic cardiac arrest (similar to resuscitative endovascular balloon occlusion of the aorta)." - Tintinalli's Emergency Medicine, p.205
Equipment
- SAAP catheter: A large-lumen (typically >12 Fr) balloon occlusion catheter with a central lumen for perfusate infusion. A prototype used in human cadaveric studies was inserted via a standard femoral percutaneous access device.
- Oxygenator: The perfusate MUST be oxygenated before infusion (the lungs are bypassed). Options include:
- Portable ECMO-type oxygenators
- HBOC (hemoglobin-based oxygen carriers) such as HBOC-201 - particularly relevant for prehospital/austere settings where whole blood logistics are challenging
- Fresh whole blood (FWB) - highest efficacy in animal models
- Packed red blood cells (diluted in normal saline, not lactated Ringer's) + oxygenator
- Fluoroscopy: Ideal for catheter positioning; cadaveric studies used fluoroscopic guidance. Ultrasound guidance for femoral access is the standard first step.
- Calcium gluconate for intra-aortic infusion: If using citrate-anticoagulated stored blood, co-infusion of calcium gluconate is mandatory to prevent citrate-induced hypocalcemia, refractory ventricular fibrillation, and failure of ROSC.
Procedural Steps (Current Protocol)
-
Femoral arterial access - Seldinger technique, typically right common femoral artery, under ultrasound guidance. Large-bore access (12 Fr or similar).
-
Catheter insertion and advancement - The large-lumen balloon catheter is advanced over a wire up through the aorta to the descending thoracic aorta (analogous to REBOA Zone I placement - at or just distal to the left subclavian artery origin).
-
Balloon inflation - The occlusion balloon is inflated to occlude the descending thoracic aorta. This creates a closed compartment: the aortic arch is now isolated proximally.
-
Perfusate preparation and oxygenation - Oxygenated blood (FWB, packed RBCs, or HBOC-201) is prepared. If using stored blood, calcium gluconate is added to the perfusion circuit.
-
Infusion of oxygenated perfusate - Oxygenated blood or HBOC is infused through the central lumen of the catheter into the aortic arch under pressure. The aortic valve (if competent) prevents reflux into the LV, directing flow to the coronary ostia and arch vessels.
-
Continue CPR or support spontaneous cardiac activity - SAAP does not replace mechanical chest compressions; these are continued alongside perfusion until ROSC is achieved.
-
Defibrillation as needed - Ventricular fibrillation may occur and respond to defibrillation once myocardial oxygen delivery is restored.
-
Transition to ECMO if prolonged support needed - If ROSC is not achieved quickly or if prolonged extracorporeal perfusion is required, full ECMO can follow SAAP using the same vascular access.
-
Optional: Coronary catheterization through SAAP catheter - The 2023 cadaveric study (Marsden et al.) demonstrated feasibility of passing a 5 Fr coronary guiding catheter through the SAAP central lumen to cannulate the left coronary system - a potential conduit for salvage PCI at the resuscitation phase.
Perfusate Options: Evidence Summary
| Perfusate | ROSC Rate (swine HiTCA model) | Notes |
|---|---|---|
| Fresh whole blood (FWB) | 100% | Gold standard; logistically challenging prehospital |
| HBOC-201 | 86% | No significant difference vs FWB (p=0.483); logistically superior for field use |
| Stored blood (citrated) | High - with calcium co-infusion | Calcium gluconate co-administration is mandatory |
| Perflubron emulsion | Studied (1997) | Oxygen-carrying PFC; no longer in active development |
- Survival to 320 minutes was 92% (FWB) vs 67% (HBOC-201) - not statistically significant (p=0.12), with small animal numbers. (Hoops et al., J Trauma 2019, PMID 31348400)
- Transition from SAAP to ECLS post-SAAP was feasible in 100% of animals in both groups.
SAAP vs. REBOA vs. ECPR: Where Does It Fit?
| Feature | REBOA | SAAP | ECPR |
|---|---|---|---|
| Aortic occlusion | Yes | Yes | No |
| Active perfusion | No | Yes (arch only) | Yes (full circuit) |
| Oxygenator required | No | Yes | Yes |
| Coronary/cerebral perfusion | Passive (CPR-dependent) | Active, direct | Active, full |
| Technical complexity | Moderate | High | Very High |
| Applicable in cardiac arrest | Adjunct | Yes | Yes |
| Bridge potential | Yes | Yes | Yes |
| Prehospital feasibility | Possible | Emerging | Very limited |
Current State of Evidence & Human Data
- Evidence base is predominantly animal (swine) models - multiple studies from Manning et al. demonstrating high ROSC rates in HiTCA
- First-in-human data (cadaveric only, 2023): Marsden et al. demonstrated feasibility of catheter placement and coronary access in perfused cadavers - not live human patients (PMID 38087352)
- No live human clinical trials have been published to date
- A 2026 expert practice review in Emergency Medicine Journal (Adams et al., PMID 42062049) describes SAAP alongside REBOA and ECPR as part of the "endovascular resuscitation" framework that emergency physicians should understand and advocate for
The 2026 EMJ review explicitly states: "As leaders in resuscitation, it is essential that emergency physicians understand the principles and practice of endovascular techniques to advocate for the critically unwell patients that may benefit from EVR."
Key Pearls for the Emergency Physician
-
Calcium is non-negotiable - If using citrate-anticoagulated stored blood as perfusate, you must co-infuse intra-aortic calcium gluconate. Omitting it causes refractory VF and failure of ROSC.
-
Oxygenate before infusing - The lungs are completely bypassed in cardiac arrest. Any perfusate must be pre-oxygenated via an external membrane oxygenator.
-
Balloon position is Zone I - The occlusion balloon sits in the descending thoracic aorta, proximal to (or at) the celiac axis, similar to REBOA Zone I. This is the same zone used for hemorrhagic shock.
-
Aortic valve competency matters - SAAP relies on a competent aortic valve to direct arch perfusion into the coronaries rather than into the LV. Significant aortic regurgitation would undermine effectiveness.
-
SAAP is a bridge, not a destination - Transition to ECMO/ECLS or damage control surgery is the goal. Use it to buy time for the definitive intervention.
-
HBOC-201 is the most practical prehospital perfusate - Fresh whole blood is logistically complex outside of military/trauma centers. HBOC-201 offers comparable ROSC rates in animal models.
-
Not yet clinical standard - As of 2026, SAAP remains investigational with no live human trials. It is described in Tintinalli's as an "advanced resuscitation technique available or practiced in some settings" alongside ECMO.
References
- Tintinalli's Emergency Medicine: A Comprehensive Study, Box 2 (Selective Aortic Arch Perfusion), p. 205
- Manning JE et al. "Selective aortic arch perfusion during cardiac arrest: a new resuscitation technique." Ann Emerg Med 1992 (PMID 1514716) - original description
- Manning JE et al. "Aortic Hemostasis and Resuscitation...intra-aortic calcium coadministration." Acad Emerg Med 2016 (PMID 26766760) - calcium requirement established
- Hoops HE, Manning JE et al. "SAAP with fresh whole blood or HBOC-201." J Trauma Acute Care Surg 2019 (PMID 31348400) - FWB vs HBOC-201, ECLS transition
- Marsden M, Barratt J, Manning J et al. "SAAP: a first-in-human observational cadaveric study." Scand J Trauma Resusc Emerg Med 2023 (PMID 38087352) - first human feasibility data
- Adams TD, Barratt J, Manning JE et al. "Endovascular resuscitation: an expert practice review." Emerg Med J 2026 (PMID 42062049) - current framework for EPs
- Iida A et al. "State-of-the-art methods...SAAP and EPR." Acute Med Surg 2021 (PMID 33791103)
CASA ( CARDIAC ARREST SONOGRAPHIC ASSESSMENT)
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.