Drug induced parkinsonism from godmen gillmen
Reading File
Finding Sources
Finding Sources
Searching the Web
drug induced parkinsonism causes mechanism treatment 2024
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full answer.
Note: "Godmen gillmen" appears to be a phonetic mis-transcription of Goodman & Gilman's (the classic pharmacology textbook). The answer below synthesizes content from Bradley & Daroff's Neurology, Kaplan & Sadock's Comprehensive Textbook of Psychiatry, Stahl's Essential Psychopharmacology, Goldman-Cecil Medicine, and current literature.
Drug-Induced Parkinsonism (DIP)
Definition
Drug-induced parkinsonism is a reversible syndrome of bradykinesia, rigidity, and tremor caused by pharmacologic agents that reduce nigrostriatal dopamine activity. It is one of the most common causes of secondary parkinsonism and accounts for approximately 20% of all Parkinson-like conditions encountered in clinical practice.
Pathophysiology
DIP results from a decrease in nigrostriatal dopamine activity via several mechanisms:
| Mechanism | Examples |
|---|---|
| D2 receptor blockade | Typical antipsychotics (haloperidol, fluphenazine), atypical antipsychotics |
| Presynaptic dopamine depletion | Reserpine, tetrabenazine, deutetrabenazine, valbenazine |
| Calcium channel blockade (atypical) | Cinnarizine, flunarizine (not marketed in US) |
| Other mechanisms | Methyldopa, SSRIs, lithium, valproic acid, phenytoin |
The dopamine deficiency in the striatum (especially putamen) mimics the same motor circuit dysfunction seen in idiopathic Parkinson disease, which is why the clinical presentations are indistinguishable.
From Stahl's Essential Psychopharmacology: DIP caused by D2 blockers is maximally reduced when the agent also has both 5HT2A and alpha-1 antagonist properties, because blocking these receptors disinhibits dopamine release into the motor striatum. The lowest incidence of DIP is seen with agents having robust alpha-1 and 5HT2A antagonism: brexpiprazole, quetiapine, clozapine, and iloperidone.
Causative Drugs
Most Common Causes
- Typical (first-generation) antipsychotics - haloperidol, fluphenazine, perphenazine, chlorpromazine (high-potency > low-potency agents)
- Antidopaminergic antiemetics - metoclopramide, prochlorperazine
- Dopamine-depleting agents - reserpine, tetrabenazine, deutetrabenazine, valbenazine
Atypical Antipsychotics (ranked by DIP risk, highest to lowest):
Risperidone = Ziprasidone > Olanzapine > Quetiapine > Clozapine
This ranking directly reflects their relative D2 receptor affinity.
Other Drugs Associated with DIP
- SSRIs (selective serotonin reuptake inhibitors)
- Lithium
- Valproic acid
- Phenytoin
- Methyldopa
- Aripiprazole and newer atypical neuroleptics
- Calcium channel blockers: flunarizine, cinnarizine
Clinical Features
The classic triad mirrors idiopathic Parkinson disease:
- Muscular rigidity - either "lead pipe" (continuous) or "cogwheel" (ratchet-like, discontinuous)
- Akinesia/bradykinesia - psychomotor retardation, masked facies, shuffling gait, decreased arm swing, slowed speech, micrographia
- Resting tremor - rhythmic 3-6 Hz oscillations, can be unilateral or symmetrical, affecting head, tongue, jaw, limbs
Key distinguishing features vs. idiopathic PD:
- Signs are usually symmetrical in DIP (asymmetric in idiopathic PD)
- Tremor is more often postural than classic resting tremor in DIP
- Positive glabella tap sign on examination
- History of offending drug exposure
Earliest signs may be subtle: diminished arm swing or decreased facial expressiveness.
Onset and Time Course
- Typically appears subacutely after weeks to months of therapy (commonly within the first 5 to 30 days for antipsychotics)
- Can appear after dose increase or after reduction of antiparkinsonian agents
- Only 1 of the 3 cardinal features is required for diagnosis
Risk Factors
- Increasing age (incidence higher in those >60 years)
- Higher drug dose
- Female sex (women more susceptible than men)
- Pre-existing history of parkinsonism
- Underlying basal ganglia damage
Relationship to Idiopathic Parkinson Disease
- The clinical presentation of antipsychotic-induced parkinsonism and idiopathic PD are indistinguishable - patients with subclinical PD often worsen dramatically on antipsychotics
- Patients taking neuroleptics may be 5 times more likely to eventually start antiparkinsonian medications than non-users
- If symptoms do not resolve after drug discontinuation, the drug likely unmasked underlying PD
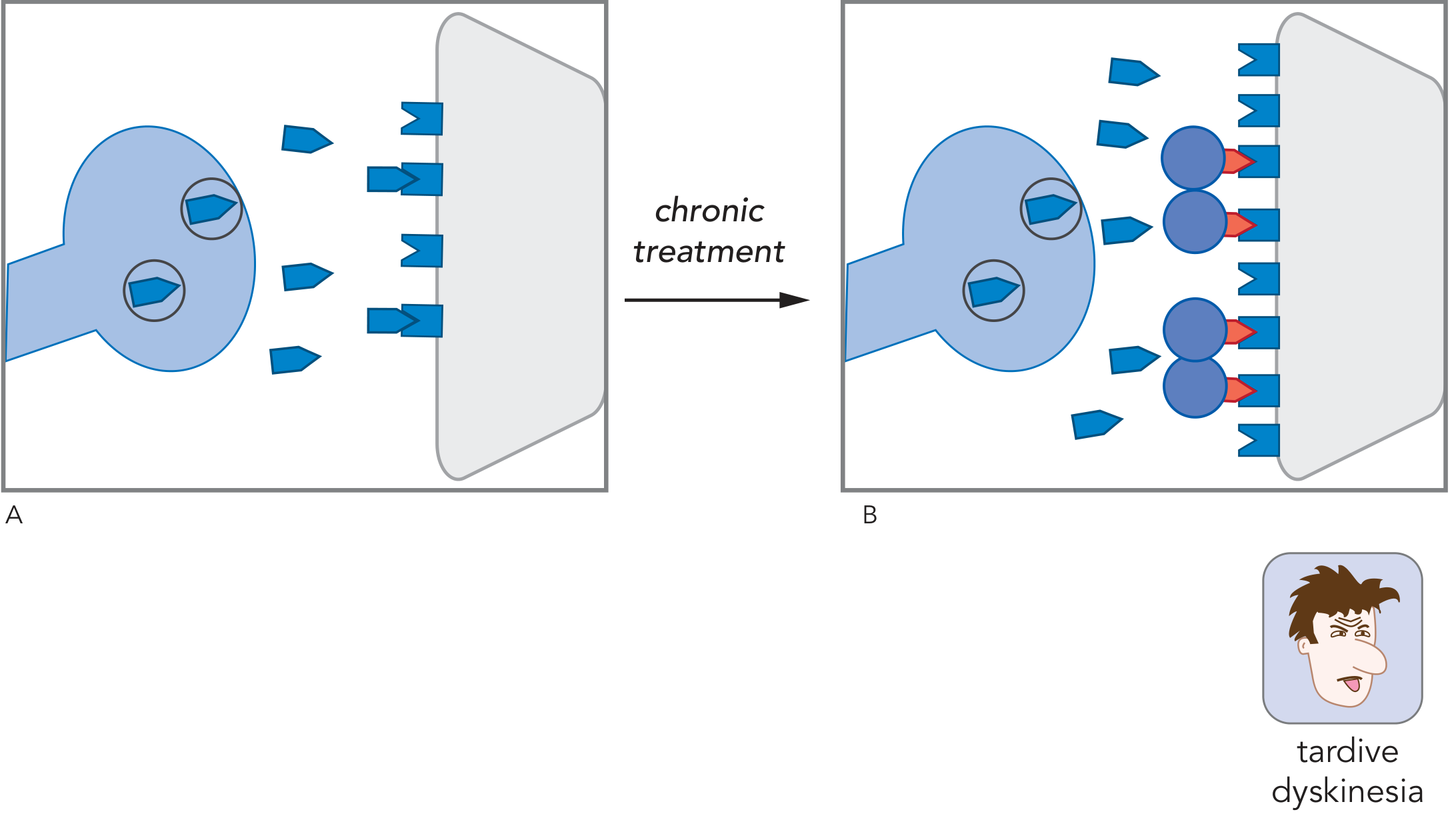
- Occasionally, discontinuing the offending dopamine receptor blocker causes tardive dyskinesia to emerge
- CSF levels of dopamine catabolites are reduced in both idiopathic PD and DIP
Treatment
Step 1 - Drug modification (preferred):
- Reduce dose or discontinue the offending agent
- Switch from high-potency D2 blocker (e.g., fluphenazine) to:
- Lower-potency FGA (e.g., perphenazine), or
- SGA such as quetiapine, lumateperone, or aripiprazole (partial D2/D3 agonists)
Step 2 - Pharmacological management (if drug cannot be stopped):
| Drug | Dose | Class |
|---|---|---|
| Benztropine (Cogentin) | 2-8 mg/day in divided doses | Anticholinergic |
| Trihexyphenidyl (Artane) | 6-10 mg/day in divided doses | Anticholinergic |
| Diphenhydramine (Benadryl) | 25-100 mg/day in divided doses | Antihistamine/anticholinergic |
| Amantadine (Symmetrel) | 100-300 mg/day in divided doses | Dopamine agonist (preferred in elderly or if anticholinergics not tolerated) |
- Anticholinergics work by restoring the dopamine-acetylcholine balance in the basal ganglia
- Levodopa and dopamine agonists can also improve most features, though may be less effective for severe neuroleptic-induced tremor
- Preliminary data also support oral DHEA as adjunctive therapy
Prognosis:
- Usually resolves with drug cessation, but may take up to 6 months for full resolution
- Once EPS are controlled, gradual withdrawal of antiparkinsonian medications can be attempted without EPS recurrence in some patients
Summary Table
| Feature | Drug-Induced Parkinsonism | Idiopathic PD |
|---|---|---|
| Symmetry | Usually bilateral/symmetrical | Usually asymmetric |
| Tremor type | Mostly postural | Resting ("pill-rolling") |
| Reversibility | Usually reversible | Progressive |
| Drug history | Yes (causative agent present) | No |
| Response to stopping drug | Improves (within weeks-months) | No change |
Sources: Bradley and Daroff's Neurology in Clinical Practice; Kaplan & Sadock's Comprehensive Textbook of Psychiatry; Stahl's Essential Psychopharmacology; Goldman-Cecil Medicine; Textbook of Family Medicine 9e.
Importance of centrally acting anticholinergic in par- Parkinson's.
Finding Sources
Finding Sources
Reading File
Finding Sources
Searching the Web
centrally acting anticholinergic drugs Parkinson disease mechanism importance trihexyphenidyl benztropine
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have all the content needed. Here is the complete, well-structured answer.
Centrally Acting Anticholinergics in Parkinson's Disease
The Core Concept: Dopamine-Acetylcholine Balance
The fundamental rationale for using anticholinergics in Parkinson's disease rests on a reciprocal balance between dopamine and acetylcholine in the striatum.
In the normal striatum:
- Dopaminergic neurons from the substantia nigra project to the striatum and act on D2 receptors to inhibit acetylcholine release from cholinergic interneurons
- This normally maintains a balance between the inhibitory dopaminergic input and the excitatory cholinergic discharge
In Parkinson's disease (or drug-induced parkinsonism):
- Dopaminergic neurons are lost (idiopathic PD) OR dopamine is blocked/depleted (DIP)
- Without dopamine's inhibitory effect, cholinergic interneurons are disinhibited - acetylcholine release increases unchecked
- This relative cholinergic excess over dopamine leads to the motor symptoms: tremor, rigidity, bradykinesia, and akinesia
As Ganong's Physiology states: "An important consideration in Parkinson disease is the balance between the excitatory discharge of cholinergic interneurons and the inhibitory dopaminergic input in the striatum. Some improvement is produced by decreasing the cholinergic influence with anticholinergic drugs."
Why "Centrally Acting" is Essential
The key word is centrally acting. These drugs must cross the blood-brain barrier (BBB) to work in the striatum. Peripheral anticholinergics (e.g., propantheline) do not cross the BBB and therefore provide no benefit in Parkinson's. Only agents with CNS penetrance can block the striatal muscarinic receptors that drive the motor symptoms.
The beneficial effect is specifically mediated by CNS muscarinic receptor blockade - particularly the M1 subtype, which is the most abundant in the neocortex, neostriatum, and hippocampus, and the M4 receptor, which is predominantly present in the neostriatum. - Kaplan & Sadock's Comprehensive Textbook of Psychiatry
Mechanism at the Circuit Level (Stahl's)
From Stahl's Essential Psychopharmacology:
Dopamine neurons in the nigrostriatal motor pathway make postsynaptic connections on cholinergic interneurons. Dopamine acting at D2 receptors normally inhibits acetylcholine release from postsynaptic nigrostriatal cholinergic neurons. When D2 blockers are given (or dopamine neurons are lost), dopamine can no longer suppress acetylcholine release, thus disinhibiting acetylcholine release. This leads to more excitation of postsynaptic muscarinic M1 receptors on medium spiny GABAergic neurons, which inhibits movements, producing akinesia, bradykinesia, rigidity, and tremor.When this enhanced acetylcholine release is blocked by anticholinergics at muscarinic receptors, this restores in part the normal balance between dopamine and acetylcholine and reduces DIP.
Drugs - The Key Agents
| Drug | Trade Name | Notes |
|---|---|---|
| Trihexyphenidyl (benzhexol) | Artane | Substituted piperidine; direct spasmolytic action; 6-10 mg/day in divided doses; FDA approved since 2003 |
| Benztropine mesylate | Cogentin | Combines benzhydryl + tropane; more anticholinergic than trihexyphenidyl, less antihistaminic than diphenhydramine; 2-8 mg/day; also used IM/IV for acute dystonia |
| Procyclidine | Kemadrin | Synthetic antispasmodic; 2.5 mg/day up to 30 mg/day; some find fewer side effects than other agents |
| Biperiden | Akineton | Analog of trihexyphenidyl; greater anticholinergic activity |
| Diphenhydramine | Benadryl | Antihistamine with anticholinergic properties; 25-100 mg/day; IM form (25-50 mg) used for acute dystonia prophylaxis |
Clinical Indications in Parkinsonism
- Drug-induced parkinsonism (DIP) - when the offending antipsychotic cannot be stopped
- Idiopathic Parkinson's disease - as adjunctive therapy, especially for tremor and drooling (less effective for bradykinesia/rigidity compared to levodopa)
- Postencephalitic parkinsonism
- Acute dystonic reactions - benztropine IM/IV is highly effective
- Akathisia - partial benefit
- Combined with levodopa - can have a more effective response than either alone in idiopathic PD
These drugs are less effective than levodopa for overall motor symptoms, but are particularly useful for tremor and when dopaminergic therapy is not yet required or not tolerated.
Advantages Over Levodopa (In Specific Contexts)
- No "on-off" phenomenon
- No dyskinesias
- Useful when tremor is the predominant symptom and rigidity/bradykinesia are mild
- Can be used when levodopa is not yet indicated (early disease with mainly tremor)
- Useful in drug-induced parkinsonism where you cannot simply give more dopamine
Adverse Effects (Why Caution is Required)
Central (CNS) Effects
- Cognitive impairment and memory loss - via M1/M2/M4 blockade in hippocampus and neocortex
- Anticholinergic delirium - especially in elderly
- Worsening psychosis in acutely ill schizophrenic patients
- May worsen tardive dyskinesia (TD) - anticholinergics shift the DA-ACh balance further toward dopamine dominance, potentially worsening TD; the incidence of TD is higher when both neuroleptic and anticholinergic medications are co-administered
Peripheral Effects (classic anticholinergic)
- Dry mouth (xerostomia)
- Blurred vision / cycloplegia
- Urinary retention
- Constipation
- Tachycardia
- Decreased sweating (risk of heat stroke)
Goodman & Gilman's: "Elderly patients are at greatest risk for parkinsonism and are most sensitive to the cognitive and peripheral adverse effects of anticholinergic antiparkinsonian medications."
Contraindications
| Condition | Reason |
|---|---|
| Narrow-angle (closed-angle) glaucoma | Can precipitate acute angle-closure attack by pupil dilation |
| Benign prostatic hyperplasia (BPH) | Urinary retention |
| Obstructive GI disorders / paralytic ileus / ulcerative colitis | Reduces gut motility |
| Dementia / cognitive impairment | Worsens cognition significantly |
| Tardive dyskinesia | May worsen TD; avoid if possible in long-term neuroleptic users |
Important Pharmacokinetic Note
The anticholinergic activity is independent of serum drug levels because levels vary up to 100-fold. A threshold serum level for anticholinergic activity exists - once achieved, EPS are unlikely to occur. The reduction in EPS is NOT related to the dose of the anticholinergic or the dose of the antipsychotic, but only to the achieved serum level of anticholinergic activity. - Kaplan & Sadock's
Summary: Why Centrally Acting Anticholinergics Matter in Parkinson's
- Mechanism: Restore the dopamine-acetylcholine balance in the striatum by blocking M1 muscarinic receptors on medium spiny neurons, reducing cholinergic overactivity caused by dopamine deficiency
- Efficacy: Best for tremor and drooling; less effective than levodopa for bradykinesia/rigidity
- Unique role: The only oral option when DIP cannot be reversed by stopping the causative drug; also useful for acute dystonia (IM/IV)
- Limitation: Cognitive side effects limit their use in elderly patients and those with dementia - in these populations, amantadine is preferred over anticholinergics
- Risk: Prolonged use alongside neuroleptics may increase the risk of TD development, so they should be minimized or avoided in long-term neuroleptic therapy
Sources: Stahl's Essential Psychopharmacology; Kaplan & Sadock's Comprehensive Textbook of Psychiatry; Katzung's Basic and Clinical Pharmacology 16e; Goodman & Gilman's Pharmacological Basis of Therapeutics; Ganong's Review of Medical Physiology 26e; Bradley and Daroff's Neurology in Clinical Practice.
This is a shared conversation. Sign in to Orris to start your own chat.