Obstructive lung disease long answer questions according to Robbins and flow chart
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have all the key content and images from Robbins. Let me compile the comprehensive long-answer notes with flowcharts.
Obstructive Lung Disease - Long Answer Questions (Robbins Pathology)
OVERVIEW
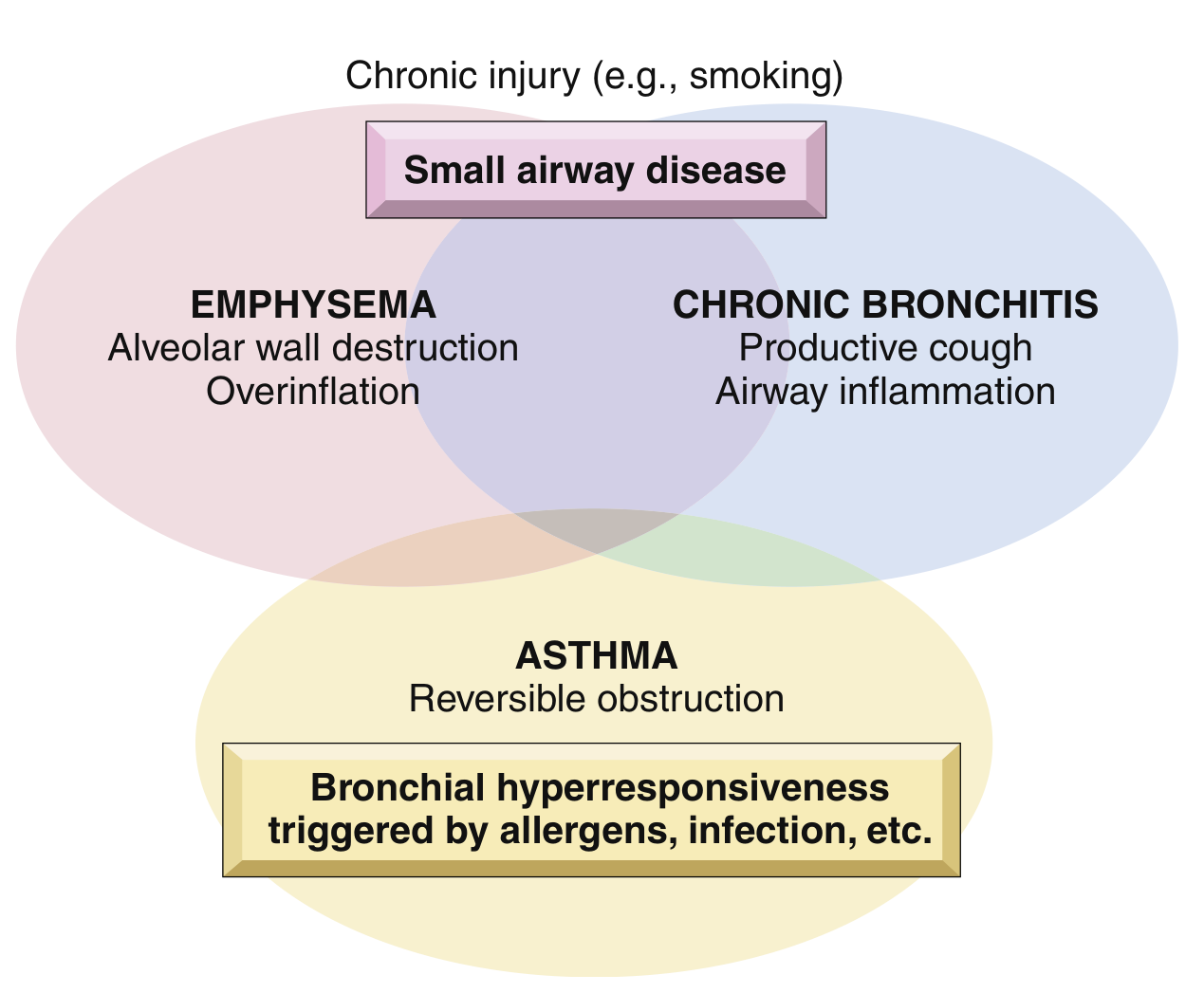
Obstructive Lung Disease (OLD) refers to a group of conditions characterized by increased resistance to airflow due to partial or complete obstruction at any level of the bronchial tree. The major entities are:
- Emphysema
- Chronic Bronchitis (together forming COPD)
- Asthma
- Bronchiectasis
FLOWCHART 1 - Classification of Obstructive Lung Diseases
OBSTRUCTIVE LUNG DISEASE
|
_____|_____________________
| |
COPD OTHER
| |
__|__________ ____|______
| | | |
Emphysema Chronic Asthma Bronchiectasis
Bronchitis
| |
Acinar Mucus gland
destruction hypertrophy
(permanent) + hypersecretion
1. CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD)
Definition (WHO): "A common, preventable and treatable disease characterized by persistent respiratory symptoms and airflow limitation due to airway and/or alveolar abnormalities caused by exposure to noxious particles or gases."
Epidemiology:
- Affects >10% of U.S. adults over age 40
- 4th leading cause of death in the USA; 3rd worldwide
- 35-50% of heavy smokers develop COPD
- ~80% of COPD is attributable to smoking
- Women appear more susceptible than men
Risk Factors:
- Cigarette smoking (primary)
- Poor lung development early in life
- Environmental/occupational pollutants
- Airway hyperresponsiveness
- Genetic polymorphisms (e.g., alpha-1 antitrypsin deficiency)
2. EMPHYSEMA
Definition
Emphysema is characterized by permanent enlargement of the air spaces distal to the terminal bronchioles, accompanied by destruction of their walls but without significant fibrosis.
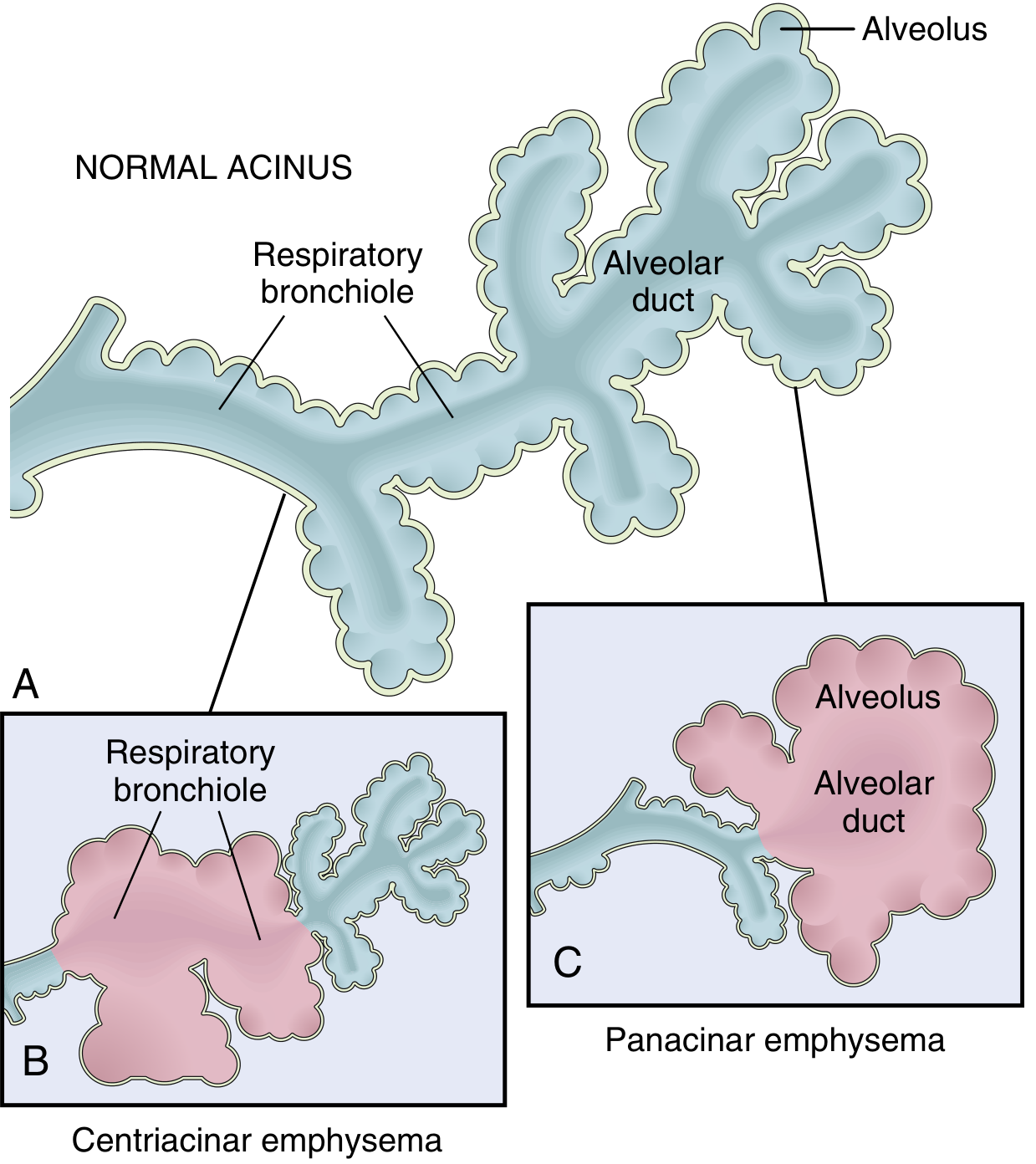
Classification (4 Types)
| Type | Distribution | Association |
|---|---|---|
| Centriacinar (Centrilobular) | Central/proximal parts of acini; distal alveoli spared | Cigarette smoking (most common); upper lobes |
| Panacinar (Panlobular) | Uniform enlargement from respiratory bronchiole to terminal alveoli | Alpha-1 antitrypsin deficiency; lower lobes |
| Distal Acinar (Paraseptal) | Distal part of acinus; near pleura, septa, margins | Young adults; spontaneous pneumothorax; bullae |
| Irregular | Acinus irregularly involved; associated with scarring | Clinically insignificant |
Only centriacinar and panacinar types are associated with COPD. Centriacinar is ~20x more common.
FLOWCHART 2 - Pathogenesis of Emphysema
Cigarette Smoke / Noxious Stimuli
|
v
Recruitment of Neutrophils & Macrophages
|
_________|_________
| |
Elastase Oxidants (ROS)
(Neutrophil) |
| v
| Inactivate
| Alpha-1 Antitrypsin (AAT)
| |
|_________________|
|
v
IMBALANCE: Protease >> Antiprotease
|
v
Destruction of Elastin in Alveolar Wall
|
v
Permanent Air Space Enlargement
(Loss of elastic recoil)
|
v
Air Trapping → Hyperinflation → EMPHYSEMA
Key Mechanism - Protease-Antiprotease Hypothesis:
- Smoking attracts neutrophils/macrophages → release elastase and other proteases
- Smoking also generates ROS that inactivate alpha-1 antitrypsin (AAT), the main inhibitor of elastase
- In AAT deficiency: even without smoking, uncheck elastase destroys alveolar walls → panacinar emphysema
Morphology
- Gross: Pale, voluminous lungs; may not deflate on opening chest; bullae in distal/paraseptal type
- Microscopic: Enlargement and destruction of air spaces; thinning/loss of alveolar walls; reduction in capillary bed
Clinical Features
- Progressive dyspnea (main symptom)
- Barrel-chest, pursed-lip breathing, use of accessory muscles
- "Pink Puffer" phenotype (predominantly emphysema): thin, dyspneic, maintain normal PaO2 by hyperventilation
- PFTs: ↓ FEV1, ↓ FEV1/FVC, ↑ TLC, ↑ RV, ↓ DLCO
- CXR: Hyperinflation, flattened diaphragm, increased AP diameter
3. CHRONIC BRONCHITIS
Definition (Clinical)
Chronic bronchitis is defined clinically as a persistent productive cough for at least 3 consecutive months in at least 2 consecutive years, after other causes of chronic cough are excluded.
Pathogenesis
Cigarette Smoke / Irritants
|
v
Hypertrophy of Mucus-Secreting Glands
+ Goblet Cell Metaplasia
|
v
Excess Mucus Production
|
v
Mucociliary Clearance Impaired
|
_____|_____
| |
Mucus plug Secondary
obstruction Bacterial
Infection
|
v
Chronic Airway Inflammation
(neutrophils, macrophages, lymphocytes)
|
v
Small Airway Disease (bronchiolitis)
|
v
Airflow Obstruction
Morphology
- Gross: Hyperemic, swollen mucosa; mucus hypersecretion; luminal narrowing
- Microscopic:
- Hypertrophy of submucosal glands (increased Reid Index - ratio of gland layer to bronchial wall thickness; normally < 0.4; in chronic bronchitis > 0.5)
- Goblet cell metaplasia of surface epithelium
- Inflammatory infiltrate (neutrophils, lymphocytes, macrophages) in airway wall
- Small airway disease: fibrosis, smooth muscle hypertrophy in bronchioles
Reid Index
- Normal: < 0.4
- Chronic Bronchitis: > 0.5 (increased due to mucous gland hypertrophy)
Clinical Features
- "Blue Bloater" phenotype (predominantly chronic bronchitis): obese, cyanotic, hypercapnic, hypoxemic, prone to cor pulmonale
- Frequent respiratory infections
- Hypoxia → polycythemia → cor pulmonale
- PFTs: ↓ FEV1/FVC; relatively normal TLC and RV (less air trapping than emphysema)
FLOWCHART 3 - Comparison: Emphysema vs. Chronic Bronchitis
Feature Emphysema ("Pink Puffer") Chronic Bronchitis ("Blue Bloater")
------------------ -------------------------- ------------------------------------
Mechanism Alveolar wall destruction Mucus hypersecretion + airway inflam.
Primary site Acini (distal airspace) Large + small airways
Definition basis Pathological Clinical
Morphology Enlarged air spaces Gland hypertrophy (Reid Index >0.5)
Body habitus Thin, barrel-chested Obese
Cyanosis Absent (late) Present early
PaO2 Relatively normal Reduced (hypoxemia)
PaCO2 Normal / slightly low Elevated (hypercapnia)
Cor pulmonale Late Early/common
Infections Less common Frequent
Sputum Minimal Copious purulent
Key test finding ↓ DLCO Normal/slightly ↓ DLCO
4. ASTHMA
Definition
Asthma is a chronic inflammatory disorder of the airways causing recurrent episodes of bronchospasm characterized by wheezing, breathlessness, chest tightness, and cough (particularly at night/early morning).
Hallmarks (Robbins)
- Intermittent, reversible airway obstruction
- Chronic bronchial inflammation with eosinophils
- Bronchial smooth muscle hypertrophy and hyperreactivity
- Increased mucus secretion
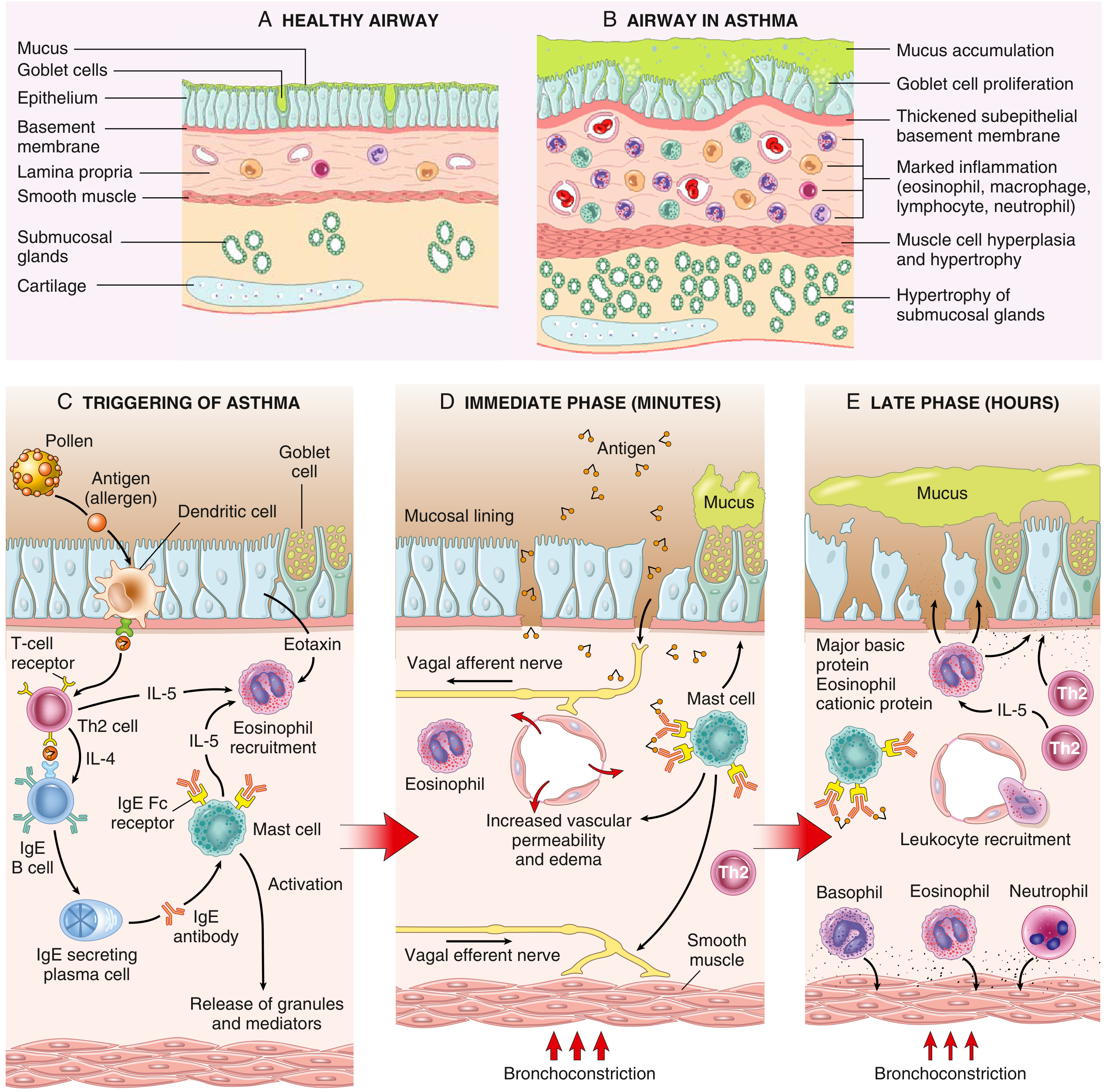
FLOWCHART 4 - Pathogenesis of Atopic (Allergic) Asthma
FIRST EXPOSURE TO ALLERGEN
|
v
Antigen processed by Dendritic Cells
|
v
Activation of Th2 CD4+ T cells
|
_________|___________________________
| | |
IL-4/IL-13 IL-5 Eotaxin
| | |
v v v
IgE Eosinophil Eosinophil
Production Activation Recruitment
by B cells
|
v
IgE binds Fc receptors on Mast Cells
SECOND EXPOSURE (Re-exposure to Allergen)
|
v
Allergen cross-links IgE on Mast Cells
|
_____|_________________________________________
| |
IMMEDIATE PHASE (minutes) LATE PHASE (hours)
| |
Mast cell degranulation Recruitment of eosinophils,
- Histamine neutrophils, basophils,
- Leukotrienes (LTC4, LTD4) Th2 cells, monocytes
- Prostaglandins (PGD2) |
- PAF, TNF Eosinophils release:
| - Major Basic Protein (MBP)
v - Eosinophil Cationic Protein (ECP)
Bronchoconstriction - Galectin-10 (Charcot-Leyden crystals)
Increased vascular permeability |
Mucus production v
Vagal reflex stimulation Airway Remodeling
(chronic changes)
Types of Asthma
| Type | Key Features |
|---|---|
| Atopic (Allergic) | Most common; IgE-mediated (Type I hypersensitivity); begins in childhood; positive skin test; triggered by allergens (pollen, dust, dander) |
| Nonatopic | No allergen sensitization; triggered by viral infections, cold air, exercise, irritants (SO2, ozone); negative skin test |
| Occupational | Triggered by fumes, dusts, organic/chemical compounds in workplace; may be IgE or non-IgE |
| Drug-induced | Aspirin-sensitive asthma: inhibition of COX → shunting to lipoxygenase → excess leukotrienes → bronchoconstriction |
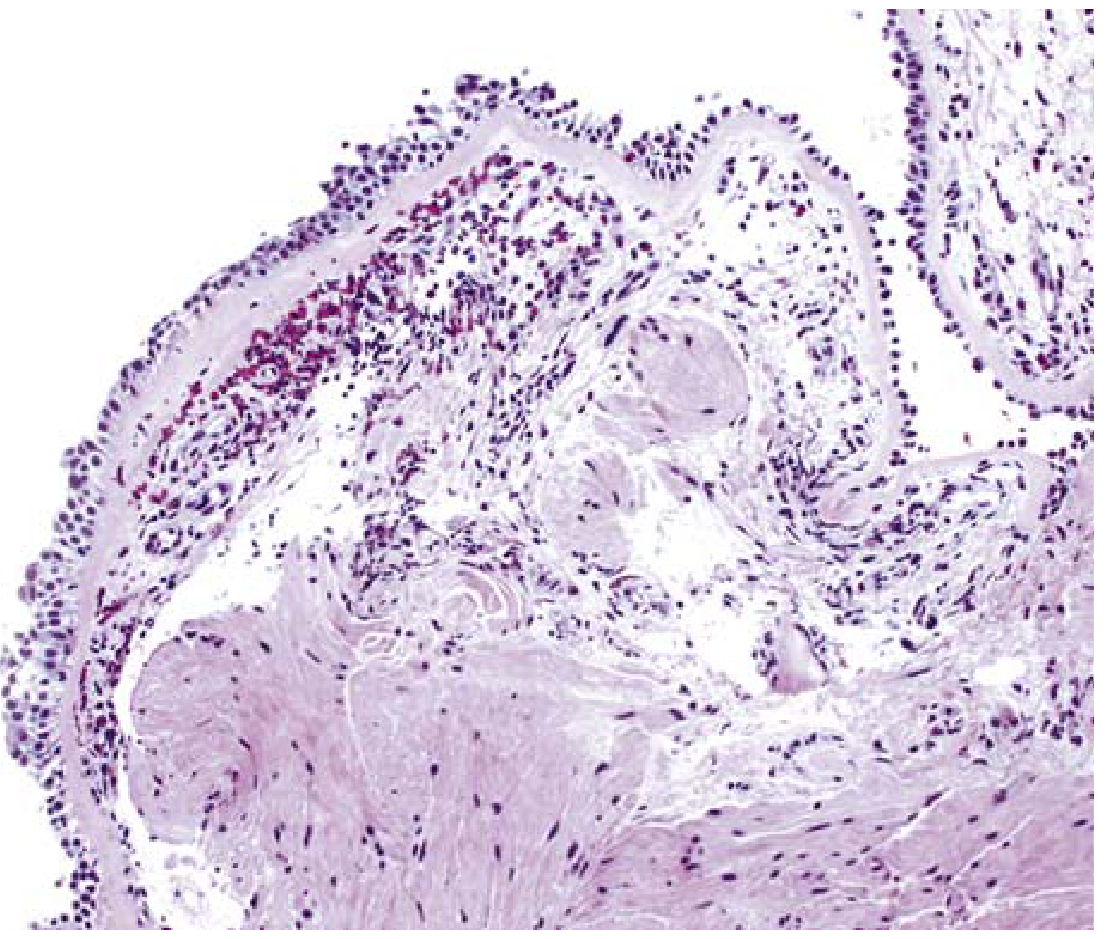
Morphology (Pathological Changes)
Gross (fatal cases):
- Lungs distended due to air trapping
- Occlusion of bronchi/bronchioles by thick mucous plugs containing Curschmann spirals (whorls of shed epithelium)
- Numerous eosinophils and Charcot-Leyden crystals (formed from galectin-10 released by eosinophils)
Microscopic - Airway Remodeling:
- Thickening of airway wall
- Subbasement membrane fibrosis
- Increased submucosal vascularity
- Hypertrophy of submucosal glands + goblet cell metaplasia
- Hypertrophy/hyperplasia of bronchial muscle
Clinical Features
- Episodic: severe dyspnea + wheezing (usually 1 to several hours)
- Between attacks: symptom-free (PFTs may still show subtle deficits)
- Status asthmaticus: severe attack unresponsive to therapy for days/weeks; hypercapnia, acidosis, severe hypoxia; potentially fatal
- PFTs during attack: ↓ FEV1, ↓ FEV1/FVC, ↑ TLC, ↑ RV (reversible with bronchodilators - key differentiator from COPD)
Treatment
- Mild: bronchodilators (beta-agonists) + glucocorticoids ± leukotriene inhibitors
- Severe/elevated eosinophils/high IgE: biologic agents targeting IL-4, IL-5, IgE (e.g., mepolizumab, omalizumab)
5. BRONCHIECTASIS
Definition
Bronchiectasis is the permanent dilation of bronchi and bronchioles caused by destruction of smooth muscle and supporting elastic tissue, typically resulting from or associated with chronic necrotizing infections.
Note: It is not a primary disorder - always secondary to persistent infection or obstruction.
Predisposing Conditions
CAUSES OF BRONCHIECTASIS
|
_______|_______________________________
| | |
Obstruction Congenital/ Necrotizing
Hereditary Infections
| | |
Tumors Cystic Fibrosis Staphylococcal
Foreign body (viscid mucus) Klebsiella
Mucus impaction Immunodeficiency Mycobacteria
(asthma, ABPA) (Ig deficiency) (TB)
Kartagener syndrome Fungal
(immotile cilia)
Young syndrome
Specific Causes:
- Bronchial obstruction: Tumors, foreign bodies, mucus impaction (asthma, chronic bronchitis)
- Congenital/hereditary:
- Cystic fibrosis (viscid mucus + secondary infections)
- Immunodeficiency states (Ig deficiencies)
- Kartagener syndrome (immotile cilia - defective ciliary motility)
- Young syndrome
- Postinfectious:
- Necrotizing pneumonias (Staphylococcus, Klebsiella, Mycobacterium, fungi, Aspergillus - ABPA)
- Measles, pertussis in children
FLOWCHART 5 - Pathogenesis of Bronchiectasis
Persistent Obstruction OR Necrotizing Infection
|
v
Impaired Mucociliary Clearance
|
v
Accumulation of Secretions / Infection
|
v
Cycle of Inflammation & Infection
|
v
Neutrophil recruitment → Protease release
|
v
Destruction of bronchial wall
(smooth muscle + elastic tissue)
|
v
PERMANENT DILATION of bronchi/bronchioles
|
v
Further impaired drainage → More infection
(vicious cycle)
Morphology
- Gross: Dilated bronchi up to 4x normal diameter; may extend to pleural surface; pus-filled airways; lower lobes involved (except TB - upper lobes)
- Microscopic:
- Intense acute and chronic inflammatory exudate within bronchial walls
- Desquamation of lining epithelium → ulceration
- Fibrosis of bronchial wall and peribronchial fibrosis
- In areas of fibrosis: atelectasis of surrounding lung
- Vascular changes: bronchial artery dilatation
Clinical Features
- Symptoms:
- Persistent cough with copious purulent, foul-smelling sputum (hallmark)
- Hemoptysis (sometimes the presenting feature)
- Recurrent fever, weight loss
- Progressive dyspnea
- Signs:
- Clubbing of fingers
- Coarse crackles on auscultation
- Cor pulmonale (in severe, long-standing disease)
- Complications:
- Cor pulmonale
- Secondary amyloidosis
- Metastatic brain abscess
- Empyema (if pleura involved)
- Diagnosis: HRCT chest (gold standard) - "tram-track" sign, signet ring sign
MASTER SUMMARY FLOWCHART - Obstructive Lung Disease
OBSTRUCTIVE LUNG DISEASE
|
|--- COPD (irreversible obstruction)
| |
| |--- EMPHYSEMA
| | Mechanism: Protease-antiprotease imbalance
| | Site: Alveoli (air space destruction)
| | Key: ↓ DLCO, Pink Puffer, ↑ TLC
| |
| |--- CHRONIC BRONCHITIS
| Mechanism: Mucus hypersecretion
| Site: Large airways (mucous glands)
| Key: Reid Index >0.5, Blue Bloater, Cor pulmonale
|
|--- ASTHMA (reversible obstruction)
| Mechanism: Th2/IgE → Mast cell → Bronchoconstriction
| Site: Bronchi + bronchioles
| Key: Eosinophils, reversible on bronchodilators
| Types: Atopic, Nonatopic, Occupational, Drug-induced
|
|--- BRONCHIECTASIS (permanent bronchial dilation)
Mechanism: Chronic infection/obstruction → wall destruction
Site: Bronchi/bronchioles
Key: Purulent copious sputum, clubbing, HRCT diagnosis
KEY DISTINGUISHING FEATURES TABLE
| Feature | Emphysema | Chronic Bronchitis | Asthma | Bronchiectasis |
|---|---|---|---|---|
| Definition basis | Pathological | Clinical | Clinical/Pathological | Pathological |
| Primary defect | Alveolar wall destruction | Mucus hypersecretion | Bronchospasm | Bronchial wall destruction |
| Obstruction type | Irreversible | Irreversible | Reversible | Irreversible |
| Key cells | Neutrophils, macrophages | Neutrophils, macrophages | Eosinophils, mast cells, Th2 | Neutrophils |
| Histology hallmark | Enlarged air spaces | ↑ Reid Index; goblet cell metaplasia | Subbasement membrane fibrosis; Curschmann spirals | Dilated bronchi, inflammatory exudate |
| Sputum | Minimal | Mucopurulent | Mucous plugs (Curschmann spirals) | Copious purulent/foul |
| Clubbing | Absent | Absent | Absent | Present |
| Main complication | Respiratory failure | Cor pulmonale | Status asthmaticus | Cor pulmonale, amyloidosis |
Source: Robbins & Kumar Basic Pathology (Robbins Pathology), 10th Edition, Chapter 11 - Lung, pp. 447-490
This is a shared conversation. Sign in to Orris to start your own chat.