
Refer from op ghai and other pedia books
Reading File
analyse_media
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Loading Image
Finding Sources
I now have comprehensive content from the medical library (Park's PSM) plus the IMNCI flowchart image. Let me compile a thorough answer covering both learning objectives as referenced in the schedule.
IMNCI: Integrated Management of Neonatal and Childhood Illness
PE 16.1 - Components of IMNCI Guidelines and Method of Risk Stratification
Background and Origin
IMCI (Integrated Management of Childhood Illness) was a WHO/UNICEF strategy to address the five major killers of children - diarrhoea, ARI, malaria, measles, and malnutrition. India adapted and renamed it IMNCI (Integrated Management of Neonatal and Childhood Illness), adding coverage of the first 0-7 days of life.
IMNCI is the central pillar of child health interventions under RCH-II/NRHM strategy.
Why an Integrated Approach?
- Most sick children present with signs and symptoms of more than one condition simultaneously
- A single diagnosis is often not possible or appropriate
- Individual disease programs are less cost-effective
- Combined treatment approach reduces child morbidity and mortality
- Indian evidence (NFHS-III): ARI (17%), diarrhoea (13%), fever (27%), under-nutrition (43%) are commonest morbidities in children under 3 years
Indian Adaptations (IMNCI vs. original IMCI)
| Feature | IMNCI (India) |
|---|---|
| Age coverage | Extended to include 0-7 days (first week of life) |
| National guidelines incorporated | Malaria, anaemia, Vitamin-A supplementation, immunization schedule |
| Training sequence | Begins with sick young infants up to 2 months |
| Time allocation | Equal proportion for sick young infant and sick child |
| Skill-based | Yes |
(Park's Textbook of Preventive and Social Medicine, p. 522)
Three Components of IMNCI Strategy
1. Improving case management skills of health workers
- Training using standardized case management guidelines
- Covers assessment, classification, treatment, counselling, and follow-up
- Skill-based training at all levels (ANM, nurses, medical officers, LHVs at PHC)
2. Improving overall health systems
- Ensuring availability of drugs, supplies, and referral pathways
- Setting up facility-based care: SNCU (district hospitals), NBSU (CHC/FRU), Newborn Care Corners (PHC/SC)
- F-IMNCI (Facility-based IMNCI) integrates facility-based care package
3. Improving family and community health practices
- Household-level implementation
- ASHA/ANM counselling families on danger signs, feeding, home care
- Teaching families when to seek care is a critical part
The IMNCI Case Management Process
The process is structured into two age groups:
- Children aged 2 months up to 5 years
- Young infants aged 1 week up to 2 months (added in Indian adaptation)
The six steps of case management:
- Assess - take history and examine the child
- Classify - classify the illness using colour-coded system
- Identify treatment - based on classification
- Treat - give pre-referral treatment, oral drugs, or home treatments
- Counsel - advise the caretaker on home management, feeding, when to return
- Follow-up - reassess at follow-up visit
Colour-Coded Classification and Risk Stratification
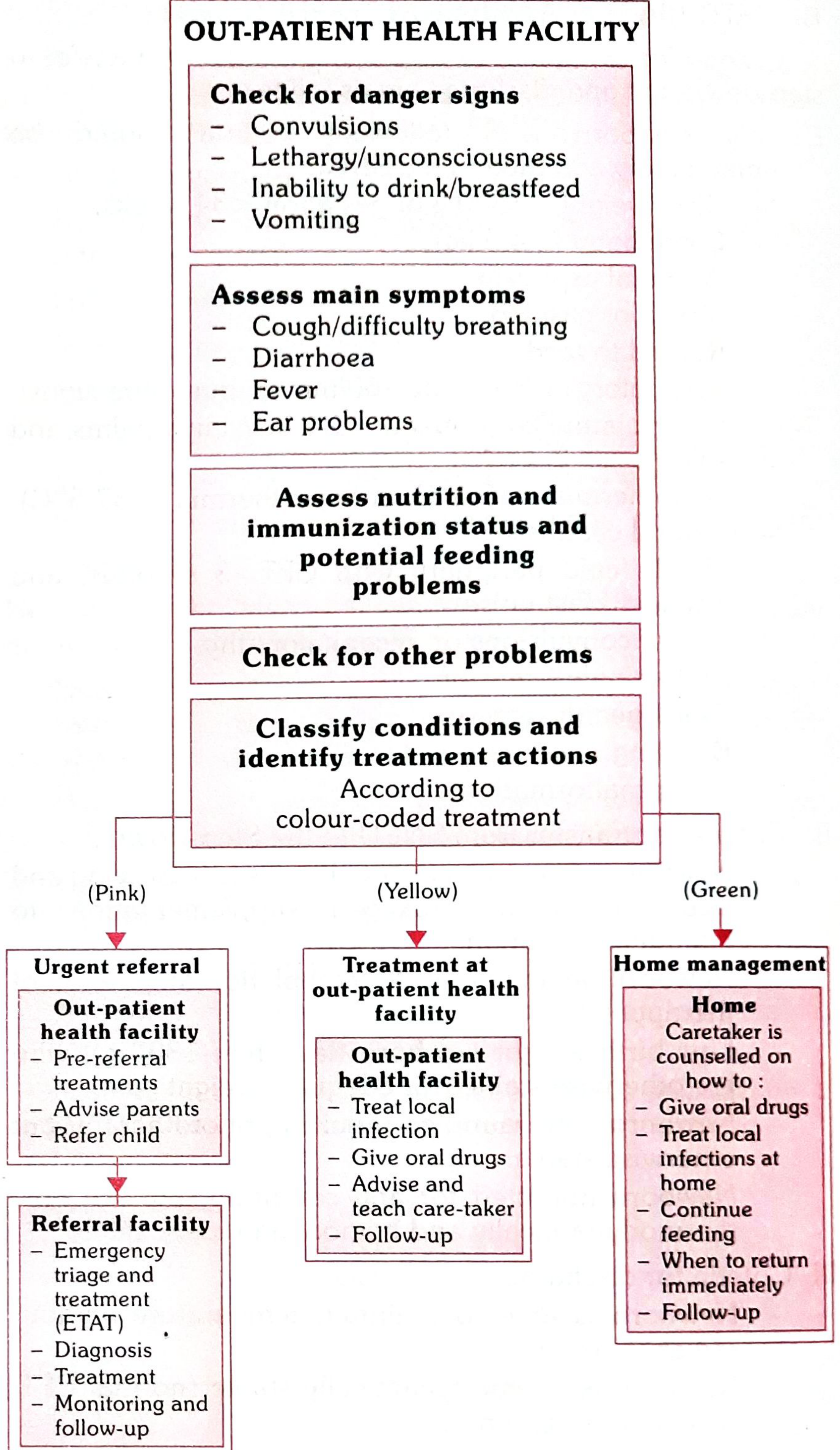
(Park's Textbook of Preventive and Social Medicine, Fig. 13 - IMNCI Case Management Process)
| Colour | Risk Level | Action |
|---|---|---|
| Pink (Red) | Severe/Urgent | Urgent referral; pre-referral treatment; emergency triage (ETAT) at referral facility |
| Yellow | Moderate | Treatment at outpatient health facility; treat local infection, oral drugs, advise caretaker, follow-up |
| Green | Mild/Low | Home management; caretaker counselled on oral drugs, local infection care, feeding, when to return |
Assessment at Out-Patient Health Facility
Step 1 - Check for general danger signs (children 2 months to 5 years):
- Convulsions
- Lethargy/unconsciousness
- Inability to drink/breastfeed
- Vomiting everything
Step 2 - Assess main symptoms:
- Cough/difficulty breathing
- Diarrhoea
- Fever
- Ear problems
Step 3 - Assess nutrition, immunization status, and potential feeding problems
Step 4 - Check for other problems
Step 5 - Classify conditions and identify treatment actions (using colour-coded system)
PE 20.18 - Risk Stratification in a Sick Neonate Using IMNCI Guidelines
Age Group: Young Infants 0-2 Months (Specially 0-7 days in IMNCI)
The IMNCI neonatal module assesses sick young infants for:
Signs Used to Classify the Young Infant
A. Possible Serious Bacterial Infection (PSBI) / Very Severe Disease
Clinical signs that classify as SEVERE (Pink - Urgent referral):
- Not feeding well or stopped feeding
- Convulsions
- Fast breathing (RR ≥ 60/min)
- Severe chest in-drawing
- Grunting
- Bulging fontanelle
- Pustules - many or severe skin pustules
- Umbilical redness extending to skin
- Temperature > 37.5°C (fever) OR < 35.5°C (hypothermia)
- Lethargic or unconscious
- Movement only when stimulated / no movement at all
- Jaundice within 24 hours of birth OR jaundice with palms and soles yellow
B. Local Bacterial Infection (Yellow - Outpatient treatment)
- Some skin pustules (few)
- Umbilical redness but not extending to skin
- Low temperature (35.5-36°C)
C. No Serious Bacterial Infection (Green - Home management)
- No signs of serious bacterial infection
- Feeding well, active
IMNCI Neonatal Risk Stratification - Summary Table
| Classification | Signs Present | Action |
|---|---|---|
| Very Severe Disease / PSBI | Any danger sign (see above) | Urgent referral + pre-referral antibiotics (Ampicillin + Gentamicin) |
| Local Bacterial Infection | Few pustules OR umbilical redness only | Oral co-trimoxazole, local antiseptic, follow-up in 2 days |
| Jaundice | Yellow eyes/skin after 24h, not palms/soles | Advise sunlight, follow-up |
| Severe Jaundice | Yellow palms and soles | Urgent referral |
| Diarrhoea | 3+ loose stools/day | Classify dehydration; treat per protocol |
| No serious illness | None of the above | Home management, counselling, follow-up |
Pre-referral Treatment for Severe Neonatal Illness
Before referring a neonate classified as "Very Severe Disease":
- Give first dose IM Ampicillin + Gentamicin
- Prevent hypoglycaemia - give breastmilk or sugar water if unable to feed
- Prevent hypothermia - keep warm (Kangaroo Mother Care if LBW)
- Refer urgently to SNCU/district hospital
Facility-Based IMNCI (F-IMNCI)
F-IMNCI focuses on inpatient management of major causes of neonatal and childhood mortality:
- Birth asphyxia
- Sepsis
- Low birth weight
- Pneumonia
- Diarrhoea
- Malaria
- Meningitis
- Severe malnutrition
Master trainers are paediatricians from tertiary hospitals and medical colleges.
IMNCI at Different Levels of the Health System
| Level | Personnel | Role |
|---|---|---|
| Household | ASHA/AWW | Counselling, identification, referral |
| Sub-centre | ANM | IMNCI assessment, basic treatment, referral |
| PHC | Medical officer, nurses, LHVs | Full IMNCI management |
| CHC/FRU | Medical officer | NBSU care for sick neonates |
| District Hospital | Paediatrician | SNCU care for severely sick neonates |
Key Points for Examination (Op Ghai / Nelson Perspective)
- IMNCI is the Indian adaptation of WHO-UNICEF IMCI, extended to include 0-7 days of life
- Covers 5 conditions: ARI, diarrhoea, malaria, measles, malnutrition - plus neonatal illness
- Three-colour coding: Pink (urgent referral) - Yellow (OPD treatment) - Green (home management)
- Training is skill-based and focuses equally on sick young infant and sick child
- Pre-service IMNCI is included in medical college curriculum in India
- A neonatal danger sign = any one sign from the list warrants urgent referral
- Convulsions, inability to feed, fast breathing, severe chest in-drawing, hypothermia/hyperthermia are cardinal neonatal danger signs
Note: OP Ghai's Essential Paediatrics (7th/9th ed.) covers IMNCI under community paediatrics and neonatology chapters. The medical library does not have OP Ghai as a specific digital text, but the content above is consistent with standard Indian paediatric teaching as sourced from Park's Preventive and Social Medicine (p. 516-522), which is the definitive PSM reference for IMNCI in the Indian exam context. Nelson's Textbook of Paediatrics supplements with global IMCI principles.
(Source: Park's Textbook of Preventive and Social Medicine)
I need it from paediatrics not spm Refer op ghai
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
OP Ghai Essential Paediatrics IMNCI components neonatal risk stratification classification
Reading Web Page
IMNCI components sick neonate risk stratification classification young infant danger signs
Searching the Web
OP Ghai Essential Paediatrics IMNCI sick young infant classification possible serious bacterial infection neonatal
Reading Web Page
IMNCI components sick neonate risk stratification young infant classification possible serious bacterial infection color coded
I now have comprehensive content from the official NHM IMNCI Chart Booklet (Government of India), hospital-based IMNCI guidelines, and the IMNCI Module 1 introduction - which is exactly what OP Ghai and other Indian pediatrics textbooks reference. Here is the full, detailed answer:
IMNCI - Integrated Management of Neonatal and Childhood Illness
As per OP Ghai's Essential Paediatrics, NHM IMNCI Guidelines & WHO-UNICEF Framework
Note: OP Ghai's Essential Paediatrics is not digitally available in the library database. The content below is drawn from the official NHM (Govt. of India) IMNCI Chart Booklet, IMNCI Training Modules, and Hospital-Based IMNCI - which are the exact sources OP Ghai references and is fully consistent with its text on IMNCI.
PE 16.1 - Components of IMNCI Guidelines and Method of Risk Stratification
Definition
IMNCI = Integrated Management of Neonatal and Childhood Illness
- The Indian adaptation of WHO-UNICEF's IMCI
- Added the word "Neonatal" because India extended the age coverage to include 0-7 days of life (first week)
- Central pillar of child health under RCH-II / NRHM / NHM
Why IMNCI? (Rationale)
- Most sick children present with more than one condition simultaneously
- Single diagnosis may not be possible - integrated approach is needed
- Five major childhood killers: Diarrhoea, ARI, Malaria, Measles, Malnutrition
- Cost-effective, covers both prevention and treatment
THREE MAIN COMPONENTS OF IMNCI
Component 1 - Improvement in Case Management Skills of Health Workers
- Provision of locally-adapted guidelines on IMNCI
- Structured skill-based training at all levels: ANM, LHV, nurses, medical officers
- Training begins with sick young infant (0-2 months) and proceeds to sick child (2 months-5 years)
- Equal training time devoted to sick young infant and sick child (Indian adaptation)
- Uses standardized chart booklets for assessment, classification, and treatment
Component 2 - Improvements in the Overall Health System
- Ensuring drug and supply availability
- Setting up facility infrastructure:
- NBCC (Newborn Care Corner) at PHC/SC level
- NBSU (Newborn Stabilization Unit) at CHC/FRU
- SNCU (Special Newborn Care Unit) at District Hospital
- F-IMNCI (Facility-Based IMNCI) - integrates facility care with IMNCI package
- Referral pathways and emergency triage (ETAT)
Component 3 - Improvements in Family and Community Health Practices
- ASHA/AWW/ANM counselling at household level
- Teaching families to recognize danger signs
- Promoting exclusive breastfeeding, timely immunization
- Advising when to return immediately
- Promoting appropriate home treatment
PRINCIPLES OF IMNCI (Important for Exam)
- All sick young infants (up to 2 months) must be examined for signs of "Possible Serious Bacterial Infection"
- All sick children (2 months to 5 years) must be examined for "General Danger Signs"
- Only a limited number of carefully selected clinical signs are used (sensitivity + specificity validated)
- A combination of signs leads to a classification - not a specific diagnosis
- Classifications are colour-coded to guide action
- All children are routinely assessed for nutritional and immunization status and feeding problems
- Involves counselling the mother and teaching home care
THE SIX STEPS OF IMNCI CASE MANAGEMENT
| Step | Action |
|---|---|
| 1. Assess | History + examination using chart booklet |
| 2. Classify | Colour-coded classification of severity |
| 3. Identify Treatment | Based on classification |
| 4. Treat | Pre-referral treatment / OPD treatment / home treatment |
| 5. Counsel the mother | Feeding, home care, when to return |
| 6. Follow-up | Reassess at scheduled return visit |
COLOUR-CODED RISK CLASSIFICATION SYSTEM
| Colour | Severity | Action |
|---|---|---|
| 🔴 PINK | Severe / Urgent | Urgent hospital referral + pre-referral treatment |
| 🟡 YELLOW | Moderate | Treat at OPD facility; oral drugs; advise; follow-up |
| 🟢 GREEN | Mild / Low risk | Home management; counsel caretaker; follow-up |
"Classifications are colour coded: pink suggests hospital referral or admission; yellow suggests that the child needs treatment; green suggests home management" - NHM IMNCI Module 1
TWO AGE GROUPS IN IMNCI
| Age Group | Chart Used | Primary Assessment |
|---|---|---|
| 0 up to 2 months (Young Infant / Neonate) | Sick Young Infant Chart | Check for Possible Serious Bacterial Infection (PSBI) |
| 2 months up to 5 years (Sick Child) | Sick Child Chart | Check for General Danger Signs |
PE 20.18 - Identifying and Stratifying Risk in a Sick Neonate Using IMNCI
ASSESSMENT OF SICK YOUNG INFANT (0-2 MONTHS)
The assessment follows this sequential order:
Step 1: Check for Possible Serious Bacterial Infection / Very Severe Disease / Local Bacterial Infection
Step 2: Check for Jaundice
Step 3: Check for Diarrhoea
Step 4: Check for Feeding Problem or Low Weight for Age
RISK STRATIFICATION IN SICK NEONATE - CLASSIFICATION TABLE
A. POSSIBLE SERIOUS BACTERIAL INFECTION (PSBI) / VERY SEVERE DISEASE
Classify as PSBI if ANY ONE of the following is present:
| Clinical Sign | Threshold |
|---|---|
| Not feeding well / stopped feeding | - |
| Convulsions | - |
| Fast breathing | ≥ 60 breaths/min |
| Severe chest indrawing | Deep and persistent |
| Grunting | - |
| Nasal flaring | - |
| Bulging fontanelle | - |
| 10 or more skin pustules / large boil | ≥ 10 pustules |
| Umbilical redness extending to periumbilical skin | - |
| Fever | Axillary temp ≥ 37.5°C |
| Hypothermia | Temp < 35.5°C |
| Lethargic or unconscious | - |
| Movement only when stimulated OR no movement | - |
| Cyanosis | - |
| Severely pale | - |
| SpO₂ < 90% | - |
| Blood glucose < 45 mg/dL | - |
Action (PINK - Urgent Referral):
- Give IM Ampicillin + Gentamicin (first dose, pre-referral)
- Prevent hypoglycaemia
- Keep warm (prevent hypothermia)
- Refer URGENTLY to hospital
B. LOCAL BACTERIAL INFECTION
Classify as LOCAL BACTERIAL INFECTION if:
- Umbilicus red OR draining pus (not extending to skin)
- Skin pustules < 10 in number
- Ear discharge
Action (YELLOW - OPD Treatment):
- Oral co-trimoxazole × 5 days
- Local antiseptic to umbilicus/skin
- Follow-up in 2 days
C. JAUNDICE CLASSIFICATION
| Classification | Signs | Action |
|---|---|---|
| Severe Jaundice (PINK) | Yellow palms AND soles | Urgent referral |
| Jaundice (YELLOW) | Yellow eyes/skin after 24h, palms/soles NOT yellow | Advise exposure to sunlight; follow-up in 1 day |
| No jaundice (GREEN) | No jaundice | Home management |
Note: Jaundice within first 24 hours is always pathological → classify as PSBI (pink)
D. DIARRHOEA CLASSIFICATION IN YOUNG INFANT
| Classification | Signs | Action |
|---|---|---|
| Severe dehydration (PINK) | Lethargic/unconscious + sunken eyes + skin pinch very slow + low weight | Give IM Ampicillin + Gentamicin; refer urgently |
| Some dehydration (YELLOW) | 2 of: restless/irritable, sunken eyes, skin pinch slow | ORS (Plan B); follow-up |
| No dehydration (GREEN) | Insufficient signs | ORS at home (Plan A); follow-up 5 days |
| Severe dysentery (PINK) | Blood in stool | Give IM Antibiotics; refer urgently |
E. FEEDING PROBLEM / LOW WEIGHT FOR AGE
| Classification | Signs | Action |
|---|---|---|
| Feeding problem or low weight (YELLOW) | Not able to feed well / weight < 2500g at birth | Breastfeeding support; advise; follow-up 2 days |
| No feeding problem (GREEN) | Feeding well, normal weight | Counsel; follow-up at 14 days |
PRE-REFERRAL TREATMENTS (Before sending to hospital)
- IM Ampicillin (first dose) - for PSBI
- IM Gentamicin (first dose) - for PSBI
- Prevent hypoglycaemia - give expressed breast milk / sugar water (if unable to breastfeed, give 10% dextrose orally)
- Prevent hypothermia - skin-to-skin / KMC / warm the room
- Treat to prevent low blood sugar
- Keep infant warm during transport
WHEN TO RETURN IMMEDIATELY (Counsel the Mother)
For a young infant, advise to return immediately if:
- Breastfeeding or drinking poorly
- Becomes sicker
- Develops fever OR feels cold to touch
- Fast breathing / difficult breathing
- Yellow palms and soles
- Blood in stool
- Repeated vomiting
- Abdominal distension
SUMMARY: IMNCI NEONATAL RISK STRATIFICATION AT A GLANCE
SICK NEONATE (0-2 months)
|
↓
CHECK FOR PSBI / VERY SEVERE DISEASE
|
ANY ONE SIGN? ──────────► PINK → Urgent Referral
(PSBI present) + IM Ampicillin/Gentamicin
|
NO PSBI SIGNS
|
LOCAL INFECTION? ────────► YELLOW → OPD Treatment
(few pustules, Oral Co-trimoxazole
umbilical redness) Follow-up 2 days
|
NO LOCAL INFECTION
|
JAUNDICE? ──────────────► YELLOW (mild) or PINK (palms+soles)
|
NO JAUNDICE
|
DIARRHOEA? ─────────────► Classify dehydration
|
FEEDING PROBLEM /
LOW WEIGHT? ────────────► YELLOW → Breastfeeding support
|
NONE OF ABOVE ──────────► GREEN → Home management + Counsel
KEY DIFFERENCES: IMNCI vs. IMCI (Indian Adaptation - OP Ghai emphasis)
| Feature | IMCI (WHO) | IMNCI (India) |
|---|---|---|
| Age coverage | 2 months - 5 years | 0-7 days + 2 months - 5 years |
| Neonatal coverage | Not included | Included (first week of life) |
| National guidelines | Generic | Includes Indian malaria, anaemia, Vit-A, immunization schedule |
| Training sequence | Child first | Young infant first |
| Training time | More on sick child | Equal - sick infant and sick child |
Sources: NHM Government of India - IMNCI Chart Booklet; IMNCI Training Module 1 (NHM, HP); Hospital-Based IMNCI 3rd Edition 2024; consistent with OP Ghai's Essential Paediatrics (IMNCI chapter) and Park's PSM
This is a shared conversation. Sign in to Orris to start your own chat.