SLE
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"systemic lupus erythematosus"[MeSH Terms] AND management
Finding Sources
Searching PubMed
"lupus erythematosus, systemic"[MeSH Terms]
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Systemic Lupus Erythematosus (SLE) - Complete Overview
Definition & Epidemiology
SLE is a chronic, multisystem autoimmune disease characterized by production of autoantibodies against nuclear antigens (especially nucleic acids and nuclear proteins), immune complex deposition, and resultant inflammation and tissue damage across virtually every organ system.
- Sex: Female:Male = ~9:1 (reproductive age)
- Peak onset: Ages 15-45; can occur at any age
- Ethnicity: More common and severe in Black, Hispanic, and Asian populations
- Prevalence: ~50-100 per 100,000 in developed countries
Etiology & Risk Factors
SLE arises from the interaction of genetic susceptibility, environmental triggers, and stochastic immune dysregulation. - Harrison's Principles of Internal Medicine 22E, 2025
Genetic Factors
- Strong genetic component: monozygotic twin concordance ~24% vs 2% in dizygotic twins
-
150 susceptibility loci identified via GWAS
- Key pathways:
- MHC (HLA-DR2, HLA-DR3) - antigen presentation
- Type I interferon axis: ~half of susceptibility loci affect IFN production or signaling (TLR7, STAT4, IRF5, IRF7, IRF8)
- Complement deficiencies (C1q, C2, C4) - impaired immune complex clearance
- Nucleic acid clearance genes (DNASE1, DNASE1L3, TREX1)
- B cell (BANK1, BACH2) and T cell (OX40L) activation genes
Environmental Triggers
- UV radiation (triggers keratinocyte apoptosis, exposing nuclear antigens)
- EBV infection (molecular mimicry with Sm/nuclear antigens)
- Hormones: Estrogens promote disease (explains female predominance and flares with pregnancy/OCP)
- Smoking, silica dust, certain drugs
Drug-Induced Lupus
Caused by hydralazine, procainamide, isoniazid, minocycline, anti-TNF agents, checkpoint inhibitors. Characterized by anti-histone antibodies; resolves on drug discontinuation.
Pathogenesis
The central mechanism is failure to clear apoptotic debris and self-nucleic acids, leading to chronic innate and adaptive immune activation:
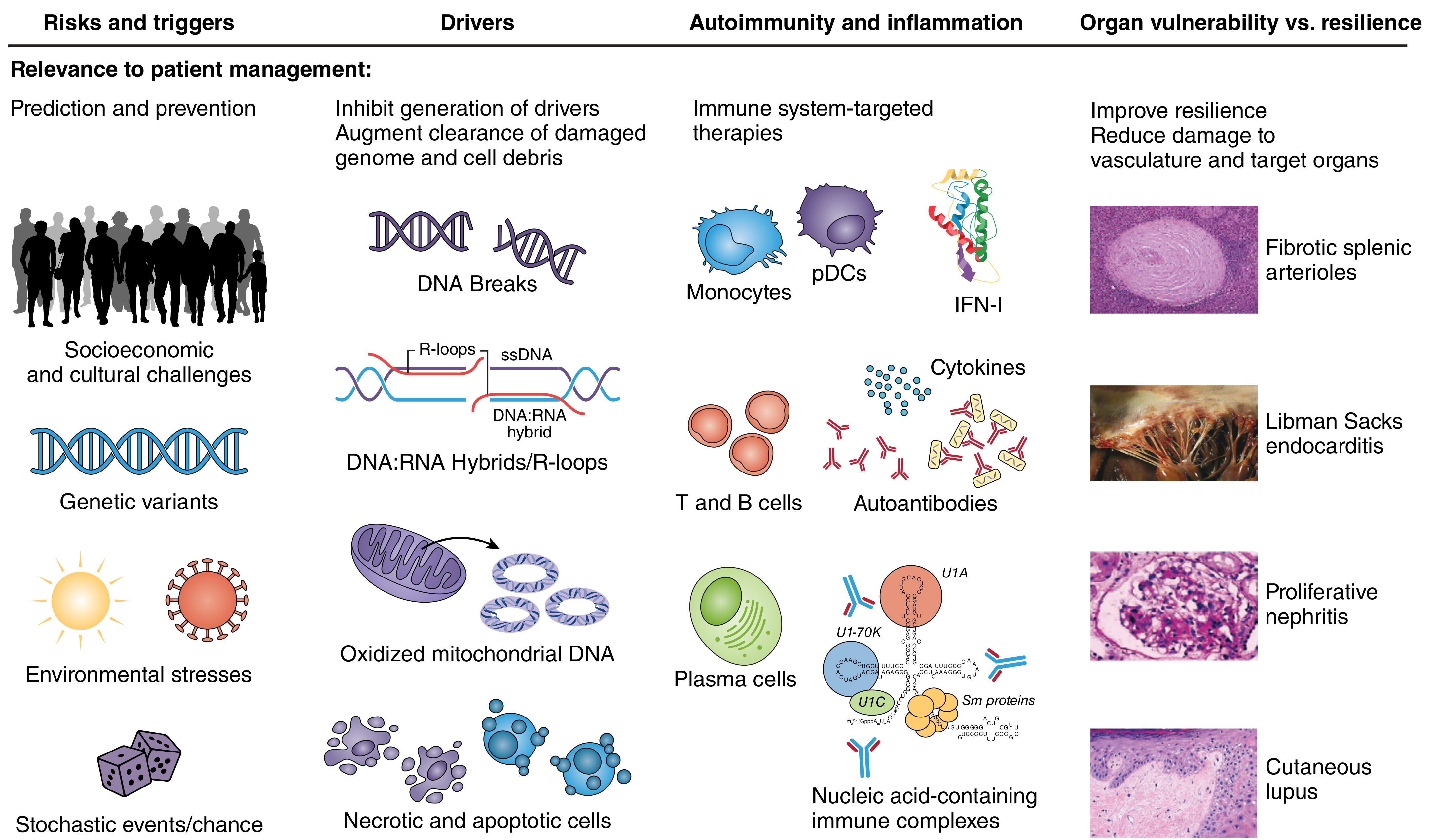
- Apoptotic cell overload / defective clearance - NETs (neutrophil extracellular traps) release chromatin into circulation
- Type I Interferon overproduction - Plasmacytoid dendritic cells (pDCs) sense self-nucleic acids via TLR7/9 → massive IFN-α/β production (the "IFN signature" seen in >75% of patients)
- Autoreactive B cells - Produce anti-dsDNA, anti-Sm, anti-Ro/SSA, anti-La/SSB antibodies
- T cell dysregulation - Reduced Tregs, overactive Th17 cells; self-reactive T cells help B cells differentiate into autoantibody-secreting plasma cells
- Immune complex deposition - Circulating anti-DNA antibody + DNA complexes deposit in glomeruli, skin, joints, choroid plexus → activate complement → inflammation and tissue damage
- Complement consumption - Low C3, C4 during active disease
Source: Harrison's Principles of Internal Medicine 22E; Firestein & Kelley's Textbook of Rheumatology
Clinical Features
SLE is the "great imitator." Manifestations vary greatly; the disease follows a relapsing-remitting course.
Malar ("Butterfly") Rash - the classic presentation:

Note the characteristic sparing of the nasolabial folds - Goldman-Cecil Medicine
Frequency of Manifestations
| Manifestation | Approximate Frequency |
|---|---|
| Cutaneous | 88% |
| Arthritis/arthralgias | 76% |
| Neuropsychiatric | 66% |
| Pleurisy/pericarditis | 63% |
| Anemia | 57% |
| Raynaud phenomenon | 44% |
| Vasculitis | 43% |
| Atherosclerosis | 37% |
| Nephritis | 31% |
| Thrombocytopenia | 30% |
| Cardiac valvular disease | 18% |
| Pulmonary alveolar hemorrhage | 12% |
Goldman-Cecil Medicine, Table 245-1
System-by-System Breakdown
Constitutional
- Fatigue (most common symptom), fever, weight loss, malaise, lymphadenopathy
Cutaneous (88%)
- Acute: Malar (butterfly) rash, maculopapular rash, bullous lupus
- Subacute (SCLE): Photosensitive annular or papulosquamous lesions; associated with anti-Ro/SSA
- Chronic: Discoid lupus (scarring, follicular plugging), panniculitis, chilblain lupus
- Other: Photosensitivity, oral/nasal ulcers, non-scarring alopecia, periungual telangiectases
Musculoskeletal (76%)
- Symmetric polyarthritis - non-erosive (unlike RA)
- Jaccoud's arthropathy - reversible deformities from periarticular laxity
- Avascular necrosis (especially femoral head; worsened by steroids)
- Myalgias, inflammatory myopathy
Renal (31-60%)
- Lupus nephritis is a major cause of morbidity
- Classified by ISN/RPS (WHO) histologic classes:
- Class I: Minimal mesangial
- Class II: Mesangial proliferative
- Class III: Focal proliferative (<50% glomeruli)
- Class IV: Diffuse proliferative (≥50% glomeruli) - most severe; "wire-loop" lesions on EM
- Class V: Membranous - presents as nephrotic syndrome
- Class VI: Advanced sclerosing
- Urinalysis shows hematuria, proteinuria, RBC casts (class III/IV)
Neuropsychiatric (NPSLE)
- Cognitive dysfunction (most common), headache, depression, psychosis
- Seizures, stroke/TIA, transverse myelitis, aseptic meningitis
- Mononeuropathy, polyneuropathy
Cardiopulmonary
- Pleuritis (30%), pericarditis (25%)
- Libman-Sacks endocarditis (verrucous, non-infective; associated with antiphospholipid antibodies)
- Premature atherosclerosis - major cause of late mortality
- Diffuse alveolar hemorrhage (rare but life-threatening)
- Pulmonary hypertension, shrinking lung syndrome
Hematologic
- Autoimmune hemolytic anemia (Coombs positive)
- Leukopenia, lymphopenia
- Thrombocytopenia (ITP-like)
- Antiphospholipid syndrome (APS) - in ~30-40%: venous/arterial thrombosis, recurrent pregnancy loss
Ocular
- Sicca syndrome, episcleritis, retinal vasculitis ("cytoid bodies" on fundoscopy)
Classification Criteria
Classification criteria are designed for clinical trial enrollment, not diagnosis - diagnosis remains clinical.
2019 EULAR/ACR Classification Criteria (most current)
- Entry criterion: ANA ≥1:80 by IIF (required)
- Then weighted clinical and immunological domains are scored
- Score ≥10 = classified as SLE
- Domains include: constitutional, hematologic, neuropsychiatric, mucocutaneous, serosal, musculoskeletal, renal, antiphospholipid antibodies, complement proteins, SLE-specific antibodies
2012 SLICC Criteria
- Requires ≥4 of 11 clinical + ≥1 immunologic criterion, OR biopsy-proven lupus nephritis + positive ANA or anti-dsDNA
- Higher sensitivity but lower specificity than EULAR/ACR 2019
Note: ~5% of SLE patients are ANA-negative; low complement + antiphospholipid antibodies can support diagnosis in ANA-negative cases.
Laboratory / Investigations
Autoantibodies
| Antibody | Sensitivity | Specificity | Clinical Significance |
|---|---|---|---|
| ANA | ~95-99% | Low | Best screening test; required for EULAR/ACR |
| Anti-dsDNA | ~40-60% | High (~97%) | Correlates with disease activity, especially nephritis |
| Anti-Sm | ~25-30% | Very high (~99%) | Pathognomonic for SLE |
| Anti-Ro/SSA | ~30-40% | Moderate | SCLE, neonatal lupus, Sjögren's overlap |
| Anti-La/SSB | ~15-20% | Moderate | With anti-Ro, neonatal heart block |
| Antiphospholipid Abs | ~30-40% | Moderate | Thrombosis, pregnancy loss (APS) |
| Anti-histone | ~50-70% | Low | Drug-induced lupus |
Complement
- Low C3, C4 (consumed by immune complexes) = active disease marker
Other Labs
- CBC: anemia, leukopenia (<4000/μL), lymphopenia (<1000/μL), thrombocytopenia (<100,000/μL)
- Urinalysis + sediment: hematuria, proteinuria, RBC/WBC casts
- BUN, creatinine, spot urine protein:creatinine ratio
- Coombs test (positive in AIHA)
- Direct Coombs, ESR, CRP (often normal in SLE flares)
Treatment
Management is guided by disease severity, organ involvement, and risk-benefit of immunosuppression.
All Patients - Background Therapy
- Hydroxychloroquine (HCQ, 200-400 mg/day): Cornerstone of SLE management. Reduces flares, organ damage, thrombosis, improves survival. Should be prescribed to ALL patients unless contraindicated. Annual ophthalmologic screening required (risk of retinopathy at cumulative doses).
- Sun protection: High-SPF sunscreen, protective clothing
- Vitamin D supplementation
- NSAIDs: For joint and serositis symptoms (short-term)
Mild-Moderate Disease (skin, joints, fatigue)
- Hydroxychloroquine ± NSAIDs
- Low-dose glucocorticoids (prednisone ≤7.5 mg/day)
- Methotrexate (15-25 mg/week) - for cutaneous and articular disease
- Belimumab (anti-BLyS/BAFF monoclonal antibody) - approved for moderate-to-severe SLE; reduces flares and organ damage
- Anifrolumab (anti-type I IFN receptor monoclonal antibody) - approved 2021 for moderate-to-severe SLE; particularly effective for skin and joint disease
Severe/Organ-Threatening Disease
- High-dose glucocorticoids (IV methylprednisolone pulses for acute flares)
- Mycophenolate mofetil (MMF) - first-line for lupus nephritis (induction and maintenance)
- Azathioprine - maintenance therapy; preferred agent in pregnancy
- Cyclophosphamide (IV pulses, Euro-Lupus low-dose regimen preferred) - for severe nephritis (class III/IV), CNS lupus, severe vasculitis
- Voclosporin (23.7 mg BID) + MMF + glucocorticoids - FDA-approved 2021 for active lupus nephritis
- Belimumab + MMF + glucocorticoids - FDA-approved 2020 for lupus nephritis
- Tacrolimus / Cyclosporine - calcineurin inhibitors for nephritis, especially proteinuria
- Rituximab (anti-CD20) - not approved but widely used for refractory nephritis, hemolytic anemia, severe thrombocytopenia
Emerging Therapies (Harrison's 22E, 2025)
- Obinutuzumab (next-gen anti-CD20) - phase III trials
- SGLT2 inhibitors - under study for nephroprotection in lupus nephritis
- CAR-T cell therapy - remarkable early results in very severe refractory SLE (case series)
Adjunctive
- ACE inhibitor / ARB - for lupus nephritis with proteinuria
- Warfarin (not DOACs) - for APS with thrombosis
- Colchicine - for pleuritis/pericarditis
- Gonadotropin-releasing hormone agonist before cyclophosphamide - to preserve fertility
Type 1 vs Type 2 SLE (new conceptual framework)
Harrison's 22E introduces a clinically useful distinction:
| Type 1 SLE | Type 2 SLE | |
|---|---|---|
| Features | Nephritis, vasculitis, arthritis, cytopenias | Fatigue, pain, cognitive dysfunction, depression, brain fog |
| Mechanism | Autoimmune inflammation / organ damage | Likely neuro-immune dysregulation, central sensitization |
| Response to IS | Good | Poor |
| Treatment | Standard immunosuppression | Symptomatic, pain management |
Pregnancy in SLE
- Pregnancy is possible but high-risk; ideally planned during remission (≥6 months)
- Risks: preeclampsia, preterm birth, IUGR, flares
- Neonatal lupus: Maternal anti-Ro/SSA IgG crosses placenta → neonatal skin rash, thrombocytopenia, hepatitis, complete congenital heart block (permanent, may require pacemaker)
- HCQ and low-dose prednisone can be continued; azathioprine preferred for IS in pregnancy
- Avoid: MMF, methotrexate, cyclophosphamide, belimumab in pregnancy
- Antiphospholipid antibodies → heparin (LMWH) + low-dose aspirin during pregnancy
Prognosis & Mortality
- 10-year survival now >90% with modern treatment
- Early mortality (<5 years): disease activity (nephritis, CNS, hemorrhage), infections
- Late mortality (>5 years): premature atherosclerosis and cardiovascular disease (3-10x increased risk), infections, malignancy
- Damage accrual (measured by SLICC damage index) is the strongest predictor of poor outcomes
Recent Evidence Update (PubMed, 2024-2026)
A 2024 systematic review informing the 2023 EULAR SLE management update (Ann Rheum Dis, PMID 38777375) confirms HCQ as backbone therapy, supports treat-to-target strategies, endorses voclosporin and belimumab for lupus nephritis, and highlights the role of anifrolumab for non-renal SLE.
Pregnancy outcomes research (PMID 39153486, Lancet Rheumatol 2024) identifies anti-dsDNA positivity, active nephritis at conception, and antiphospholipid antibodies as the strongest predictors of adverse pregnancy outcomes.
Sources: Harrison's Principles of Internal Medicine 22E (2025, McGraw-Hill); Goldman-Cecil Medicine International Edition; Firestein & Kelley's Textbook of Rheumatology 2-Volume Set; Rheumatology 2-Volume Set (Elsevier 2022)
This is a shared conversation. Sign in to Orris to start your own chat.