Congenital syphilis
Reading File
Finding Sources
Searching PubMed
"congenital syphilis"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
Loading Image
I now have all the information needed for a comprehensive, well-illustrated answer. Here is the full response:
Congenital Syphilis
Congenital syphilis results from transplacental, hematogenous spread of Treponema pallidum from mother to fetus. It can occur at any stage of pregnancy and at any stage of maternal infection. Because spread is hematogenous, a primary chancre is not present on the fetus or infant.
Epidemiology and Transmission Risk
The probability of transmission depends heavily on the stage of maternal syphilis:
| Maternal Stage | Transmission Risk |
|---|---|
| Primary / Secondary | 70-100% |
| Early latent (<1 year) | 40% |
| Late latent (>1 year) | 10% |
An untreated mother can infect her fetus during at least the first 5 years of her infection. T. pallidum can cross the placenta as early as the 6th gestational week, though anatomic fetal abnormalities are not apparent before 16 weeks' gestation (when fetal immunocompetence develops). Transmission can also occur intrapartum via contact with active genital lesions.
Untreated maternal syphilis leads to:
- Stillbirth in 30-40% of cases
- Neonatal death
- Preterm birth (rate ~28%)
- Fetal growth restriction (~21%)
Classification
Early congenital syphilis = onset before 2 years of age
Late congenital syphilis = onset at or after 2 years of age
Late congenital syphilis = onset at or after 2 years of age
60-90% of exposed neonates are asymptomatic at birth. Clinical signs typically emerge within the first 3 months of life if untreated.
Early Congenital Syphilis (< 2 Years)
The disease resembles secondary syphilis in adults. Classic features include:
Skin / Mucosal
- Rash at birth: bullous ("syphilitic pemphigus") - very infectious. The bullae rupture, leaving erosions, as seen below on the soles:

- Rash appearing 2+ weeks after birth: maculopapular, small copper-red lesions affecting hands and feet, similar to secondary syphilis; may progress to desquamation and crusting
- Condyloma lata, mucous patches, fissures around lips/nares/anus
- Petechiae (from thrombocytopenia)
- Dry, wrinkled skin with a café-au-lait or yellowish-brownish hue ("old man" appearance)
Below is the characteristic appearance of a newborn with early prenatal syphilis - note the dry wrinkled skin, yellowish hue, and hemorrhagic rhinitis:

Systemic
- "Snuffles" - persistent hemorrhagic rhinitis (a syphilitic rhinitis, flu-like with nasal discharge)
- Hepatosplenomegaly, jaundice
- Hemolytic anemia
- Lymphadenopathy
- Thrombocytopenia
- Hydrops fetalis (nonimmune edema)
- Leukocytosis
Skeletal
- Osteochondritis causing Parrot pseudoparalysis: the infant refuses to move the affected extremity due to pain - appears as limb immobility mimicking paralysis
- Periostitis
Neurologic
- Neurosyphilis (CSF abnormalities, meningitis)
Ocular
- Chorioretinitis, iritis
Late Congenital Syphilis (≥ 2 Years)
Many late manifestations result from irreversible damage from early infection - scarring and persistent inflammatory reactions. They are often not reversible with treatment.
Hutchinson's Triad (pathognomonic for late congenital syphilis)
- Hutchinson teeth - peg-shaped, widely-spaced, centrally notched upper central incisors (screwdriver-shaped), due to syphilitic vasculitis in developing tooth buds
- Interstitial keratitis - bilateral corneal inflammation; seen in ~1/3 of patients; may cause secondary cataracts, glaucoma, corneal scarring
- Eighth nerve deafness - sensorineural hearing loss

Dental
- Mulberry molars - permanent first molars with multiple poorly developed, rounded, rudimentary cusps
Skeletal (from chronic periostitis)
- Saddle nose deformity - destruction of nasal cartilage
- Frontal bossing (Olympian brow) - prominent frontal bones
- Saber shins - anterior bowing of the midtibia
- Scaphoid scapula
- Higoumenakia sign - thickening of the sternoclavicular portion of the clavicle
- Poor development of the maxilla
Skin
- Rhagades - perioral linear scars from cutaneous fissures of early congenital syphilis
Joints
- Clutton joints - late-onset bilateral knee arthritis (synovitis)
Neurologic
- Mental retardation, hydrocephalus, general paresis, optic nerve atrophy
Important Note
Cardiovascular manifestations (aortitis, aneurysm) seen in adult-acquired syphilis do not occur in congenital syphilis.
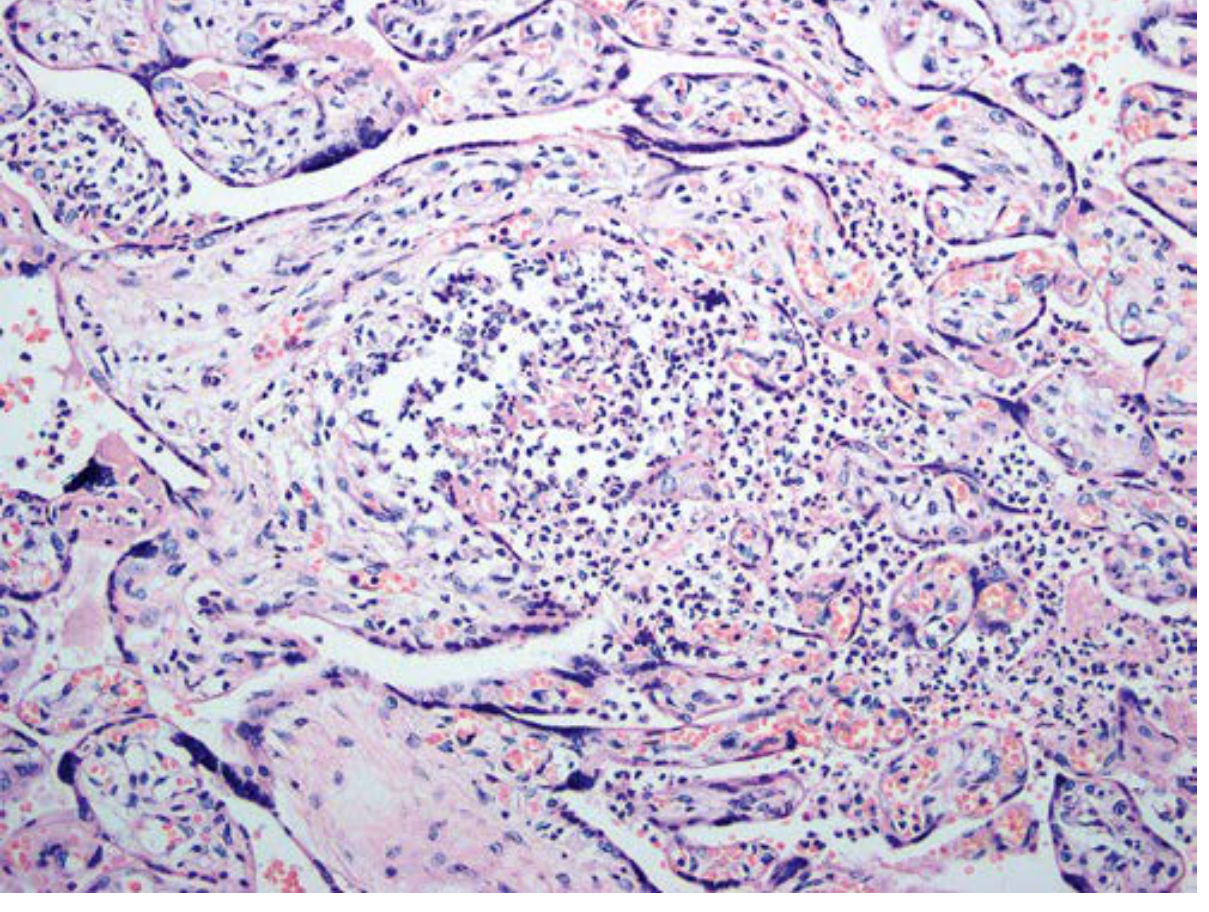
The histopathology of the placenta shows syphilitic placentitis with acute villitis in a large edematous placenta:
Diagnosis
Confirmed Case
T. pallidum identified by dark-field microscopy, fluorescent antibody staining, or other specific stains in specimens from lesions, placenta, umbilical cord, or autopsy material.
Presumptive Case (any of the following)
- Infant whose mother had untreated or inadequately treated syphilis at delivery
- Infant with reactive treponemal test PLUS:
- Clinical signs of congenital syphilis
- Reactive CSF VDRL
- Elevated CSF WBC (>5/mm³) or protein (>150 mg/dL)
- Reactive FTA-ABS for 19S-IgM fraction
Serologic Tests
Two types are used:
Nontreponemal tests (screening + treatment monitoring):
- RPR (Rapid Plasma Reagin)
- VDRL (Venereal Disease Research Laboratory)
- These detect anticardiolipin (anti-diphosphatidylglycerol) antibodies
- Quantifiable - ideal for monitoring response to treatment
- May give false positives
Treponemal tests (confirmatory):
- FTA-ABS (Fluorescent Treponemal Antibody Absorption)
- TPPA (T. pallidum particle agglutination)
- Detect antibodies to specific treponemal antigens
- Remain positive for life even after treatment (not useful for monitoring)
Maternal Screening
Serologic testing should be performed:
- At first prenatal visit (universal)
- At 28 weeks gestation
- At delivery (in high-risk areas/populations)
Treatment
Key Principle
T. pallidum is inhibited by <0.01 µg/mL of penicillin G. Because treponemes divide slowly and penicillin is active only on dividing cells, serum levels must be maintained for many days. Penicillin G is the only recommended drug for congenital syphilis.
Neonatal Treatment Algorithm
- Examine CSF first before starting treatment
- CSF normal → Single IM injection of benzathine penicillin G 50,000 units/kg (max 2.4 million units)
- CSF abnormal (neurosyphilis) → Aqueous penicillin G 50,000 units/kg IV/IM twice daily for minimum 10 days OR Procaine penicillin 50,000 units/kg IM once daily for 10 days
Treat infant at birth if:
- Mother received no treatment or inadequate treatment
- Mother was treated with drugs other than penicillin
- Mother has not yet responded to therapy
- Infant cannot be carefully monitored for several months
Maternal Treatment (prevents congenital syphilis)
Adequate treatment before 16 weeks usually prevents clinical illness in the neonate. Later treatment may not prevent late sequelae.
| Indication | Treatment |
|---|---|
| Early syphilis (<1 year) | Benzathine penicillin G 2.4 million units IM single dose |
| Late latent / unknown duration | Benzathine penicillin G 7.2 million units IM (2.4 MU weekly x 3) |
| Neurosyphilis | Aqueous penicillin G 2-4 million units IV q4h x 10-14 days |
Jarisch-Herxheimer Reaction
Up to 60% of patients with early syphilis experience a transient febrile reaction within hours of starting treatment. It peaks at 6-8 hours and resolves within 12-24 hours. In pregnant women, it may rarely precipitate preterm labor. It is caused by cytokine release from spirochete antigen liberation, not an allergic reaction to penicillin.
Differential Diagnosis
Early congenital syphilis resembles other TORCH infections: cytomegalovirus, toxoplasmosis, herpes simplex virus, rubella ("TORCH" infections).
Key Clinical Pearls
- Syphilis in a child beyond the neonatal period should prompt evaluation for child sexual abuse
- An infant may be seronegative if maternal infection was acquired late in pregnancy
- The classic description of an affected newborn: "a little wrinkled, potbellied old man with a cold in his head" (Diday)
- Congenital syphilis does not cause cardiovascular syphilis (unlike adult-acquired disease)
- The "snuffles" of congenital syphilis teeming with spirochetes are extremely infectious
Sources: Fitzpatrick's Dermatology (8th ed.), Goldman-Cecil Medicine, Creasy & Resnik's Maternal-Fetal Medicine, Andrews' Diseases of the Skin, Dermatology 2-Volume Set (5e)
This is a shared conversation. Sign in to Orris to start your own chat.