Atrial flutter
Reading File
Finding Sources
Searching PubMed
"atrial flutter"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent - I now have comprehensive content and two key images. Let me compile the full answer.
Atrial Flutter
Definition & Mechanism
Atrial flutter is a macro-reentrant supraventricular tachyarrhythmia with an atrial rate of approximately 300 beats/min and a ventricular response that depends on the degree of AV block - typically 150 bpm (2:1), 100 bpm (3:1), or slower multiples.
Typical (CTI-dependent) atrial flutter involves a reentrant circuit confined to the right atrium. The circuit travels:
- Counterclockwise (more common): caudocranial up the interatrial septum, craniocaudal down the right atrial free wall
- Clockwise (less common): reverse direction
The cavotricuspid isthmus (CTI) - the narrow strip of tissue between the inferior vena cava and tricuspid annulus - acts as a critical slow-conduction zone and is the target of ablation.
Atypical atrial flutter involves macro-reentrant circuits that do NOT use the CTI - these often occur in the left atrium after mitral valve surgery or catheter ablation for AF, or are scar-mediated. - Braunwald's Heart Disease
ECG Findings
The classic ECG shows a sawtooth flutter wave pattern:
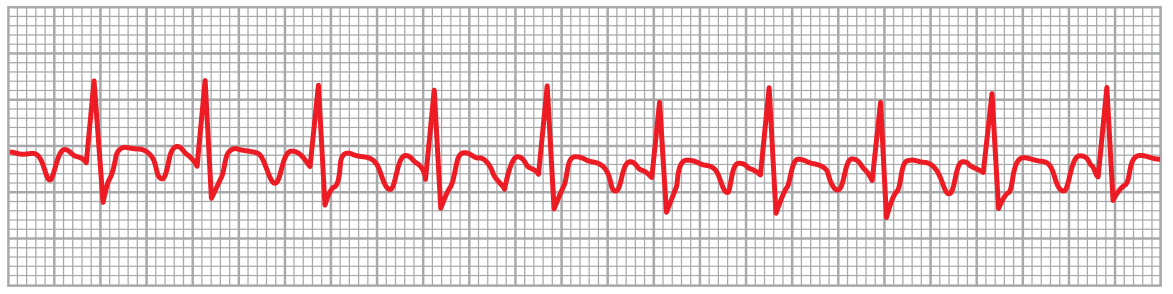
Atrial flutter at 250 bpm with 2:1 AV block giving a ventricular rate of 125 bpm - Guyton & Hall Textbook of Medical Physiology
| Feature | Counterclockwise (Typical) | Clockwise (Reverse Typical) |
|---|---|---|
| Leads II, III, aVF | Negative (sawtooth) | Positive |
| Lead V1 | Positive | Negative |
| Atrial rate | ~300 bpm | ~300 bpm |
Clinical Presentation
- Asymptomatic if AV block results in a physiologic rate
- Palpitations, light-headedness, syncope, or shortness of breath with faster ventricular rates
- Can precipitate heart failure or myocardial ischemia in patients with underlying heart disease
- If high-grade AV block develops: bradycardia, light-headedness, syncope
Aetiology / Associations
Typical atrial flutter almost always occurs with underlying cardiovascular or pulmonary disease. It can also be triggered by antiarrhythmic drugs (e.g., sodium-channel blockers used for AF). Common precipitants include hypoxia, fever, and electrolyte abnormalities. - Goldman-Cecil Medicine
Management
The approach follows three parallel tracks:
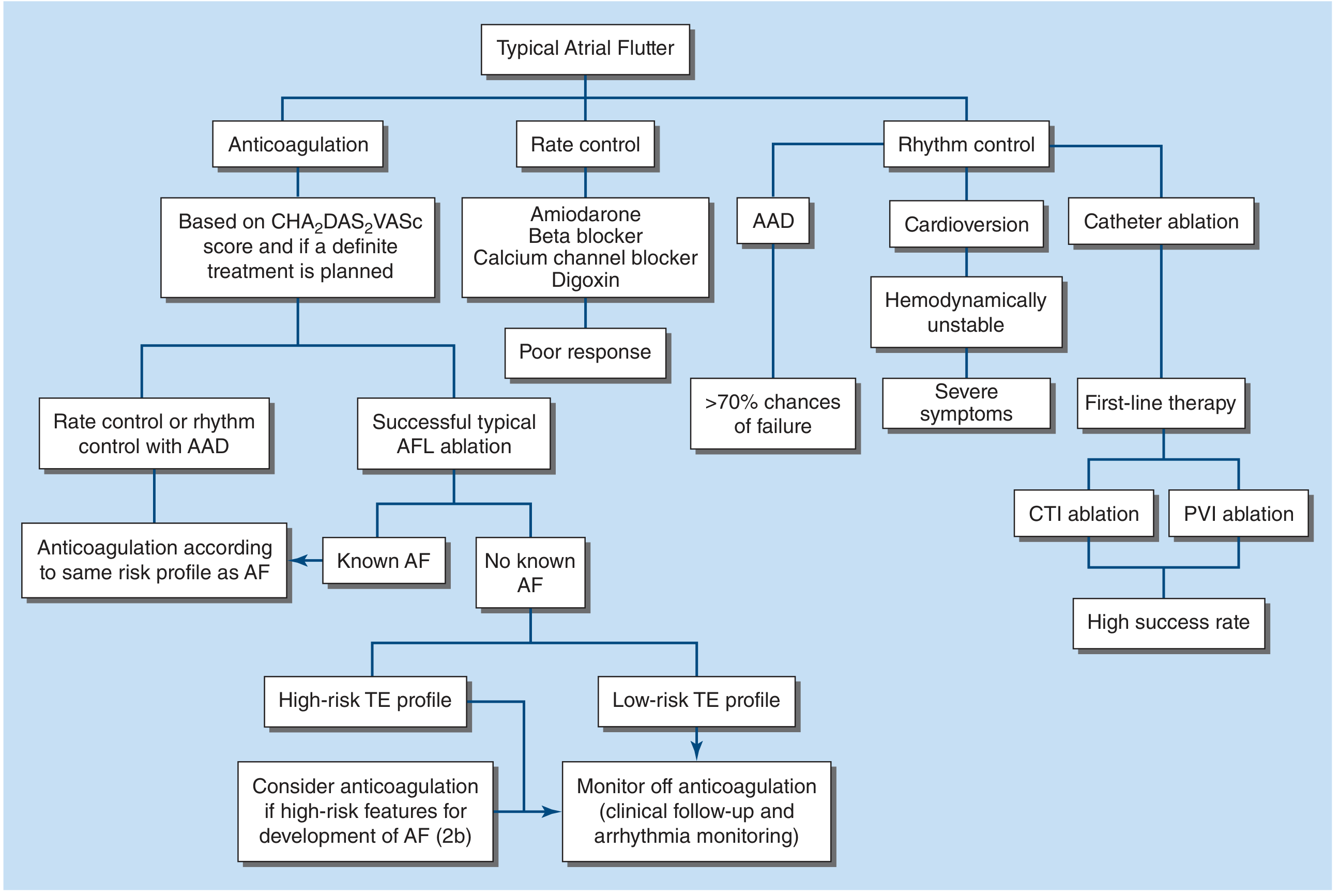
1. Anticoagulation
- Risk-stratify using CHA₂DS₂-VASc score
- Required before cardioversion unless episode is confirmed <48 hours, TEE has excluded left atrial appendage thrombus, or the patient is hemodynamically unstable requiring emergency cardioversion
- If cardioversion is not urgent: therapeutic anticoagulation (DOAC or warfarin with INR 2-3) for 4 weeks prior
- 3% per year thromboembolic risk - long-term anticoagulation similar to AF guidelines for patients at risk of recurrence
- After successful CTI ablation with no known AF and low-risk TE profile: can monitor off anticoagulation
2. Rate Control
- AV nodal blocking agents: beta-blockers (e.g., metoprolol 25-50 mg daily), calcium channel blockers (e.g., diltiazem 180-240 mg daily), amiodarone, or digoxin
- Rate control in atrial flutter is harder to achieve compared to AF - the AV node tends to conduct at fixed ratios (e.g., 2:1, 3:1), leading to abrupt rate changes
- Temporary measure while planning definitive rhythm control
3. Rhythm Control
Acute cardioversion:
- DC cardioversion is preferred and >95% effective
- IV ibutilide (1 mg over 10 min, repeat once if needed) - ~60% effective for chemical cardioversion
- Other antiarrhythmics (sotalol, dofetilide, disopyramide, amiodarone) - but >70% recurrence rate
Definitive therapy - Catheter ablation:
- Radiofrequency ablation of the CTI is >95% curative for typical flutter and is the first-line, preferred option for most patients
- Low risk of complications and low recurrence rates
- Antiarrhythmic drugs are a secondary option or for atypical flutter where ablation success is lower
Important caveat: Up to 50% of patients undergoing CTI ablation subsequently develop atrial arrhythmias, most commonly atrial fibrillation. This is an ongoing area of research.
Post-Ablation Follow-Up
- If ablation is successful and no known AF: risk of recurrence is very small - long-term anticoagulation is not necessary in low-risk patients
- If known AF coexists: continue anticoagulation based on AF risk profile
- Monitor for AF development with clinical follow-up and arrhythmia monitoring
Prognosis
Prognosis is generally determined by underlying comorbid conditions (heart disease, pulmonary disease) rather than the arrhythmia itself. Successful CTI ablation offers near-curative rates for typical flutter.
Recent evidence note: A 2025 systematic review (PMID 40434140) assessed pulsed field ablation (PFA) as an emerging modality for CTI-dependent flutter, showing favorable safety and efficacy - though this remains under investigation. A 2024 meta-analysis (PMID 39784135) found dapagliflozin (SGLT2 inhibitor) may have a protective effect against AF/flutter and reduce all-cause mortality.
Sources: Braunwald's Heart Disease; Harrison's Principles of Internal Medicine 22E; Goldman-Cecil Medicine; Guyton & Hall Textbook of Medical Physiology
This is a shared conversation. Sign in to Orris to start your own chat.