A clinical study on human with respect to its development it's circulation muscles. It's pathophysiology
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Loading Image
Here is a comprehensive clinical study of the Heart covering its development, circulation, muscles, and pathophysiology, drawn from multiple authoritative medical textbooks.
The Human Heart: Development, Circulation, Cardiac Muscle, and Pathophysiology
PART 1 - CARDIAC DEVELOPMENT (Embryology)
1.1 Primary and Secondary Heart Fields
The heart is the first functional organ in the human embryo, operational by approximately week 4 of development. Specialized cells leave the primitive streak and migrate anteriorly to form an inverted U-shaped region called the cardiac crescent (primary heart field). A second population - the secondary heart field - derives from pharyngeal mesoderm.
- Primary heart field cells become ventricular myocardium
- Secondary heart field cells become atria, outflow tracts, and portions of the right ventricle
Key molecular signals driving this process include:
- BMPs and FGFs from the anterior visceral endoderm
- Transcription factors NKX2.5 and GATA4
- Retinoic acid (RA) gradients: high posterior RA induces atrial formation; low/absent RA drives ventricular development
- HAND-1 (restricted to left side of posterior heart tube) and HAND-2 (predominantly right ventricle) - asymmetric expression drives cardiac looping into the four-chamber configuration
(Source: Creasy & Resnik's Maternal-Fetal Medicine)
1.2 Cardiac Looping and Chamber Formation
The primitive tubular heart loops to form distinct chambers. Neural crest cells participate in formation of the outflow tracts. Defects in neural crest derivatives cause 22q11 deletion syndrome (DiGeorge syndrome) due to haploinsufficiency of transcription factor TBX1.
1.3 Development of Cardiac Valves
As partitioning of the truncus arteriosus nears completion, semilunar valves develop from three swellings of subendocardial tissue around the orifices of the aorta and pulmonary trunk. Neural crest cells also contribute to this tissue. These swellings are hollowed out and reshaped to form three thin-walled cusps. The AV valves (tricuspid and mitral) develop similarly from localized proliferations of tissue around the AV canals.
(Source: The Developing Human - Clinically Oriented Embryology)
1.4 Development of the Conducting System
Initially, myocardium of the primordial atrium and ventricle is continuous. As chambers form, certain cells conduct depolarization faster.
- SA node: develops in week 5; located in the right wall of the sinus venosus, incorporated into the right atrial wall at the SVC junction - the pacemaker of the heart
- AV node and bundle: formed from cells of the left sinus venosus wall and AV region; located superior to the endocardial cushions
- Bundle branches: split from the AV bundle and distribute throughout ventricular myocardium
- The two chambers (atrial and ventricular) are electrically isolated by fibrous tissue; only the AV node and bundle conduct across
- Parasympathetic innervation derives from neural crest cells that also play an essential role in conducting system development
1.5 Development of Coronary Blood Vessels
By the end of week 5, blood islands appear at the atrioventricular and interventricular grooves and in the epicardium. Precursor cells forming coronary vessels derive from the proepicardium and areas near the sinus venosus. Mesenchymal cells deep to the epicardium form vascular channels (vasculogenesis), which then branch into a capillary network. By day 44, a vascular plexus penetrates the atrioventricular groove and aortic root to form the coronary ostia and coronary artery stem. The tunica media and adventitia mature during the late embryonic/early fetal period.
(Source: The Developing Human - Clinically Oriented Embryology)
PART 2 - CORONARY CIRCULATION
2.1 Anatomical Overview
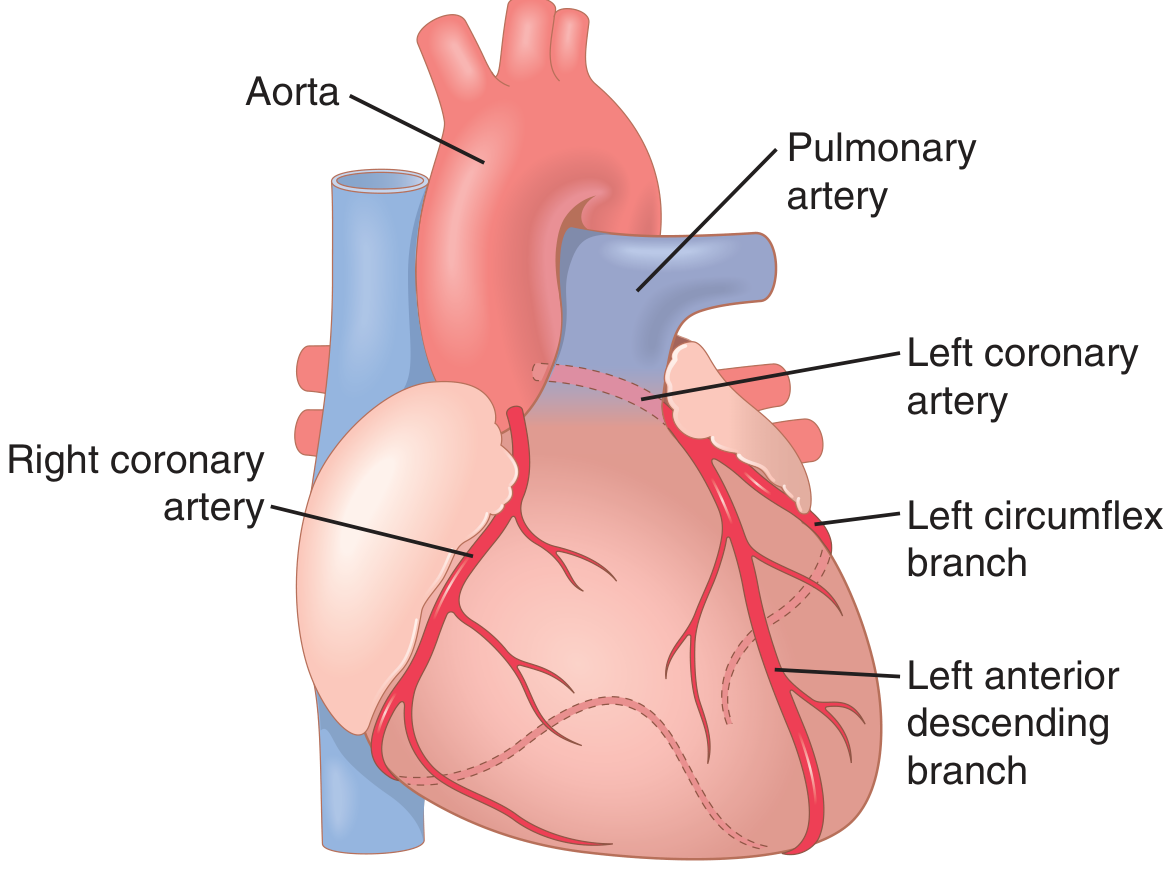
The main coronary arteries lie on the surface (epicardium) of the heart, with smaller branches penetrating into the myocardium. Only the inner 0.1 mm of the endocardial surface receives nutrition directly from the cardiac chamber blood; the rest depends entirely on the coronary arteries.
| Vessel | Territory Supplied |
|---|---|
| Left coronary artery (LCA) | Anterior and left lateral portions of the left ventricle |
| Left anterior descending (LAD) | Anterior interventricular septum, anterior LV |
| Left circumflex (LCx) | Lateral and posterior LV |
| Right coronary artery (RCA) | Most of RV; posterior LV in 80-90% of people |
Venous drainage:
- ~75% of coronary venous blood from the left ventricle drains via the coronary sinus to the right atrium
- Right ventricular venous blood drains via anterior cardiac veins directly to the right atrium
- Small amounts drain via thebesian veins into all chambers
(Source: Guyton and Hall Textbook of Medical Physiology)
2.2 Coronary Blood Flow - Quantitative Features
- Resting coronary blood flow: ~70 mL/min/100 g of heart weight, ~225 mL/min total (4-5% of cardiac output)
- During strenuous exercise: coronary flow increases 3-4 fold, while cardiac work increases 6-9 fold - the efficiency of cardiac energy utilization must increase to compensate
Phasic nature of coronary flow:
During systole, mechanical compression of intramuscular coronary vessels causes a brief reduction of blood flow - especially in the left ventricle. Blood flow to the LV is therefore predominantly diastolic. When compression ends, reactive hyperemia restores oxygen delivery.
2.3 Control of Coronary Blood Flow
Blood flow is controlled almost entirely by local metabolites, with sympathetic innervation playing only a minor role:
- Hypoxia and adenosine are the most important local vasodilators. Increased myocardial demand → local hypoxia → coronary arteriole vasodilation → increased flow (active hyperemia)
- Adenosine mechanism: severe ischemia degrades ATP → ADP → AMP → adenosine, which diffuses out of cells and dilates coronary arterioles. Critically, adenine stores deplete within 30 minutes of severe ischemia and are replaced at only ~2%/hour - this is a key mechanism of irreversible cardiac cell death
- Other vasodilators: CO₂, H⁺ (decreased pH), bradykinin, prostaglandins
- Sympathetic innervation: epicardial coronary vessels have predominantly alpha (vasoconstricting) receptors; intramuscular arteries may have more beta receptors. In some individuals, excessive alpha vasoconstriction causes vasospastic ischemia (Prinzmetal angina)
(Source: Guyton and Hall Textbook of Medical Physiology; Costanzo Physiology)
PART 3 - CARDIAC MUSCLE (Histology and Structure)
3.1 Embryological Origin
Cardiac muscle develops from the lateral splanchnic mesoderm, which gives rise to mesenchyme surrounding the developing heart tube. Cardiac myoblasts differentiate from the primordial myocardium, recognizable by week 4. Key regulators include PBX proteins interacting with HAND2 to promote cardiac muscle differentiation. Immunohistochemical studies show spatial distribution of myosin heavy-chain isoforms in the embryonic heart between weeks 4-8.
(Source: The Developing Human - Clinically Oriented Embryology)
3.2 Structural Organization
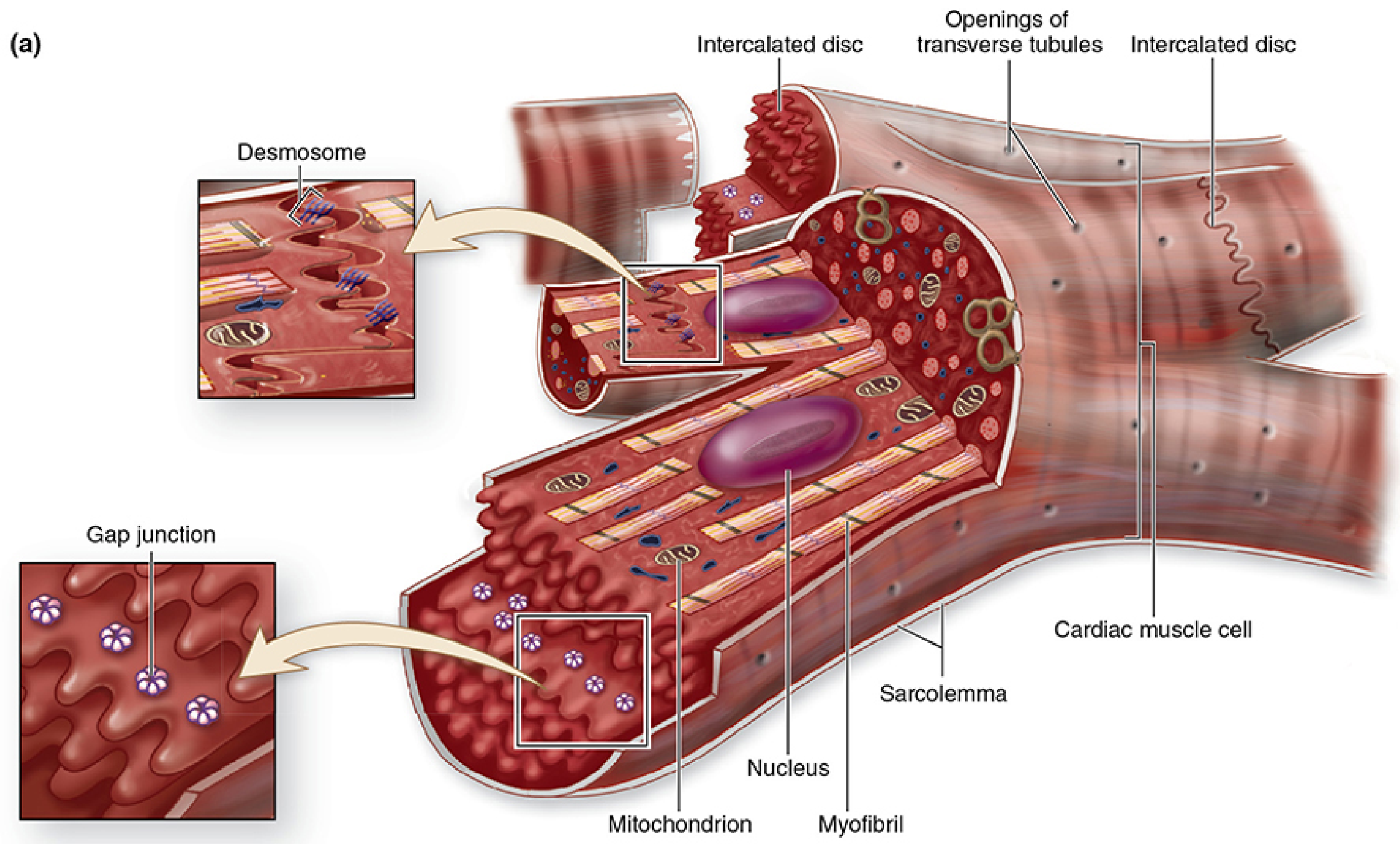
Cardiac muscle fibers form by differentiation and growth of single cells (not fusion, unlike skeletal muscle). The cells form complex intercellular junctions during development:
Intercalated Discs - the defining structural feature of cardiac muscle:
- Visible as irregular transverse lines crossing the fibers
- Transverse regions: highly interdigitated, contain abundant desmosomes and fascia adherens junctions - provide mechanical adhesion during constant contraction
- Lateral (longitudinal) regions: contain numerous gap junctions - provide ionic continuity (electrical synapses), promoting rapid impulse conduction so many cells contract simultaneously as a functional syncytium
The heart is consequently a functional syncytium: tightly knit bundles of cells interwoven in spiraling layers producing a wringing-type contraction that efficiently empties the ventricles.
(Source: Junqueira's Basic Histology)
3.3 Cellular Features
| Feature | Detail |
|---|---|
| Cell diameter | 15-30 μm |
| Nucleus | Single, central, euchromatic |
| Mitochondria | Occupy up to 40% of cell volume (higher than slow-twitch skeletal muscle) |
| Primary fuel | Fatty acids (~70% of energy at rest); stored as triglycerides in small lipid droplets |
| T-tubules | Present in ventricles (associate with Z discs); smaller/absent in atria |
| SR junctions | Form dyads (one T-tubule + one SR terminal cistern) rather than triads as in skeletal muscle |
| Atrial granules | Right atrium contains ~600 granules/cell containing atrial natriuretic factor (ANF) precursor - promotes natriuresis and diuresis, opposes aldosterone and ADH |
3.4 Purkinje Fibers
Late in the embryonic period, special conducting cells differentiate from original trabeculated myocardium. These Purkinje fibers have:
- Fast-conducting gap junctions
- Relatively few myofibrils
- Relatively larger diameters
They form the specialized conduction system of the heart.
(Source: The Developing Human - Clinically Oriented Embryology; Junqueira's Basic Histology)
PART 4 - PATHOPHYSIOLOGY
4.1 Ischemic Heart Disease
Ischemic heart disease is the most common cause of death in men and women in Western countries, accounting for ~35% of deaths in individuals aged 65+ in the United States. It results from insufficient coronary blood flow.
Mechanisms of myocardial ischemia:
- Atherosclerotic coronary artery disease - the most common cause; plaques narrow the vessel lumen
- Coronary vasospasm - due to excessive alpha-adrenergic stimulation
- Microvascular disease - especially in women (ischemia without obstructive CAD, or INOCA)
Cellular consequences of ischemia:
- Reduced coronary flow → local hypoxia → shift from fatty acid oxidation to anaerobic glycolysis
- Anaerobic glycolysis consumes large amounts of glucose and produces lactic acid (likely contributes to cardiac pain/angina)
- ATP degrades: ATP → ADP → AMP → adenosine, which diffuses out of cells
- Within 30 minutes of severe ischemia, ~50% of adenine bases are lost from affected cells
- Adenine is replaced at only ~2%/hour; therefore >30 min of severe ischemia may cause irreversible cell death - this is why reperfusion therapy (thrombolytics, PCI) is time-critical
Zones of injury in myocardial infarction:
- The subendocardium is most vulnerable because coronary flow is already reduced during systole and this area is farthest from the epicardial blood supply
4.2 Valve Pathology - Congenital Basis
- Developmental errors in valve formation cause bicuspid aortic valve (failure to form 3 cusps from the truncus arteriosus swellings), leading to aortic stenosis and regurgitation in adults
- Ebstein's anomaly: abnormal development of the tricuspid valve
- These arise from disruption of the subendocardial swellings or neural crest contributions during weeks 5-8
4.3 Congenital Heart Defects (CHDs)
CHDs occur at a frequency of ~6 per 1000 live births. Common examples arising from developmental disruption include:
| Defect | Developmental Basis |
|---|---|
| Tetralogy of Fallot | Abnormal conotruncal septation |
| Transposition of Great Arteries | Failure of aorticopulmonary septum rotation |
| VSD / ASD | Incomplete septal formation |
| DiGeorge syndrome (22q11 deletion) | Loss of TBX1 → neural crest defects in outflow tract |
4.4 Heart Failure Pathophysiology
When myocardial function is impaired (from ischemia, hypertension, valve disease, or cardiomyopathy), compensatory mechanisms are activated:
- Frank-Starling mechanism: increased preload stretches myofibrils → stronger contraction (initially compensatory, eventually fails)
- Neurohormonal activation: RAAS and sympathetic nervous system activated → vasoconstriction, Na⁺/water retention (aldosterone and ADH) → worsening volume overload
- ANF/BNP release: atrial and ventricular granules release natriuretic peptides to counteract RAAS (basis for serum BNP as a heart failure biomarker)
- Myocardial remodeling: hypertrophy → fibrosis → dilation → eventual systolic dysfunction
Summary Table
| Domain | Key Points |
|---|---|
| Development | Primary/secondary heart fields; NKX2.5, GATA4, HAND1/2; SA node at week 5; coronary vasculogenesis from proepicardium |
| Coronary Circulation | LCA (anterior LV) + RCA (RV, posterior LV); flow regulated by O₂/adenosine; phasic - mainly diastolic in LV |
| Cardiac Muscle | Lateral splanchnic mesoderm origin; intercalated discs (desmosomes + gap junctions); 40% mitochondria; dyads not triads; ANF in atrial granules |
| Pathophysiology | Ischemia → lactic acid + adenine loss → cell death at 30 min; atherosclerosis main cause; CHDs from week 4-8 developmental errors; heart failure via RAAS + neurohormonal activation |
Sources:
- The Developing Human - Clinically Oriented Embryology (Moore, Persaud)
- Guyton and Hall Textbook of Medical Physiology, 14e
- Junqueira's Basic Histology, 17e
- Costanzo Physiology, 7e
- Creasy & Resnik's Maternal-Fetal Medicine
This is a shared conversation. Sign in to Orris to start your own chat.