Neonatal resuscitation
Reading File
Finding Sources
Searching PubMed
"neonatal resuscitation"[MeSH Terms] AND guidelines
Reading File
Reading File
Searching PubMed
"neonatal resuscitation" AND "newborn"
Reading File
Reading File
Loading Image
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Reading File
Here is a comprehensive overview of neonatal resuscitation based on the NRP guidelines (AHA 2015 update), drawn from multiple authoritative textbooks.
Neonatal Resuscitation
Overview
About 10% of newborns require some assistance to establish breathing at birth; fewer than 1% need extensive resuscitation. The goal is to support the physiological transition from fetal to neonatal circulation. Resuscitation of the neonate ideally begins before delivery - with antenatal counseling, team briefing, and equipment check.
Neonatal Resuscitation Algorithm
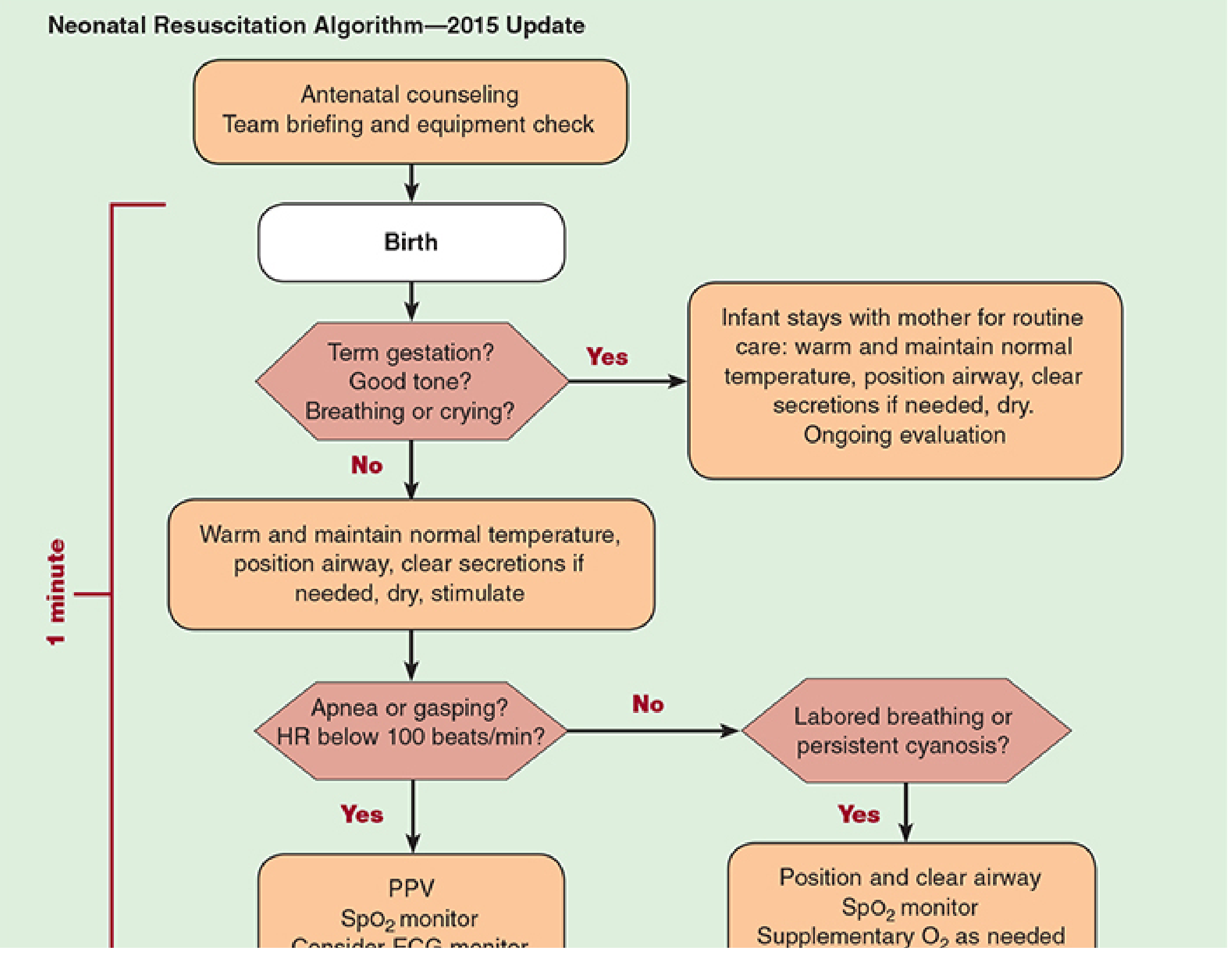
NRP Algorithm (AHA 2015 Update) - Morgan & Mikhail's Clinical Anesthesiology, 7e
Pre-Delivery Preparation
Maternal history questions to ask:
- Estimated gestational age?
- Multiple gestation?
- Meconium present?
- Maternal fever?
- Medications/drugs given?
- Any abnormalities on prenatal ultrasound?
Equipment checklist (ROSEN's Emergency Medicine):
- Radiant warmer, blankets, plastic wrap (for prematurity/omphalocele)
- Bulb syringe, suction catheters (5, 8, 10 Fr), wall suction <100 mmHg
- Self-inflating bag (450/750 mL) or flow-inflating bag (250/450 mL)
- Masks (premature, newborn, infant sizes)
- Laryngoscope with straight blades (Nos. 00, 0, 1) - Miller blades for intubation
- ETTs (2.5, 3.0, 3.5, 4 mm), uncuffed, with stylets
- CO2 detector, meconium aspirator
- Umbilical catheters (3.5 and 5 Fr)
- ECG leads, pulse oximeter
Step 1: Initial Assessment (First 60 seconds - "The Golden Minute")
Ask three questions at birth:
- Term gestation?
- Good tone?
- Breathing or crying?
If YES to all three → routine care: warm, maintain temperature, position airway, clear secretions if needed, dry. Infant stays with mother.
If NO to any → proceed with resuscitation steps below.
Step 2: Initial Stabilization Steps
Perform simultaneously:
- Warm (prevent hypothermia - independent risk factor for neonatal mortality)
- Position airway (slight neck extension; 1-inch towel under shoulders helpful)
- Clear airway if needed - bulb or mechanical suction, mouth before nose (<100 mmHg)
- Dry and stimulate (rub the back, flick soles of feet)
Suctioning should be reserved for obvious obstruction only - overly vigorous suctioning causes vagal bradycardia and apnea.
Meconium exception: Suction the trachea with ETT + meconium aspirator only if meconium is present AND the newborn has poor tone, poor respiratory effort, or HR <100 bpm after 1 minute of PPV.
Normal neonatal vitals:
- Respirations: 30-60 breaths/min (begins within 30 s, sustained within 90 s)
- Heart rate: 120-160 bpm
Step 3: Assess Response - Apgar Score
The Apgar score is recorded at 1 min and 5 min after delivery.
| Sign | 0 | 1 | 2 |
|---|---|---|---|
| Heart rate | Absent | <100 bpm | >100 bpm |
| Respirations | Absent | Weak/irregular | Strong cry |
| Muscle tone | Limp | Some flexion | Active motion |
| Reflex irritability | None | Grimace | Cry/cough |
| Color | Blue/pale | Blue extremities | Pink all over |
- Score 7-10: Normal
- Score 5-7 (mild asphyxia): Stimulation + blow-by O2
- Score 3-4 (moderate asphyxia): PPV with bag-mask
- Score 0-2 (severe depression): Immediate intubation + possible chest compressions
The 1-min score correlates with survival; the 5-min score has a limited relationship to neurological outcome.
Step 4: Positive Pressure Ventilation (PPV)
Indications:
- Apnea or gasping respirations
- Persistent central cyanosis on 100% O2
- Heart rate persistently <100 bpm
Technique:
- Rate: 40-60 breaths/min
- Initial breath pressure: up to 40 cmH2O; thereafter, do not exceed 30 cmH2O
- Preterm: 20-25 cmH2O
- Start with room air (not 100% O2) for term infants; titrate by SpO2
- SpO2 probe on right upper extremity (preductal)
If no improvement with PPV - use "MR. SOPA":
- M - Mask: adjust seal
- R - Reposition head to open airway
- S - Suction mouth then nose
- O - Open mouth with jaw thrust
- P - increase Pressure (max 40 cmH2O)
- A - Airway: proceed to definitive airway (ETT)
ETT sizes by weight:
| Birth Weight | ETT Size |
|---|---|
| <1 kg | 2.5 mm |
| 1-2 kg | 3.0 mm |
| >2 kg | 3.5 mm |
ETT depth ("tip to lip") = 6 cm + weight in kg
Confirm placement with capnography.
Step 5: Chest Compressions
Indications: HR <60 bpm despite adequate PPV for 30 seconds
Technique - two methods:
- Two-thumb encircling technique (preferred): both thumbs on lower one-third of sternum, fingers encircling the chest. Generates greater peak systolic pressures.
- Two-finger technique: second and third digits on lower sternum. More practical when colleague is placing umbilical catheter.
Depth: ~1 cm (one-third chest depth)
Rate: 90 compressions/min + 30 ventilations/min = 3:1 ratio (compression:ventilation)
Stop compressions when spontaneous HR >60 bpm; then increase ventilation rate to 40-60 breaths/min.
Intubation is strongly recommended before initiating chest compressions.
Step 6: Medications and Vascular Access
Vascular Access
Preferred: Umbilical vein catheter (UVC) - 3.5F or 5F
- Tip just below skin level (free backflow of blood)
- Do not advance too far - risks infusing hypertonic solutions into liver
- Alternatives: IO access, peripheral vein, endotracheal tube
Drug Therapy
| Drug | Indication | Dose | Route |
|---|---|---|---|
| Epinephrine | HR <60 despite adequate ventilation + compressions x 45-60 s | 0.01-0.03 mg/kg (0.1-0.3 mL/kg of 1:10,000) IV/IO; 0.05-0.1 mg/kg ET | IV/IO preferred; repeat q3-5 min |
| Normal saline / LR / O-neg blood | Known/suspected blood loss, pallor, poor perfusion | 10 mL/kg | IV/IO slowly over 3-5 min |
| Calcium gluconate | Documented hypocalcemia or suspected Mg intoxication (maternal MgSO4) | 100 mg/kg (CaGluconate) or 30 mg/kg (CaCl2) | IV |
| Sodium bicarbonate | Severe documented metabolic acidosis + adequate ventilation | 2 mEq/kg of 4.2% solution | IV; rate ≤1 mEq/kg/min |
| Glucose | Hypoglycemia | 8 mg/kg/min | IV infusion |
| Naloxone | Respiratory depression from opioids given to mother in last 4 h | 0.1 mg/kg IV or 0.2 mg/kg IM | Contraindicated if maternal opioid addiction suspected (risks neonatal seizures) |
Naloxone and sodium bicarbonate are no longer recommended for routine neonatal resuscitation.
Step 7: Post-Resuscitation Care
- Any degree of asphyxia requires close observation in special care nursery or NICU
- Therapeutic hypothermia (33.5°C): Consider for term or near-term (≥36 weeks) neonates with moderate-to-severe hypoxic-ischemic encephalopathy (HIE). Significant reduction in mortality and improved 18-month neurological outcomes shown in multiple large trials. Turn off warmer immediately to initiate passive cooling; monitor temperature continuously.
- Obtain emergency neonatology consultation early
When to Discontinue Resuscitation
Consider discontinuing resuscitation if there is no cardiac activity after 10 minutes of complete and adequate resuscitative efforts (confirmed asystole). Each case requires individualized decision-making based on gestational age, clinical context, and family input.
Special Situations
Prematurity
- Nearly two-thirds of premature infants requiring resuscitation are hypovolemic at birth
- Use plastic wrap instead of drying to prevent heat loss
- Gentler ventilation pressures (20-25 cmH2O)
- Higher risk of intraventricular hemorrhage - give volume slowly
Fetal Resuscitation (Intrauterine)
- Intrauterine asphyxia during labor is the most common cause of neonatal depression
- Interventions: correct maternal hypotension (fluids/vasopressors), supplemental O2, stop oxytocin/give tocolytics
- Normal fetus can compensate ~45 min of relative hypoxia before progressive lactic acidosis
Sources:
- Morgan & Mikhail's Clinical Anesthesiology, 7e, pp. 1651-1665
- ROSEN's Emergency Medicine, pp. 3125-3131
- Tintinalli's Emergency Medicine, pp. 716-718
- Miller's Anesthesia, 10e
My teacher taught me 15:1 and 30:2 for chest compression
Finding Sources
Finding Sources
Reading File
Reading File
Your teacher is partially right - but those ratios apply to different age groups, not neonates. Here's the full picture with textbook-verified data:
Compression-to-Ventilation Ratios in CPR
| Population | Single Rescuer | Two Rescuers | Rate |
|---|---|---|---|
| Adult | 30:2 | 30:2 | 100-120/min |
| Pediatric (infant/child) | 30:2 | 15:2 | 100-120/min |
| Neonatal (newborn) | 3:1 | 3:1 | 90 compressions + 30 ventilations = 120 events/min |
Breaking it down:
30:2 - Adult AND single-rescuer pediatric CPR (standard BLS)
15:2 - Pediatric CPR with two or more rescuers. This is the ratio your teacher was likely referring to for children/infants. The rationale is that respiratory problems are more commonly the cause of arrest in children, so more frequent ventilations are needed. - Barash, Cullen & Stoelting's Clinical Anesthesia, 9e
3:1 - Neonatal resuscitation only (newborns in the delivery room). This gives 90 compressions and 30 ventilations per minute. - ROSEN's Emergency Medicine; Roberts & Hedges' Clinical Procedures in Emergency Medicine
Exception within neonates: If the arrest is known to be of primary cardiac cause (rather than the typical asphyxial cause), a 15:2 ratio may be considered even in neonates. - ROSEN's Emergency Medicine
Why is neonatal 3:1 different from pediatric 15:2?
Neonatal cardiac arrest is almost always asphyxial (from respiratory failure), not primary cardiac. The heart is healthy - it just needs oxygenated blood. So more frequent ventilations relative to compressions are prioritized. This is the opposite of the adult model where primary cardiac causes dominate.
Bottom line: Your teacher's 15:2 is correct for pediatric (two-rescuer) CPR. The 30:2 is correct for adults or single-rescuer pediatric. For neonates specifically, the ratio is 3:1. All three ratios are correct - they just apply to different populations.
This is a shared conversation. Sign in to Orris to start your own chat.