Excellent - I now have comprehensive textbook content and diagrams. Let me compose the full long-answer English notes.
THE NERVOUS SYSTEM — Complete Long Answer Notes
Sources: Histology: A Text and Atlas (Ross & Pawlina) | Guyton & Hall Medical Physiology | Ganong's Review of Medical Physiology, 26th Ed. | Principles of Neural Science (Kandel), 6th Ed. | Medical Physiology (Boron & Boulpaep)
1. WHAT IS THE NERVOUS SYSTEM?
The nervous system is the body's master control and communication network. It receives sensory information from both the internal and external environments, integrates and processes that information, and generates appropriate motor responses. It is responsible for all conscious thought, emotion, memory, and perception, as well as the regulation of virtually every organ and tissue in the body.
Functions of the Nervous System
| Function | Description |
|---|
| Sensory Input | Detects stimuli via receptors - pain, temperature, touch, pressure, vision, hearing, smell |
| Integration | Processes, analyzes, and stores sensory data; makes decisions |
| Motor Output | Sends commands to muscles (movement) and glands (secretion) |
| Homeostasis | Regulates heart rate, blood pressure, temperature, breathing |
| Higher Functions | Memory, learning, language, reasoning, emotion, consciousness |
2. CLASSIFICATION OF THE NERVOUS SYSTEM
NERVOUS SYSTEM
│
├── CENTRAL NERVOUS SYSTEM (CNS)
│ ├── Brain
│ └── Spinal Cord
│
├── PERIPHERAL NERVOUS SYSTEM (PNS)
│ ├── Afferent (Sensory) Division
│ ├── Efferent (Motor) Division
│ │ ├── Somatic NS — voluntary, skeletal muscle
│ │ └── Autonomic NS — involuntary, viscera
│ ├── Cranial Nerves (12 pairs)
│ └── Spinal Nerves (31 pairs)
│
└── AUTONOMIC NERVOUS SYSTEM (ANS) [subdivision of PNS]
├── Sympathetic Division ("Fight or Flight")
└── Parasympathetic Division ("Rest and Digest")
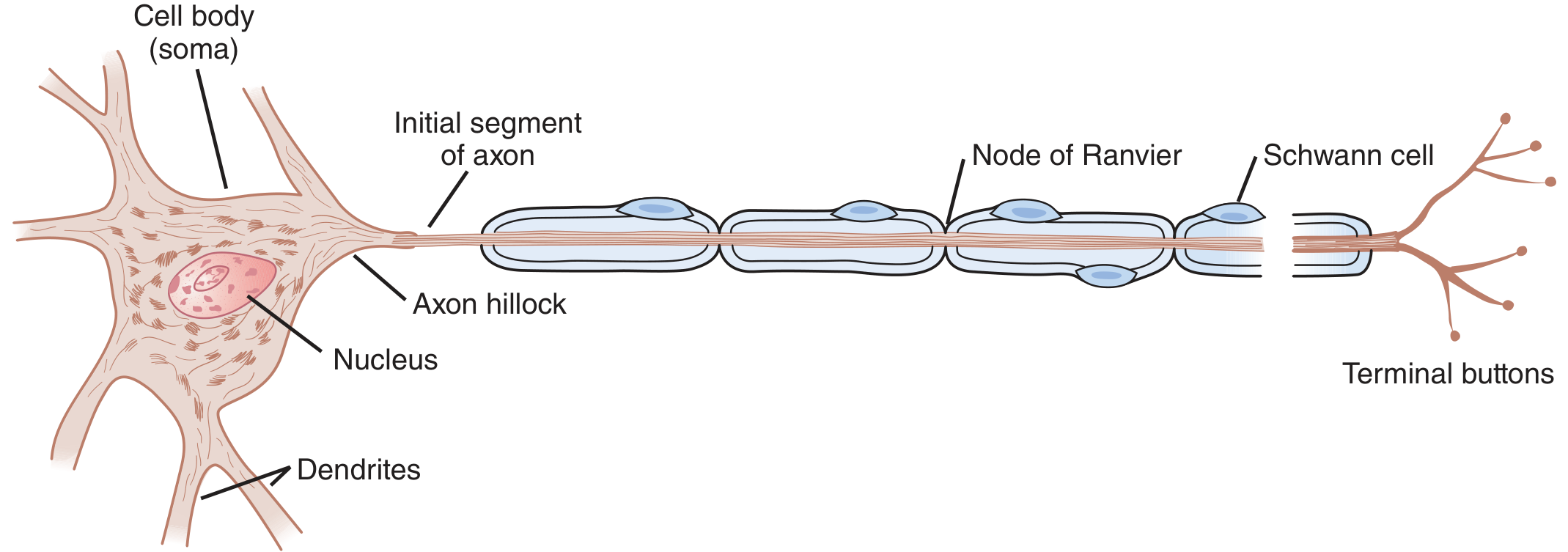
3. NEURON — THE STRUCTURAL AND FUNCTIONAL UNIT
The neuron is the structural and functional unit of the nervous system. The human nervous system contains more than 10 billion neurons (some estimates reach 80-100 billion in the CNS alone). Despite enormous variation in size and shape, all neurons share a common architecture.
Structure of a Neuron
| Component | Structure | Function |
|---|
| Cell Body (Soma / Perikaryon) | Contains nucleus, Nissl bodies (rough ER), mitochondria, Golgi | Metabolic center of the neuron; synthesizes proteins; contains DNA |
| Dendrites | Multiple short branching processes; covered in dendritic spines | Receive incoming signals from other neurons; integrate synaptic input |
| Axon Hillock | Thickened cone-shaped junction between soma and axon | Site where action potentials are generated (lowest threshold) |
| Axon (Nerve Fiber) | Single long process; one axon per neuron; can be up to 1 meter | Conducts action potentials away from the cell body to targets |
| Myelin Sheath | Lipid-rich wrapping around axon (from Schwann cells/oligodendrocytes) | Electrical insulation; speeds up conduction |
| Nodes of Ranvier | Gaps in the myelin sheath at regular intervals | Sites of ionic exchange during saltatory conduction |
| Axon Terminal / Terminal Buttons (Boutons) | Presynaptic endings containing synaptic vesicles | Store and release neurotransmitters into the synapse |
"A typical neuron also has a long fibrous axon that originates from a thickened area of the cell body (axon hillock). The axon divides into presynaptic terminals, each ending in a number of synaptic knobs that contain granules or vesicles in which synaptic transmitters released by the nerves are stored." - Ganong's Review of Medical Physiology
Four Functional Zones of a Neuron
- Dendritic zone - local potential changes generated by synaptic connections are integrated
- Initial segment - propagated action potentials are generated
- Axon - conducts the action potential to distant targets
- Terminal buttons - release neurotransmitters at the synapse
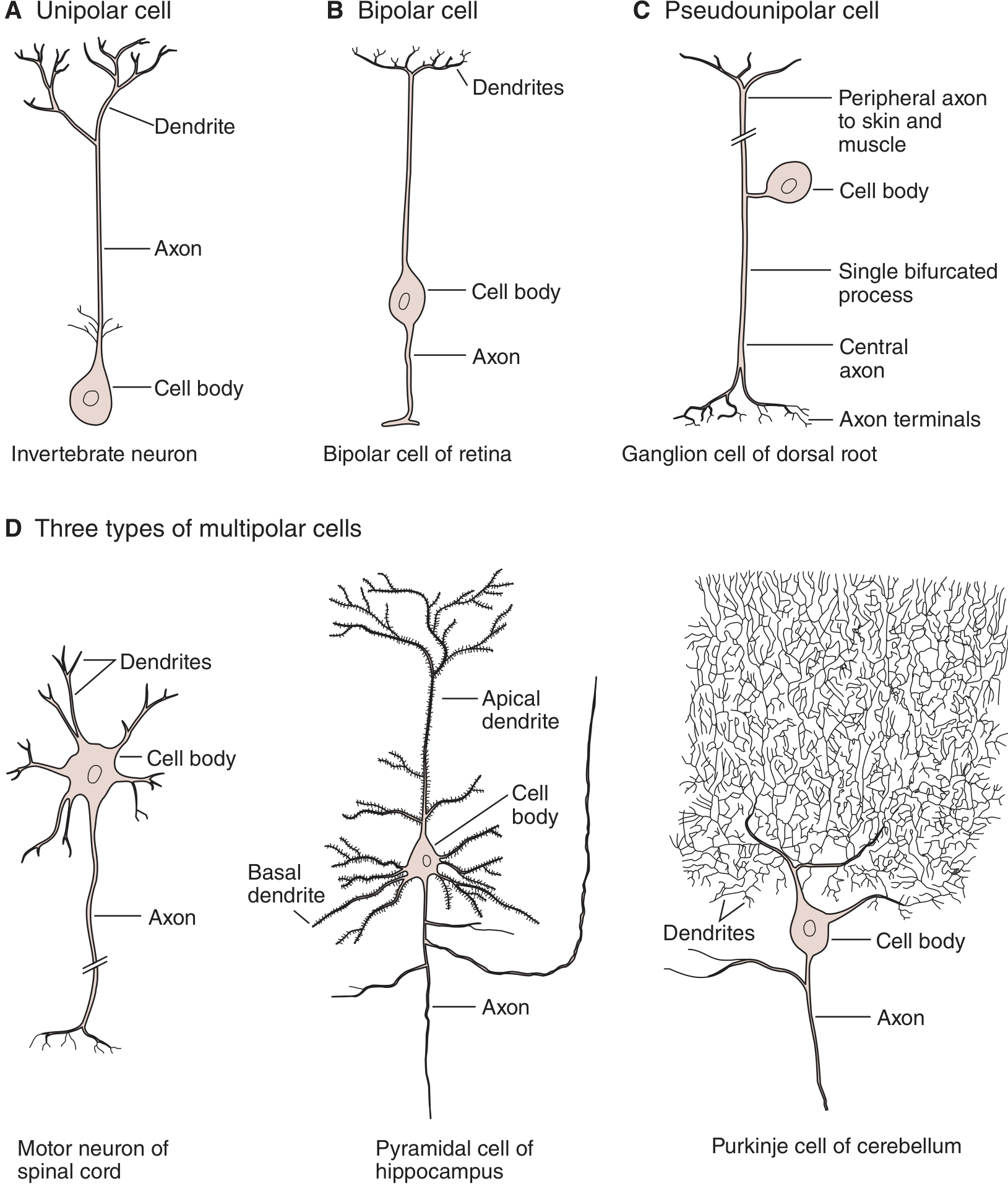
Classification of Neurons
A. By Number of Processes:
| Type | Processes | Example |
|---|
| Unipolar | One process from soma | Invertebrate neurons |
| Bipolar | One dendrite + one axon | Retinal photoreceptors, cochlear ganglion cells |
| Pseudounipolar | One process that splits into two (both act as axons) | Dorsal root ganglion cells (cutaneous sensory) |
| Multipolar | One axon + many dendrites | Spinal motor neurons, cerebral pyramidal cells, cerebellar Purkinje cells |
B. By Function:
| Type | Direction | Role |
|---|
| Sensory (Afferent) | Receptor → CNS | Convey pain, temperature, touch, proprioception from body surface and viscera |
| Motor (Efferent) | CNS → Effector | Carry commands to skeletal muscle (somatic) or smooth muscle/glands (visceral) |
| Interneurons (Association) | Within CNS | Integrate sensory and motor information; >99.9% of all neurons belong to this category |
4. NEUROGLIA (GLIAL CELLS)
Glial cells are the non-neuronal supporting cells of the nervous system. They outnumber neurons by approximately 10:1 and perform vital roles in maintaining the neuronal environment.
Central Nervous System Glia
| Cell Type | Location | Key Functions |
|---|
| Astrocytes | CNS | - Form the Blood-Brain Barrier (BBB) with endothelial cells - Maintain ionic homeostasis (K⁺ buffering) - Provide nutrients (lactate) to neurons - Respond to injury (reactive gliosis) - Guide neuronal migration during development |
| Oligodendrocytes | CNS | - Produce and maintain the myelin sheath in the CNS - One oligodendrocyte can myelinate up to 50 axons simultaneously - Damage causes Multiple Sclerosis |
| Microglia | CNS | - Resident immune cells of the CNS (CNS macrophages) - Phagocytose pathogens, dead neurons, and debris - Produce cytokines; monitor synaptic activity |
| Ependymal Cells | CNS | - Line the ventricular system and central canal of spinal cord - Produce Cerebrospinal Fluid (CSF) via Choroid Plexus - Some (tanycytes) transport substances between CSF and brain tissue |
Peripheral Nervous System Glia
| Cell Type | Location | Key Functions |
|---|
| Schwann Cells | PNS | - Produce myelin sheath in the PNS - One Schwann cell myelinates one segment of one axon - Also ensheath unmyelinated fibers (Remak bundles) - Essential for peripheral nerve regeneration after injury |
| Satellite Cells | PNS | - Surround cell bodies in ganglia - Provide structural and metabolic support to ganglion neurons |
Key Distinction: CNS myelin = Oligodendrocytes | PNS myelin = Schwann cells. This is why MS (CNS demyelination) and Guillain-Barre syndrome (PNS demyelination) are separate diseases.
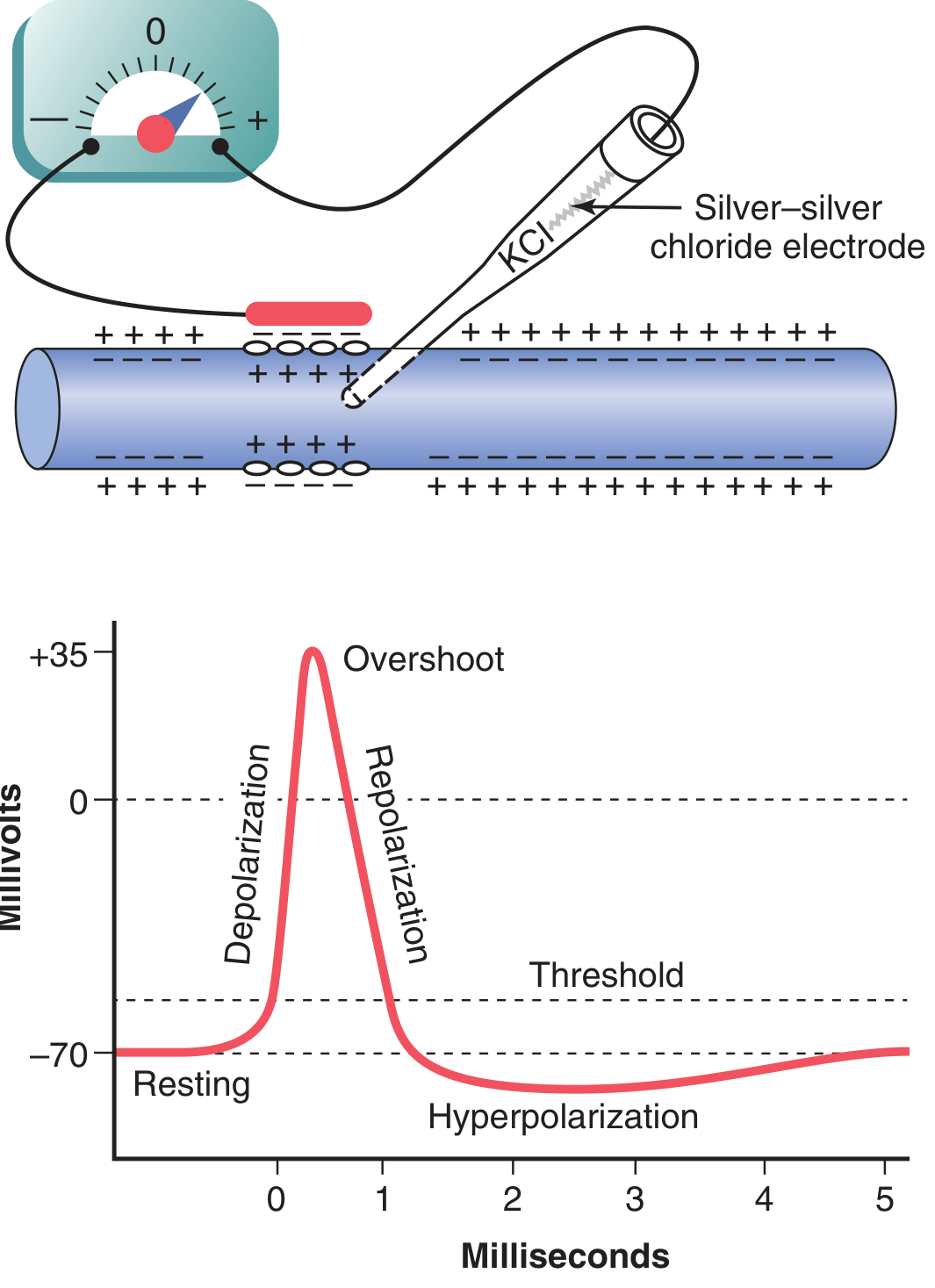
5. NERVE IMPULSE (ACTION POTENTIAL)
Resting Membrane Potential (RMP)
At rest, the inside of the neuron is negative (-70 mV) relative to the outside. This electrochemical gradient is maintained by:
- Na⁺/K⁺-ATPase Pump: Actively pumps 3 Na⁺ out and 2 K⁺ in (net outward positive charge)
- Selective permeability: Membrane at rest is more permeable to K⁺ than Na⁺ (K⁺ leaks out)
- Large intracellular anions (proteins, phosphates) that cannot cross the membrane
Ion distribution at rest:
- Na⁺ : High outside (145 mEq/L), Low inside (12 mEq/L)
- K⁺ : High inside (140 mEq/L), Low outside (4 mEq/L)
- Cl⁻ : High outside (100 mEq/L)
Action Potential
An action potential is a rapid, self-propagating reversal of membrane polarity triggered when the membrane reaches threshold (~-55 mV).
| Phase | Membrane Potential | Ionic Events |
|---|
| Resting | -70 mV | Na⁺ channels closed; K⁺ leak channels open |
| Threshold | -55 mV | Depolarizing stimulus brings membrane to this critical level |
| Depolarization (Rising phase) | -70 → +35 mV | Voltage-gated Na⁺ channels open → Na⁺ floods inward → inside becomes positive |
| Overshoot | +30 to +35 mV | Peak of action potential |
| Repolarization (Falling phase) | +35 → -70 mV | Na⁺ channels inactivate; voltage-gated K⁺ channels open → K⁺ flows outward |
| Hyperpolarization (Undershoot) | Below -70 mV | K⁺ channels slow to close; brief overshoot into hyperpolarization |
| Refractory Period | Returns to -70 mV | Absolute refractory: no new AP possible (Na⁺ channels inactivated) - Relative refractory: only a supramaximal stimulus triggers AP |
"An action potential is triggered when a stimulus depolarizes the membrane to a threshold level, usually around -55 mV. At this time, the membrane suddenly becomes permeable to sodium ions, allowing rapid diffusion of positively charged sodium ions to the interior of the axon." - Guyton & Hall
The All-or-None Law
An action potential either occurs fully or does not occur at all. The size and speed of an AP is fixed for a given neuron regardless of stimulus strength. Stimulus strength is encoded by the frequency of action potentials, not their amplitude.
Saltatory Conduction
In myelinated fibers, action potentials "jump" from one Node of Ranvier to the next, rather than propagating continuously along the membrane. This is called saltatory conduction (from Latin saltare = to jump).
- Conduction velocity: up to 120 m/s in large myelinated fibers vs. < 2 m/s in unmyelinated fibers
- Extremely energy-efficient - ionic exchange occurs only at nodes
- Demyelination (as in Multiple Sclerosis) dramatically slows or blocks conduction
6. SYNAPSE
A synapse is the specialized junction between two neurons (or between a neuron and an effector cell) across which signals are transmitted.
Structure of a Chemical Synapse
Presynaptic Neuron (Axon Terminal)
- Synaptic vesicles (contain neurotransmitters)
- Active zone (site of vesicle docking)
- Voltage-gated Ca²⁺ channels
↓
Synaptic Cleft (~20-40 nm gap)
↓
Postsynaptic Membrane
- Neurotransmitter receptors (ionotropic or metabotropic)
- Postsynaptic density (scaffold proteins)
Mechanism of Synaptic Transmission
- Action potential reaches the presynaptic terminal
- Voltage-gated Ca²⁺ channels open → Ca²⁺ enters the terminal
- Ca²⁺ triggers vesicle fusion with the presynaptic membrane (exocytosis)
- Neurotransmitter is released into the synaptic cleft
- Neurotransmitter binds to receptors on the postsynaptic membrane
- Postsynaptic response occurs (excitation or inhibition)
- Neurotransmitter is removed by: reuptake, enzymatic degradation, or diffusion
Types of Synapses
| Type | Mechanism | Speed | Direction | Example |
|---|
| Chemical | Neurotransmitters released into cleft | Slower (0.5-1 ms delay) | Unidirectional | Most synapses in CNS |
| Electrical | Gap junctions - direct ionic flow | Very fast | Bidirectional | Cardiac muscle, some CNS interneurons |
Excitatory vs. Inhibitory Synapses
- Excitatory synapse: Releases glutamate, acetylcholine, or serotonin → opens Na⁺ or Ca²⁺ channels → depolarization → EPSP (Excitatory Post-Synaptic Potential) → action potential
- Inhibitory synapse: Releases GABA or glycine → opens Cl⁻ channels → hyperpolarization → IPSP (Inhibitory Post-Synaptic Potential) → prevents action potential
"The ultimate generation of a nerve impulse in a postsynaptic neuron depends on the summation of excitatory and inhibitory impulses reaching that neuron. This allows precise regulation of the reaction of a postsynaptic neuron." - Ross & Pawlina Histology
Receptor Types
| Receptor | Type | Mechanism | Speed |
|---|
| Ionotropic | Ligand-gated ion channel | NT binding opens channel directly | Fast (milliseconds) |
| Metabotropic | G-protein coupled receptor (GPCR) | NT activates G-protein → 2nd messenger cascade | Slow (seconds to minutes); modulates activity |
Major Neurotransmitters
| Neurotransmitter | Type | Location | Function | Clinical Relevance |
|---|
| Acetylcholine (ACh) | Excitatory/Inhibitory | NMJ, ANS, basal forebrain | Muscle contraction, memory, parasympathetic | ↓ in Alzheimer's; blocked in Myasthenia Gravis |
| Dopamine | Modulatory | Substantia nigra, VTA, limbic | Reward, motivation, fine motor control | ↓ in Parkinson's; ↑ in Schizophrenia |
| Serotonin (5-HT) | Modulatory | Raphe nuclei | Mood, sleep, appetite, pain modulation | ↓ in Depression; SSRIs increase serotonin |
| GABA | Inhibitory | Widespread in CNS | Primary inhibitory NT; anxiety reduction | ↓ causes Epilepsy; benzodiazepines enhance GABA |
| Glutamate | Excitatory | Widespread in CNS | Primary excitatory NT; learning, memory (LTP) | Excess causes excitotoxicity (stroke) |
| Norepinephrine | Excitatory/Modulatory | Locus coeruleus, SNS | Alertness, attention, fight-or-flight | ↓ in Depression |
| Glycine | Inhibitory | Spinal cord, brainstem | Inhibitory control of motor neurons | Blocked by strychnine → tetanic spasms |
7. THE BRAIN
The adult brain weighs approximately 1,400 grams and consumes about 20% of the body's total oxygen and glucose despite being only 2% of body weight. It is organized into the cerebrum, diencephalon, brainstem, and cerebellum.
A. Cerebrum
The largest part of the brain, divided into two hemispheres (left and right) connected by the corpus callosum. The outer surface is the cerebral cortex (grey matter, ~2-4 mm thick), thrown into folds called gyri and grooves called sulci.
Four Lobes and Their Functions:
| Lobe | Location | Primary Functions |
|---|
| Frontal | Anterior | Voluntary motor control (primary motor cortex, precentral gyrus), executive function, personality, decision-making, Broca's area (speech production) |
| Parietal | Superior posterior | Somatosensory processing (primary sensory cortex, postcentral gyrus), spatial awareness, body image, reading |
| Temporal | Lateral | Auditory processing, memory (hippocampus), Wernicke's area (language comprehension), object recognition |
| Occipital | Posterior | Visual processing (primary visual cortex) |
Important Cortical Areas:
- Primary Motor Cortex (precentral gyrus, frontal lobe) - voluntary movement
- Primary Somatosensory Cortex (postcentral gyrus, parietal lobe) - sensory perception
- Broca's Area (left inferior frontal gyrus) - speech production; damage → Broca's (expressive) aphasia
- Wernicke's Area (left superior temporal gyrus) - language comprehension; damage → Wernicke's (receptive) aphasia
B. Diencephalon
Thalamus:
- Located at the center of the brain; paired egg-shaped structures flanking the 3rd ventricle
- The "relay station" and "gateway" to the cerebral cortex
- All sensory information (except smell/olfaction) passes through the thalamus before reaching the cortex
- Key nuclei: Lateral Geniculate (vision), Medial Geniculate (hearing), VPL/VPM (somatosensation)
Hypothalamus:
- Located below the thalamus; small but enormously important
- Controls the pituitary gland (master endocrine gland) via releasing/inhibiting hormones
- Regulates: body temperature, hunger, thirst, circadian rhythms, sleep-wake cycles, sexual behavior, emotional responses
- Contains centers for the ANS
- Key nuclei: suprachiasmatic (circadian), arcuate (hunger), supraoptic/paraventricular (ADH, oxytocin)
C. Brainstem
The brainstem connects the cerebrum to the spinal cord and contains vital centers for life support. It has three parts:
Midbrain (Mesencephalon):
- Contains the substantia nigra (dopamine-producing; degenerated in Parkinson's disease)
- Controls eye movements (CN III, CN IV nuclei), pupillary reflex
- Superior colliculi - visual reflexes | Inferior colliculi - auditory reflexes
- Reticular formation begins here
Pons:
- Means "bridge" - connects midbrain to medulla; connects cerebellum to brainstem
- Contains nuclei for CN V, VI, VII, VIII
- Pneumotaxic and apneustic centers - regulate breathing rhythm
- Important in sleep regulation (REM sleep)
Medulla Oblongata:
- Most caudal part; continuous with spinal cord at foramen magnum
- Contains vital centers:
- Cardiac center - heart rate and force
- Respiratory center - rhythmic breathing (dorsal and ventral respiratory groups)
- Vasomotor center - blood pressure via vascular tone
- Reflex centers: vomiting, swallowing, coughing, sneezing, hiccupping
- Contains nuclei for CN IX, X, XI, XII
- Site of pyramidal decussation - corticospinal tracts cross here
D. Cerebellum
- Located posterior to the brainstem in the posterior cranial fossa
- Two hemispheres + central vermis; highly folded cortex (folia)
- Functions: coordination of movement, balance, posture, motor learning, fine-tuning of voluntary movements
- Does NOT initiate movement - it compares intended vs. actual movement and corrects errors
- Damage (cerebellar lesions) → Ataxia (uncoordinated gait), dysmetria (past-pointing), intention tremor, nystagmus, dysdiadochokinesia
8. VENTRICLES AND CEREBROSPINAL FLUID (CSF)
The Ventricular System
The brain contains four fluid-filled cavities called ventricles:
Two Lateral Ventricles (one in each cerebral hemisphere)
↓ (through Interventricular Foramen of Monro)
Third Ventricle (diencephalon)
↓ (through Cerebral Aqueduct of Sylvius)
Fourth Ventricle (between pons/medulla and cerebellum)
↓ (through Foramina of Magendie and Luschka)
Subarachnoid Space → Circulation around brain and spinal cord
↓ (absorbed at)
Arachnoid Villi/Granulations into venous sinuses
CSF - Cerebrospinal Fluid
| Property | Value |
|---|
| Appearance | Clear, colorless ("water-like") |
| Total Volume | ~150 mL at any time |
| Production Rate | ~500 mL/day (replaced 3-4 times daily) |
| Production Site | Choroid plexus (ependymal cells) in lateral, 3rd, and 4th ventricles |
| Reabsorption Site | Arachnoid granulations (villi) into superior sagittal sinus |
| Pressure | 70-180 mmH₂O (lying) |
Composition (vs. plasma):
- Very low protein (~0.35 mg/mL vs. 70 mg/mL in plasma)
- No RBCs (normally)
- Glucose ~60% of plasma glucose
- Na⁺, Cl⁻ slightly higher; K⁺ lower than plasma
Functions of CSF
- Mechanical protection (Cushioning): Acts as a shock absorber for brain and spinal cord against physical trauma
- Buoyancy: The brain effectively weighs only ~50g in CSF versus 1,400g in air - prevents crushing of inferior brain under its own weight
- Waste removal: Removes metabolic waste products from the CNS extracellular space
- Nutrient delivery: Carries nutrients (glucose, amino acids) to neural tissue
- Intracranial pressure regulation: Maintains constant chemical environment for neurons
- Immune surveillance: Contains immunoglobulins and immune cells
Clinical Application: CSF examination via lumbar puncture is used to diagnose meningitis (↑ WBC, ↑ protein, ↓ glucose in bacterial meningitis), subarachnoid hemorrhage (xanthochromia = yellow CSF), and multiple sclerosis (oligoclonal bands).
9. MENINGES
The brain and spinal cord are enclosed by three concentric protective membranes called the meninges (from outermost to innermost):
SKULL / VERTEBRAL CANAL
↓
[Epidural Space - fat + epidural veins in spine]
↓
DURA MATER (tough, fibrous outer layer)
↓
[Subdural Space - potential space]
↓
ARACHNOID MATER (thin, avascular, spider-web like)
↓
[SUBARACHNOID SPACE - contains CSF + blood vessels]
↓
PIA MATER (delicate, closely adherent to brain surface)
↓
BRAIN / SPINAL CORD
| Layer | Structure | Key Features |
|---|
| Dura Mater | Thick, tough, fibrous; two layers intracranially (periosteal + meningeal) | Forms dural folds: Falx cerebri (between hemispheres), Tentorium cerebelli (between cerebrum/cerebellum), Falx cerebelli. Contains venous sinuses (sagittal, cavernous, transverse). |
| Arachnoid Mater | Thin, avascular membrane resembling spider web; trabeculations cross subarachnoid space | Subarachnoid space below it contains CSF. Arachnoid granulations absorb CSF into venous sinuses. |
| Pia Mater | Thinnest, most delicate layer; directly adherent to brain surface; follows all sulci and gyri | Carries blood vessels into brain substance. Cannot be separated from brain tissue. |
Clinical Relevance:
- Epidural hematoma: Blood in epidural space (usually arterial - middle meningeal artery rupture); lens-shaped on CT
- Subdural hematoma: Blood in subdural space (venous - bridging vein rupture); crescent-shaped on CT
- Subarachnoid hemorrhage: Blood in subarachnoid space (berry aneurysm rupture); "worst headache of life"
- Meningitis: Inflammation of meninges; signs include nuchal rigidity, Kernig's sign, Brudzinski's sign
10. SPINAL CORD
Structure
The spinal cord extends from the foramen magnum to approximately L1-L2 vertebral level in adults (conus medullaris). Below this, nerve roots form the cauda equina ("horse's tail").
- Length: ~45 cm; diameter ~1-1.5 cm
- Cervical and lumbar enlargements: Areas of increased thickness supplying the limbs
Cross-Sectional Organization:
WHITE MATTER (outer ring) - myelinated axon tracts
┌────────────────────┐
│ Posterior │ ← Dorsal columns (sensory tracts)
│ White matter │
WHITE │ ┌──────────────┐ │ WHITE
MATTER │ │ GREY MATTER │ │ MATTER
(Lateral│ │ H-SHAPED │ │ (Lateral
columns)│ │ │ │ columns)
│ │ Posterior │ │
│ │ horn (sens) │ │
│ │ Lateral horn│ │ ← ANS neurons (T1-L2, S2-S4)
│ │ Anterior │ │
│ │ horn (motor)│ │
│ └──────────────┘ │
│ Anterior │
│ White matter │ ← Corticospinal tract (motor)
└────────────────────┘
Grey Matter Horns:
- Dorsal (Posterior) Horn - Contains sensory neuron cell bodies and interneurons; receives afferent input
- Ventral (Anterior) Horn - Contains lower motor neuron (LMN) cell bodies; sends motor commands to muscles
- Lateral Horn (T1-L2 and S2-S4 only) - Contains preganglionic ANS neurons
Major Spinal Cord Tracts
Ascending (Sensory) Tracts:
| Tract | Location | Sensation Carried |
|---|
| Spinothalamic tract (anterior + lateral) | Anterolateral white matter | Pain, temperature, crude touch, pressure |
| Dorsal columns (Fasciculus gracilis + cuneatus) | Posterior white matter | Fine touch, vibration, two-point discrimination, proprioception (conscious) |
| Spinocerebellar tract | Lateral white matter | Proprioception (unconscious) to cerebellum |
Descending (Motor) Tracts:
| Tract | Location | Function |
|---|
| Lateral corticospinal tract | Lateral white matter | Voluntary movement of limbs (crossed - from opposite motor cortex) |
| Anterior corticospinal tract | Anterior white matter | Voluntary movement of trunk (uncrossed) |
| Rubrospinal, vestibulospinal, reticulospinal | Various | Posture, balance, muscle tone |
Reflex Arc
A reflex is an automatic, involuntary, stereotyped response to a stimulus. The pathway involved is called the reflex arc.
Five Components of a Reflex Arc:
STIMULUS
↓
1. RECEPTOR (sensory nerve ending detects stimulus)
↓
2. AFFERENT (SENSORY) NERVE (carries impulse to spinal cord)
↓
3. INTEGRATION CENTER (spinal cord interneurons process input)
↓
4. EFFERENT (MOTOR) NERVE (carries command to effector)
↓
5. EFFECTOR (muscle contracts or gland secretes = RESPONSE)
Important Reflexes:
| Reflex | Spinal Level | Stimulus | Response | Clinical Use |
|---|
| Patellar (Knee Jerk) | L3-L4 | Tap patellar tendon | Quadriceps contracts, knee extends | Tests L3-L4 integrity |
| Ankle Jerk | S1-S2 | Tap Achilles tendon | Gastrocnemius contracts, plantar flexion | Tests S1-S2 integrity |
| Biceps Reflex | C5-C6 | Tap biceps tendon | Biceps contracts, elbow flexion | Tests C5-C6 integrity |
| Withdrawal Reflex | Multiple | Painful stimulus | Flexion of affected limb + extension of opposite | Protective reflex |
| Babinski Sign | Corticospinal | Stroke lateral sole | Normal: plantar flexion. Abnormal (Babinski +): big toe dorsiflexion, fanning of toes → upper motor neuron lesion | |
The key clinical significance of spinal reflexes is that they continue even if higher centers are damaged. Testing reflexes maps the integrity of specific spinal cord segments.
11. CRANIAL NERVES (12 Pairs)
Cranial nerves arise directly from the brain and brainstem (not spinal cord, except CN XI which has a spinal component). They exit through foramina in the skull base.
Mnemonic to Remember the Names:
"Oh, Oh, Oh, To Touch And Feel Very Good Velvet, Ah Heaven"
(Olfactory, Optic, Oculomotor, Trochlear, Trigeminal, Abducens, Facial, Vestibulocochlear, Glossopharyngeal, Vagus, Accessory, Hypoglossal)
The 12 Cranial Nerves:
| # | Name | Type | Origin | Function | Key Clinical Point |
|---|
| I | Olfactory | Sensory | Olfactory bulb | Smell (olfaction) | Anosmia after head injury |
| II | Optic | Sensory | Lateral geniculate (diencephalon) | Vision | Optic neuritis in MS |
| III | Oculomotor | Motor | Midbrain | Eye movement (4 of 6 extraocular muscles), eyelid (levator palpebrae), pupil constriction, lens accommodation | CN III palsy = ptosis, eye "down and out", dilated pupil |
| IV | Trochlear | Motor | Midbrain (posterior) | Superior oblique muscle (down-and-inward eye movement) | Weakest CN, longest intracranial course |
| V | Trigeminal | Mixed | Pons | Sensation of entire face (3 divisions: V1 ophthalmic, V2 maxillary, V3 mandibular); muscles of mastication (chewing) | Trigeminal neuralgia (severe facial pain) |
| VI | Abducens | Motor | Pons | Lateral rectus muscle (abduction of eye) | Medial deviation in CN VI palsy |
| VII | Facial | Mixed | Pons | Facial expression muscles; taste (anterior 2/3 of tongue); lacrimation, salivation | Bell's Palsy = ipsilateral facial paralysis |
| VIII | Vestibulocochlear | Sensory | Pons-medulla junction | Hearing (cochlear division); balance/equilibrium (vestibular division) | Acoustic neuroma (vestibular schwannoma) |
| IX | Glossopharyngeal | Mixed | Medulla | Taste (posterior 1/3 tongue); swallowing; parotid gland; baroreceptor input from carotid sinus | Gag reflex (afferent limb) |
| X | Vagus | Mixed | Medulla | Longest cranial nerve; heart, lungs, GI tract (parasympathetic); pharynx/larynx (voice, swallowing); taste (epiglottis) | Damage → hoarse voice, dysphagia, tachycardia |
| XI | Accessory (Spinal Accessory) | Motor | Medulla + C1-C5 spinal | Sternocleidomastoid (head turning) and trapezius (shoulder shrug) | Damage → can't shrug shoulder or turn head |
| XII | Hypoglossal | Motor | Medulla | All intrinsic and extrinsic tongue muscles | Damage → tongue deviates toward lesion side |
Mixed nerves (Sensory + Motor): CN V, VII, IX, X
12. SPINAL NERVES (31 Pairs)
Spinal nerves are formed by the union of a dorsal (sensory) root and a ventral (motor) root. They exit through intervertebral foramina.
| Region | Number of Pairs | Spinal Level |
|---|
| Cervical | 8 pairs | C1 - C8 |
| Thoracic | 12 pairs | T1 - T12 |
| Lumbar | 5 pairs | L1 - L5 |
| Sacral | 5 pairs | S1 - S5 |
| Coccygeal | 1 pair | Co1 |
| TOTAL | 31 pairs | |
Major Nerve Plexuses:
| Plexus | Spinal Levels | Region Supplied |
|---|
| Cervical Plexus | C1-C4 | Neck, scalp, diaphragm (phrenic nerve C3,C4,C5) |
| Brachial Plexus | C5-T1 | Entire upper limb; branches: musculocutaneous, median, ulnar, radial, axillary nerves |
| Lumbar Plexus | L1-L4 | Anterior thigh; branches: femoral, obturator |
| Sacral Plexus | L4-S3 | Posterior thigh, entire leg and foot; largest nerve = sciatic nerve (L4-S3) |
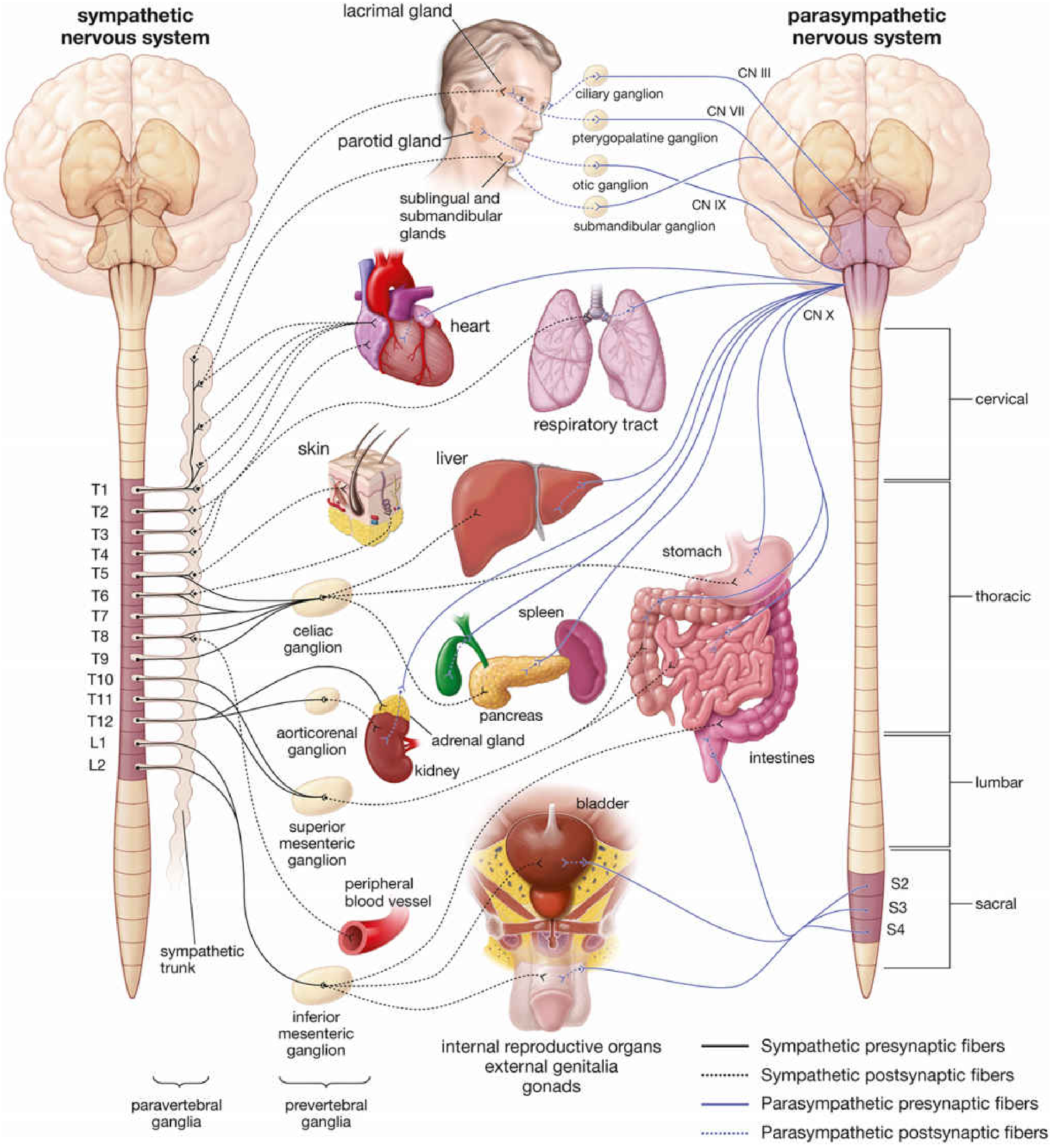
13. AUTONOMIC NERVOUS SYSTEM (ANS)
The ANS controls involuntary functions of smooth muscle, cardiac muscle, and glands. It operates largely below the level of consciousness.
Organization
The ANS uses a two-neuron chain:
- Preganglionic neuron: Cell body in CNS; myelinated axon
- Postganglionic neuron: Cell body in peripheral ganglion; unmyelinated axon → effector organ
Sympathetic vs. Parasympathetic - Complete Comparison
| Feature | Sympathetic ("Fight or Flight") | Parasympathetic ("Rest and Digest") |
|---|
| Origin (Outflow) | Thoracolumbar (T1-L2) | Craniosacral (CN III, VII, IX, X; S2-S4) |
| Preganglionic length | Short (ganglia near spinal cord) | Long (ganglia near/in target organ) |
| Postganglionic length | Long | Short |
| Ganglia location | Paravertebral (sympathetic trunk) and prevertebral | Terminal ganglia (near or within target organs) |
| Preganglionic NT | Acetylcholine (nicotinic receptor) | Acetylcholine (nicotinic receptor) |
| Postganglionic NT | Norepinephrine (adrenergic) [exception: sweat glands use ACh] | Acetylcholine (muscarinic receptor) |
| Heart rate | ↑ Increases (positive chronotropy) | ↓ Decreases (negative chronotropy) |
| Blood pressure | ↑ Increases (vasoconstriction) | ↓ Minimal direct effect |
| Bronchi | Dilates (bronchodilation) | Constricts (bronchoconstriction) |
| GI tract motility | ↓ Decreases (sphincters contract) | ↑ Increases (sphincters relax, peristalsis) |
| Pupils | Mydriasis (dilation) | Miosis (constriction) |
| Salivation | Scanty, thick saliva | Profuse, watery saliva |
| Sweating | Stimulates (cholinergic) | No effect |
| Bladder | Relaxes detrusor; contracts internal sphincter (urine retention) | Contracts detrusor; relaxes sphincter (micturition) |
| Sexual function | Ejaculation | Erection ("Point and Shoot" mnemonic: Parasympathetic = erection, Sympathetic = ejaculation) |
| Adrenal medulla | Secretes epinephrine and norepinephrine (acts like sympathetic postganglionic) | No direct innervation |
| Metabolic effects | Glycogenolysis, lipolysis (mobilizes energy) | Glycogen synthesis |
"The sympathetic and parasympathetic divisions of the ANS often supply the same organs. In these cases, the actions of the two are usually antagonistic. For example, sympathetic stimulation increases the rate of cardiac muscle contractions, whereas parasympathetic stimulation reduces the rate." - Ross & Pawlina Histology
14. REFLEX ACTION
A reflex is an automatic, rapid, stereotyped, involuntary response to a specific stimulus. The neural pathway is the reflex arc.
Importance of Reflexes
- Faster than voluntary responses (no conscious cortical processing needed)
- Protective function (withdrawal from pain)
- Maintain posture and balance (stretch reflexes)
- Diagnostic tools (testing reflexes reveals neurological deficits at specific spinal levels)
Types of Reflexes
| Type | Example | Description |
|---|
| Monosynaptic (stretch reflex) | Patellar (knee jerk) | Sensory neuron synapses directly on motor neuron - only ONE synapse |
| Polysynaptic | Withdrawal reflex | Multiple interneurons between sensory and motor neurons |
| Somatic | Knee jerk, withdrawal | Effector is skeletal muscle |
| Visceral (Autonomic) | Pupillary light reflex, baroreceptor reflex | Effector is smooth muscle, cardiac muscle, or gland |
| Ipsilateral | Withdrawal | Response on same side as stimulus |
| Contralateral | Crossed extensor reflex | Response on opposite side |
The Stretch Reflex (Myotatic Reflex) in Detail
When a muscle is stretched:
- Muscle spindles (intrafusal fibers) detect stretch
- Ia afferent neurons carry signal to spinal cord
- Synapse directly on alpha motor neurons (monosynaptic)
- Motor neuron fires → muscle contracts (resists further stretch)
- Simultaneously, Ia inhibitory interneurons inhibit the antagonist muscle (reciprocal inhibition)
This is the basis of all deep tendon reflexes (DTRs) tested clinically.
15. CLINICAL DISORDERS OF THE NERVOUS SYSTEM
1. Stroke (Cerebrovascular Accident - CVA)
| Feature | Detail |
|---|
| Definition | Sudden interruption of blood supply to part of the brain |
| Types | Ischemic (85%) - clot; Hemorrhagic (15%) - bleed |
| Cause | Thrombosis, embolism, or hemorrhage |
| Symptoms | Sudden unilateral weakness/numbness, facial droop, slurred speech (dysarthria/aphasia), visual disturbance, sudden severe headache (hemorrhage) |
| Mnemonic | FAST - Face drooping, Arm weakness, Speech difficulty, Time to call emergency |
| Key Principle | "Time is Brain" - every minute, ~1.9 million neurons die without treatment |
| Treatment | tPA (thrombolysis) for ischemic within 4.5 hrs; thrombectomy; BP control |
2. Meningitis
| Feature | Detail |
|---|
| Definition | Inflammation of the meninges |
| Causes | Bacterial (Neisseria meningitidis, Streptococcus pneumoniae), Viral (enterovirus), Fungal (Cryptococcus) |
| Symptoms | Triad: Fever + Severe headache + Neck stiffness (nuchal rigidity) + Photophobia |
| Signs | Kernig's sign (can't extend knee when hip flexed), Brudzinski's sign (neck flexion causes involuntary leg flexion) |
| Diagnosis | Lumbar puncture: ↑ WBC, ↑ protein, ↓ glucose (bacterial); ↑ lymphocytes, normal glucose (viral) |
| Treatment | Immediate IV antibiotics (do not wait for LP if clinical picture clear); Dexamethasone to reduce inflammation |
3. Parkinson's Disease
| Feature | Detail |
|---|
| Pathology | Progressive degeneration of dopaminergic neurons in substantia nigra (midbrain). Presence of Lewy bodies (α-synuclein inclusions) |
| Neurotransmitter | Dopamine ↓ → loss of inhibition of basal ganglia → excess inhibition of movement |
| Clinical Triad | TRAP: Tremor (resting, pill-rolling), Rigidity (cogwheel), Akinesia/Bradykinesia, Postural instability |
| Other features | Festinating gait, masked facies, micrographia, slurred speech, autonomic dysfunction, dementia (late) |
| Treatment | L-DOPA + Carbidopa (carbidopa prevents peripheral conversion); Dopamine agonists; MAO-B inhibitors; Deep Brain Stimulation (DBS) |
4. Alzheimer's Disease
| Feature | Detail |
|---|
| Definition | Most common cause of dementia; progressive neurodegenerative disorder |
| Pathology | Amyloid plaques (extracellular β-amyloid deposits) + Neurofibrillary tangles (intracellular hyperphosphorylated tau protein). Loss of cholinergic neurons in basal nucleus of Meynert |
| Neurotransmitter | Acetylcholine ↓ |
| Clinical | Progressive memory loss (recent > remote), language difficulties, disorientation, personality changes, eventually complete dependence |
| Risk Factors | Age (>65), family history, ApoE4 gene, Down syndrome (trisomy 21 - amyloid precursor protein gene on chromosome 21) |
| Treatment | AChE inhibitors (donepezil, rivastigmine, galantamine) - symptomatic; Memantine (NMDA antagonist) for moderate-severe; no cure |
5. Epilepsy
| Feature | Detail |
|---|
| Definition | Disorder characterized by recurrent, unprovoked seizures due to abnormal synchronized electrical activity in the brain |
| Pathophysiology | Imbalance between excitation (glutamate) and inhibition (GABA) - either GABA ↓ or glutamate ↑ |
| Seizure Types | Focal (localized cortex) vs. Generalized (whole brain); Absence (petit mal - brief staring spells), Tonic-clonic (grand mal - loss of consciousness + convulsions) |
| Diagnosis | EEG (electroencephalogram) - abnormal spike-wave discharges |
| Treatment | Anti-epileptic drugs (AEDs): Valproate, Phenytoin, Carbamazepine, Levetiracetam, Clonazepam; mechanism varies - Na⁺ channel blockers, GABA enhancers, Ca²⁺ channel blockers |
6. Multiple Sclerosis (MS)
| Feature | Detail |
|---|
| Definition | Autoimmune demyelinating disease of the CNS white matter |
| Pathology | Immune attack on myelin (produced by oligodendrocytes) → plaques (sclerosis) in white matter → slowed/blocked conduction; axonal damage in late stages |
| Demographics | Young adults (20-40 years), female > male (2:1), higher prevalence in temperate climates |
| Symptoms | Highly variable: Optic neuritis (blurred vision, painful eye movement - common first symptom), limb weakness, sensory disturbance (tingling, numbness), ataxia, bladder dysfunction, Uhthoff's phenomenon (symptoms worsen with heat), Lhermitte's sign (electric shock down spine on neck flexion) |
| Patterns | Relapsing-Remitting MS (RRMS, 85%) - attacks + recovery; Secondary/Primary Progressive MS |
| Diagnosis | MRI (periventricular white matter lesions - "Dawson's fingers"), CSF (oligoclonal bands), VEPs |
| Treatment | Acute relapse: IV Methylprednisolone; Disease-modifying therapies: Interferon-β, Glatiramer, Natalizumab, Ocrelizumab |
QUICK REVISION SUMMARY
NS = CNS (Brain + Spinal Cord) + PNS (Cranial 12 + Spinal 31) + ANS (Symp + Parasymp)
NEURON: Cell body → Axon hillock → Axon → Terminal buttons
Dendrites receive; Axons transmit
Types: Sensory (Afferent) | Motor (Efferent) | Interneuron (99.9%)
GLIA: CNS: Astrocyte, Oligodendrocyte (myelin), Microglia (immune), Ependymal (CSF)
PNS: Schwann cells (myelin), Satellite cells
AP: RMP = -70 mV → Threshold -55 mV → Na⁺ in (depolarization to +35 mV)
→ Na⁺ channels close, K⁺ out (repolarization) → Hyperpolarization → Rest
SYNAPSE: Ca²⁺ → Vesicle fusion → NT release → Receptor binding
Excitatory (Na⁺ in) = EPSP | Inhibitory (Cl⁻ in) = IPSP
BRAIN: Cerebrum (thinking) > Cerebellum (coordination) > Brainstem (vital)
Thalamus (relay) | Hypothalamus (homeostasis)
CSF: Made by Choroid Plexus (ependymal cells) | 500mL/day | 150mL total
Absorbed by Arachnoid granulations | Lateral→3rd→Aqueduct→4th→Subarachnoid
MENINGES (outside→in): Dura → Arachnoid → Pia | CSF in Subarachnoid space
CRANIAL NERVES: 12 pairs | Sensory: I, II, VIII | Motor: III, IV, VI, XI, XII
Mixed: V, VII, IX, X | Longest = Vagus (X)
SPINAL NERVES: 31 pairs = C8 + T12 + L5 + S5 + Co1
ANS: Sympathetic = T1-L2, Norepinephrine postganglionic, "Fight or Flight"
Parasympathetic = Craniosacral (CN III/VII/IX/X + S2-S4), ACh, "Rest & Digest"
DISORDERS:
Stroke = "Time is Brain" | Meningitis = Fever+Headache+Stiff neck
Parkinson = Dopamine↓, TRAP triad | Alzheimer = ACh↓, amyloid plaques
Epilepsy = GABA↓/Glutamate↑ | MS = CNS demyelination (oligodendrocytes)
Sources: - Histology: A Text and Atlas, Ross & Pawlina, 8th Ed. | - Guyton and Hall Medical Physiology, 14th Ed. | - Ganong's Review of Medical Physiology, 26th Ed. | - Principles of Neural Science, Kandel, 6th Ed. | - Medical Physiology, Boron & Boulpaep, 3rd Ed.