What is vasectomy
Reading File
Searching the Web
vasectomy procedure male sterilization overview
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a thorough overview of vasectomy based on leading urology textbooks:
Vasectomy
What Is It?
A vasectomy is a safe, effective, and permanent method of male contraception that works by interrupting the flow of sperm through the vas deferens - the tubes that carry sperm from the testes toward the urethra. Without sperm reaching the ejaculate, fertilization cannot occur.
In 2015, approximately 520,000 vasectomies were performed in the United States alone. It is most commonly performed in an office setting by a urologist, on men aged 25-44 years. - Campbell-Walsh-Wein Urology
Anatomy
The vas deferens runs along the posteromedial aspect of the spermatic cord. It has thick walls of smooth muscle, giving it a firm, almost "hard-cooked spaghetti noodle" feel on palpation - about 3 mm in diameter. It lies deep within the scrotum, beneath nine tissue layers, surrounded by its own small artery (the deferential artery) and vasal nerves.
Here is a cross-section of the spermatic cord showing the key structures:
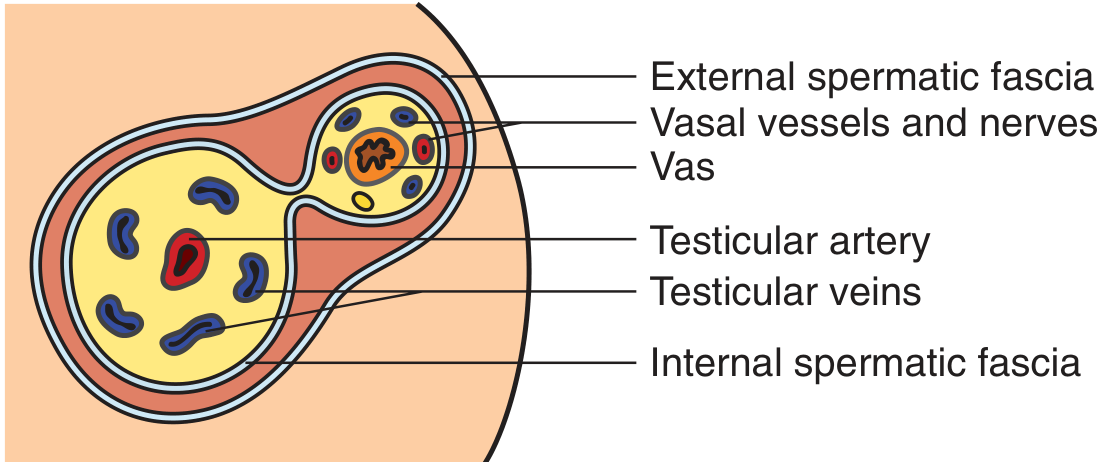
Schematic coronal view of the spermatic cord - note the vas deferens with its associated vessels and nerves within the internal spermatic fascia. - Pfenninger & Fowler's Procedures for Primary Care
The Two Key Surgical Steps
Every vasectomy involves two main steps:
- Vas isolation - accessing and isolating the vas deferens
- Vas occlusion - cutting, ligating, cauterizing, or blocking the vas
Methods of Vas Isolation
| Method | Description |
|---|---|
| Conventional Vasectomy (CV) | A 1.5-3 cm scrotal incision is made; the vas is grasped with a towel clamp or Allis forceps. Used when anatomy is challenging (prior surgery, thick scrotal skin, varicocele). |
| No-Scalpel Vasectomy (NSV) | A minimally invasive technique using a small puncture instead of an incision. Associated with less discomfort, fewer complications, and faster recovery. Preferred technique. |
The AUA recommends minimally invasive techniques (like NSV) as the standard of care because of their lower complication profile. - Campbell-Walsh-Wein Urology
Methods of Vas Occlusion
Several techniques exist to block the vas:
- Ligation (tying) with or without excision of a small segment
- Electrocautery of the lumen
- Metal or plastic clips
- Fascial interposition (placing a tissue layer between the two cut ends) - reduces risk of recanalization
- Mucosal fulguration - destroying the inner lining
Anesthesia
Vasectomy is performed under local anesthesia (1-2% lidocaine, with or without bupivacaine) using a fine 25-32 gauge needle to minimize injection pain. Oral sedation may be added. General anesthesia is reserved for patients where local anesthesia is not feasible. - Campbell-Walsh-Wein Urology
Pre-Procedure Counseling
Patients must be counseled on:
- The procedure is intended to be permanent - reversal is possible but not guaranteed
- Need for a post-vasectomy semen analysis (PVSA) to confirm success
- A 1-2% risk of needing a repeat vasectomy if PVSA shows persistent sperm
- A small risk of spontaneous recanalization (the two ends reconnecting), which can result in pregnancy
- 1-2% risk of chronic scrotal pain
Effectiveness
Vasectomy has a >99% success rate, making it one of the most effective contraceptive methods available. It is more effective than female tubal ligation for equal simplicity of procedure.
Complications
| Complication | Notes |
|---|---|
| Hematoma | Most common early complication |
| Infection | Uncommon; scrotal skin heals rapidly |
| Chronic scrotal pain | ~1-2% of men |
| Recanalization / failure | Rare; requires PVSA to detect |
| Sperm granuloma | Local reaction to leaked sperm |
Vasectomy vs. Tubal Ligation
Despite its simplicity and lower risk, vasectomy is less commonly used than female tubal ligation. In the US, ~13% of married women report relying on their partner's vasectomy vs. ~24% who rely on tubal ligation. This disparity reflects cultural factors, insurance coverage differences (lower Medicaid coverage of vasectomies), and marital status patterns. - Campbell-Walsh-Wein Urology
Reversal
Vasectomy reversal (vasovasostomy or epididymovasostomy) is possible but success depends heavily on the time elapsed since vasectomy - the longer the interval, the lower the patency and pregnancy rates. It should not be used as justification to proceed with a vasectomy in a man who is uncertain about permanence.
For a clear visual explanation of the procedure itself, this video is helpful:
This is a shared conversation. Sign in to Orris to start your own chat.