Explain the mechanism of sialolithiasis
Reading File
Finding Sources
Finding Sources
Searching PubMed
sialolithiasis pathogenesis mechanism
Reading File
Reading File
Reading File
Loading Image
Searching Images
sialolithiasis salivary gland stone mechanism formation diagram
I have all the information needed for a comprehensive answer. Let me compile it now.
Sialolithiasis — Mechanism of Stone Formation
Sialolithiasis is the formation of calculi (sialoliths) within the ductal system of the salivary glands. It is the most common cause of salivary gland inflammation. The precise etiology remains incompletely understood, but the following cascade of events is well established.
1. Anatomical and Salivary Predispositions
The submandibular gland (Wharton's duct) is affected in 80–90% of cases, with the parotid (Stensen's duct) accounting for 10–20%, and the sublingual duct for ~1%. This distribution reflects specific anatomical and biochemical properties that promote stasis:
| Factor | Submandibular | Parotid |
|---|---|---|
| Duct length | Longer | Shorter |
| Duct calibre | Wider | Narrower |
| Course | Tortuous, angulated against gravity around the mylohyoid muscle | More direct |
| Saliva viscosity | Higher (mucous acini) | Lower (serous acini) |
| Calcium/phosphate concentration | Higher | Lower |
These factors collectively slow salivary flow and promote stagnation.
2. The Core Pathogenic Sequence
Step 1 — Salivary stasis
Intermittent stagnation of saliva in the duct occurs due to the anatomical features above, or secondary to dehydration, anticholinergic medications (e.g., phenothiazines), or reduced oral intake.
Step 2 — Organic nidus formation
Stasis causes an alteration in the mucoid elements of saliva. The mucopolysaccharides and glycoproteins within saliva aggregate to form an organic gel matrix — this acts as the scaffold (nidus) upon which minerals are deposited.
Step 3 — Mineral deposition and stone growth
Calcium salts (predominantly calcium phosphate and calcium carbonate) deposit onto the organic nidus in concentric lamellae. Small amounts of magnesium, potassium, and ammonium salts also contribute. This process mirrors biomineralization seen in urinary and gallstones. Serum calcium and phosphate levels are not elevated — the process is locally driven, not systemic.
Step 4 — Ductal obstruction
The growing calculus obstructs salivary outflow, especially during meals when salivary secretion surges. This produces the classic postprandial salivary colic (pain and swelling that peaks with eating and subsides gradually).
3. The Sialolithiasis–Sialadenitis Relationship (Gland-Specific)
The relationship between stone formation and ductal inflammation differs by gland:
-
Submandibular gland: Sialolith formation is the primary event. The resulting obstruction causes salivary stasis, which then facilitates retrograde bacterial migration (commonly S. aureus, S. viridans, anaerobes) leading to secondary sialadenitis.
-
Parotid gland: Chronic sialadenitis is the inciting event — ductal injury and inflammation promote subsequent stone formation. Parotid stones tend to occur at the hilum or parenchyma rather than in the duct itself.
4. Histopathology
On light microscopy, a sialolith appears as a basophilic, amorphous mass with a layered or granular internal architecture. The surrounding duct shows dilatation (ductal ectasia) with periductal chronic inflammatory infiltrate — representing the tissue response to obstruction. If infection supervenes, the inflammation becomes acute and suppurative, potentially with abscess formation.
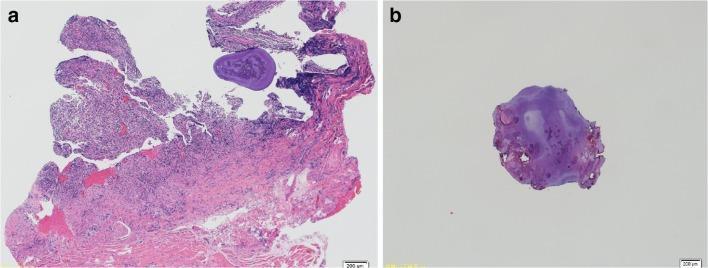
H&E section: the sialolith (basophilic amorphous mass) with surrounding ductal ectasia and chronic inflammatory infiltrate.
5. Ultrasound Appearance

US image of sialolithiasis: the bright hemi-circular echogenic structure is the calculus within the duct (Rosen's Emergency Medicine).
Summary
Anatomical stasis factors (long tortuous duct, anti-gravity course, viscous/high-Ca saliva)
↓
Intermittent salivary stagnation
↓
Mucoid element alteration → organic gel nidus formation
↓
Calcium phosphate/carbonate deposition onto nidus
↓
Growing sialolith → ductal obstruction
↓
Postprandial pain/swelling + retrograde bacterial sialadenitis
Sources:
- Cummings Otolaryngology Head and Neck Surgery, block 17
- Robbins, Cotran & Kumar: Pathologic Basis of Disease, block 8
- Tintinalli's Emergency Medicine: A Comprehensive Study, block 20
- Rosen's Emergency Medicine, block 10
This is a shared conversation. Sign in to Orris to start your own chat.