Thrombo philabitis anatomy, medicine, pathology, surgery
Reading File
Finding Sources
Finding Sources
Searching PubMed
thrombophlebitis treatment management
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive material from multiple authoritative textbooks. Let me compile the full answer.
Thrombophlebitis - A Comprehensive Review
Thrombophlebitis = simultaneous thrombosis (clot formation) + phlebitis (vein wall inflammation). It ranges from benign superficial disease to life-threatening deep vein thrombosis (DVT) and septic/suppurative forms.
1. ANATOMY
Lower Extremity Venous System
The venous anatomy of the lower extremity is divided into the deep and superficial systems.
Superficial system:
- Greater saphenous vein (GSV) - runs medially from the foot to the groin, joins the common femoral vein at the saphenofemoral junction (SFJ)
- Short (small) saphenous vein (SSV) - runs laterally, joins the popliteal vein at the saphenopopliteal junction (SPJ)
- Perforating veins - directly connect the saphenous system to the deep veins at various levels
Deep system (proximal to distal):
- Common femoral vein (formed at inguinal ligament)
- Femoral vein (previously called "superficial femoral vein" - a confusing old term since it IS a deep vein)
- Popliteal vein (below adductor canal)
- Calf veins: anterior tibial, posterior tibial, and peroneal veins
"Distal greater saphenous vein thrombi are often referred to as superficial thrombosis, but greater saphenous clots near the connection with the femoral vein should be referred to as DVT." - Rosen's Emergency Medicine
Classification of DVT by location:
- Distal DVT - calf veins only
- Proximal DVT - popliteal vein and above
- Iliofemoral DVT - femoral and iliac veins (highest risk)
Key anatomical fact: valves within veins prevent retrograde flow; when thrombosis forms, valves become incompetent and venous stasis worsens.
Intracranial Venous Anatomy (for Suppurative Thrombophlebitis)
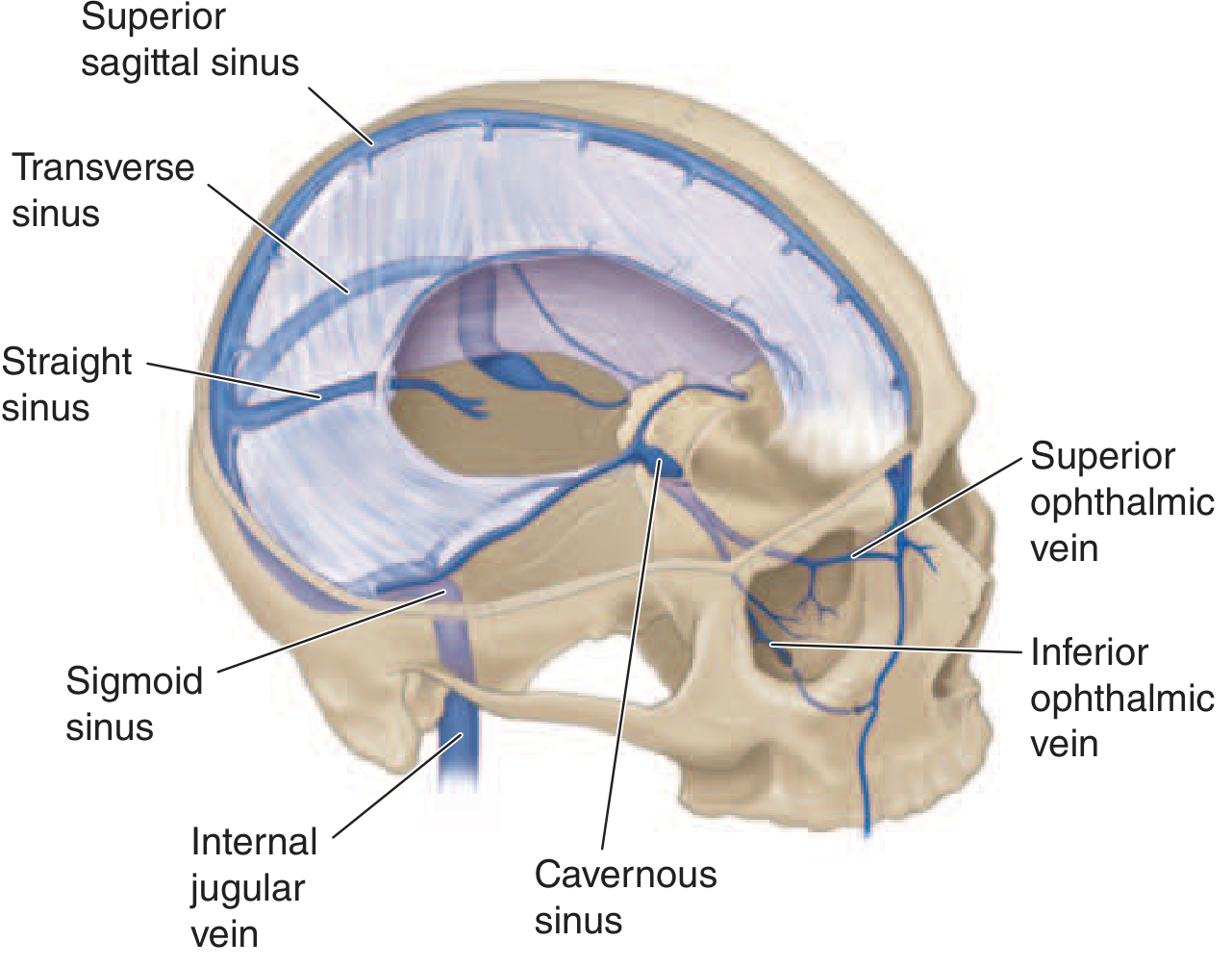
The cerebral sinuses have no valves, so blood can flow in either direction. The key structures are:
- Superior sagittal sinus - largest sinus; receives blood from frontal, parietal, and occipital superior cerebral veins and the diploic veins
- Transverse sinus - drains the superior sagittal sinus; also receives drainage from the middle ear and mastoid cells
- Sigmoid sinus - continuation of transverse sinus, drains into the internal jugular vein
- Cavernous sinus - at the skull base; receives blood from facial veins via the superior and inferior ophthalmic veins
The facial veins communicate with the cavernous sinus, which is why facial infections (furuncles, paranasal sinusitis) can spread intracranially.
2. PATHOLOGY (Virchow's Triad)
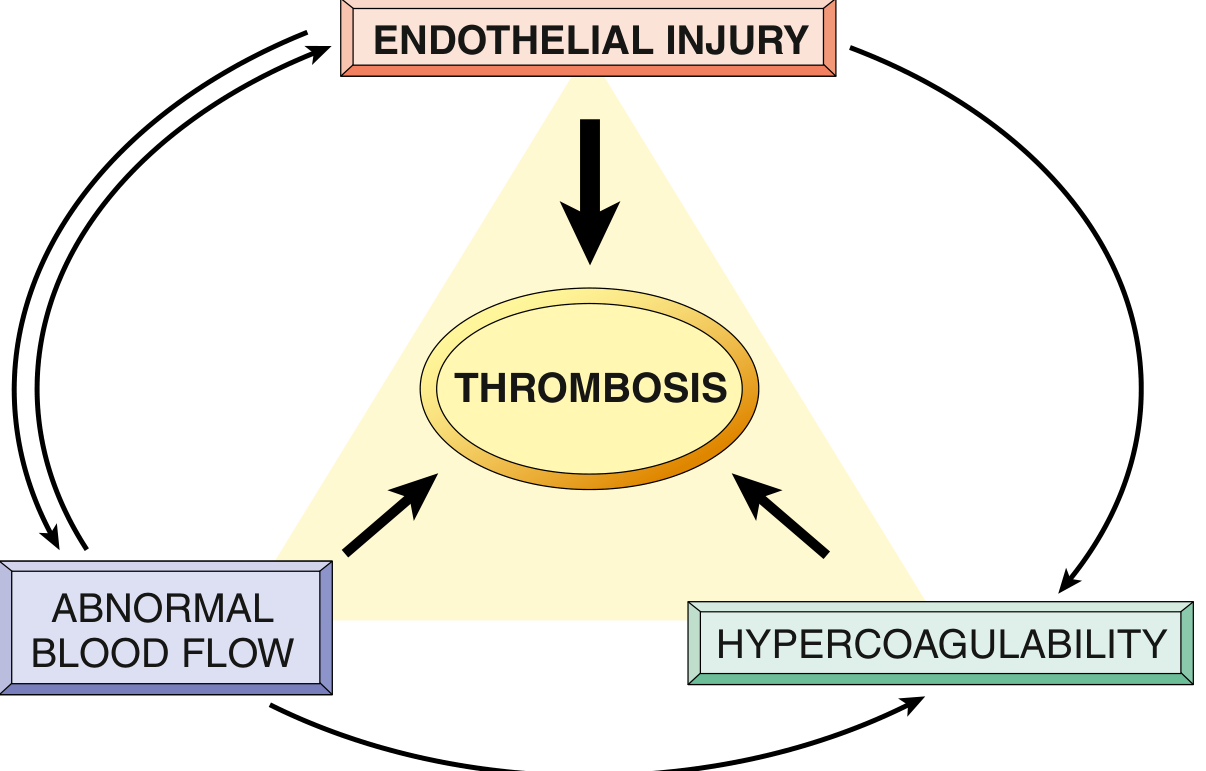
Thrombosis arises from one or more components of Virchow's triad (Robbins & Kumar Basic Pathology):
1. Endothelial Injury
- Most important factor in arterial thrombosis
- Injury exposes von Willebrand factor (vWF) and tissue factor
- Endothelial "activation" can occur from: physical injury, infections, cytokines, hypercholesterolemia, homocysteinemia, cigarette smoke toxins
- Activated endothelium: downregulates thrombomodulin, endothelial protein C receptor, TFPI; upregulates tissue factor and PAI (plasminogen activator inhibitors - inhibiting fibrinolysis)
2. Abnormal Blood Flow (Stasis / Turbulence)
- Stasis is the primary factor in venous thrombosis
- Stasis allows platelets and leukocytes to contact endothelium
- Slows the washout of activated clotting factors
- Prevents dilution by fresh flowing blood
- Common causes: prolonged immobility, heart failure, long-haul travel, varicose veins, pregnancy, cast immobilization
3. Hypercoagulability
Primary (genetic) causes:
| Factor | Risk Level |
|---|---|
| Factor V Leiden (Arg506Glu) | Common; ~3x venous thrombosis risk |
| Prothrombin G20210A variant | Common |
| Antithrombin deficiency | Rare; presents in adolescence |
| Protein C deficiency | Rare |
| Protein S deficiency | Rare |
| Homozygous homocystinuria | Very rare |
Secondary (acquired) causes - high risk:
- Prolonged bed rest / immobilization
- Surgery, fracture, burns
- Cancer (especially pancreatic, lung - Trousseau syndrome)
- Antiphospholipid syndrome
- Heparin-induced thrombocytopenia (HIT)
- Disseminated intravascular coagulation (DIC)
- Pregnancy / postpartum
- Oral contraceptive use
Thrombus Morphology
- Venous thrombi are red (red cell-rich) thrombi - formed under low flow, rich in red blood cells and fibrin
- They propagate in the direction of blood flow (proximally in legs)
- Fates: lysis, organization/recanalization, propagation, or embolism
3. MEDICINE (Clinical Presentation, Diagnosis, Treatment)
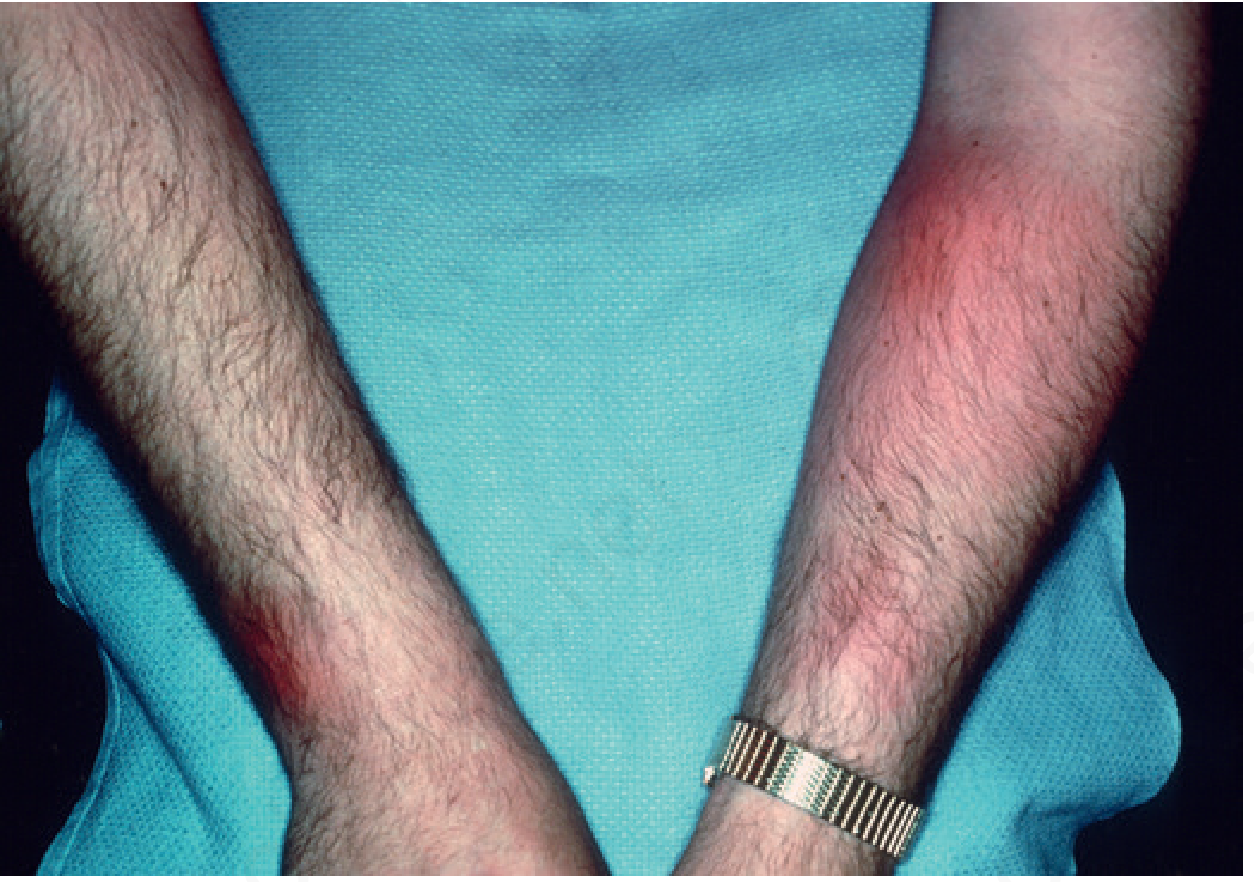
A. Superficial Thrombophlebitis (SVT)
Clinical features:
- Tender, red, indurated cord following the line of a superficial vein
- Most commonly the GSV
- Prevalence: 3-11% of the general population
- Associated with: malignancy, obesity, thrombophilia, pregnancy, estrogen use, varicose veins, IV catheters, sclerotherapy
Clinical photo - migratory superficial thrombophlebitis (Trousseau syndrome):
Important associations:
- Trousseau syndrome - migratory thrombophlebitis associated with occult malignancy (classically pancreatic or lung cancer)
- Mondor disease - SVT of the thoracoepigastric veins of the chest wall or breast; starts as a painful red cord, then becomes a painless fibrous band; 3x more common in women
- Thromboangiitis obliterans (Buerger disease) - recurrent SVT in young male smokers
Overlap with DVT: Up to 25% of patients with SVT have concomitant DVT or PE - duplex ultrasound is mandatory.
Diagnosis:
- Duplex ultrasonography - confirms SVT, excludes DVT, assesses valve competence
- Thrombophilia workup is not routine but indicated for recurrent or idiopathic SVT
- Screen for malignancy if clinically suspected
Medical treatment (Fuster & Hurst's The Heart, Mulholland & Greenfield's Surgery):
- Distal/limited SVT: NSAIDs, leg elevation, warm compresses, ambulation, compression
- SVT within 5 cm of SPJ or 10 cm of SFJ: anticoagulation required
- First-line anticoagulants: fondaparinux (CALISTO trial - most evidence) or LMWH
- DOAC alternative: rivaroxaban 10 mg/day x 6 weeks was non-inferior to fondaparinux in the SURPRISE trial, and is more patient-friendly
- Septic SVT: broad-spectrum IV antibiotics; excision if patient becomes septic
B. Deep Vein Thrombosis (DVT)
Clinical features:
- Classic: unilateral leg pain, swelling, erythema, warmth
- Up to 50% are asymptomatic
- Signs: Homan's sign (calf pain on dorsiflexion) - not reliable
Diagnosis:
- Duplex (compression + Doppler) ultrasound - first-line
- D-dimer - high negative predictive value; use with Wells score
- CT venography or MRI if iliac/IVC involvement suspected
Wells Pretest Probability Score for DVT - guides whether to go straight to ultrasound or use D-dimer first.
Treatment:
- Anticoagulation for minimum 3-6 months (provoked) or longer/indefinitely (unprovoked)
- Preferred agents: DOACs (rivaroxaban, apixaban) - first-line in most patients
- LMWH preferred in cancer-associated thrombosis
- IVC filter only for contraindication to anticoagulation
- Compression stockings to prevent post-thrombotic syndrome
C. Suppurative (Septic) Thrombophlebitis
Two main types:
- Peripheral septic SVT - usually from IV catheter infection (Staphylococcus aureus most common)
- Intracranial suppurative thrombophlebitis - complication of sinusitis, otitis media, mastoiditis, or facial infections (Harrison's 22E)
Intracranial forms and predisposing sources:
| Sinus | Primary Infection Source |
|---|---|
| Superior sagittal sinus | Bacterial meningitis, SDE |
| Transverse/sigmoid sinus | Otitis media, mastoiditis (via emissary veins) |
| Cavernous sinus | Sphenoid/ethmoid sinusitis, facial furuncles (via ophthalmic veins) |
Clinical presentation - intracranial:
- Superior sagittal sinus: headache, fever, seizures, stupor, bilateral leg weakness
- Cavernous sinus: CN III, IV, V, VI palsies; proptosis; chemosis; periorbital edema; fever
Diagnosis: MRI with MR venography (gold standard); CT venography
Treatment (Harrison's 22E):
- IV antibiotics x 6 weeks (pathogen-directed)
- Heparin anticoagulation - recommended; small intracerebral hemorrhage is NOT an absolute contraindication
- Surgical debridement for septic lateral/cavernous sinus thrombosis
- Thrombolytics (rtPA) and thrombectomy: insufficient data to recommend routinely
4. SURGERY
A. Indications for Surgical Intervention
Superficial vein excision/stripping:
- Suppurative SVT not responding to antibiotics - the infected vein segment must be excised
- Recurrent SVT in varicose veins - high ligation/stripping of GSV eliminates the source
DVT - surgical options (Fischer's Mastery of Surgery, Sabiston):
| Procedure | Indication |
|---|---|
| Catheter-directed thrombolysis (CDT) | Massive iliofemoral DVT with limb-threatening ischemia (phlegmasia cerulea dolens) |
| Surgical venous thrombectomy | Phlegmasia cerulea dolens unresponsive to CDT; iliofemoral DVT with severe symptoms |
| IVC filter placement | Contraindication to anticoagulation; recurrent PE despite adequate anticoagulation |
| Balloon venoplasty/stenting | Residual iliofemoral stenosis post-thrombectomy; May-Thurner syndrome (right iliac artery compression of left iliac vein) |
B. DVT Prophylaxis - Surgical Context
From Campbell's Operative Orthopaedics (2026):
- Without prophylaxis, DVT incidence after knee arthroscopy ranges from 1.8% to 41.2% (average 6.8%)
- With prophylaxis, incidence drops to 0.1%-11.9% (average 1.8%)
- Recommended: sequential compression devices (SCDs) during surgery, early active ROM, and aspirin postoperatively when weight-bearing is altered
- High-risk patients (known thrombophilia, prior VTE, prolonged immobility): LMWH prophylaxis
Virchow's triad in the surgical patient:
- Endothelial injury - from the operation itself
- Stasis - from immobility, anesthesia, tourniquet use
- Hypercoagulability - from the inflammatory response to surgery
C. Postoperative Thrombophlebitis
From Tintinalli's Emergency Medicine:
- Aseptic SVT: local heat, elevation, NSAIDs
- Suppurative SVT: requires excision of the affected vein (not just antibiotics alone)
- Always evaluate for concurrent DVT in postoperative patients with SVT
D. Phlegmasia
Two severe forms of massive DVT requiring urgent surgery:
- Phlegmasia alba dolens ("milk leg") - white, pale, edematous limb; collateral flow still present
- Phlegmasia cerulea dolens - blue, cyanotic, massively swollen limb; risk of venous gangrene if untreated; requires emergent CDT or surgical thrombectomy
Summary Table
| Type | Key Features | Diagnosis | Treatment |
|---|---|---|---|
| Superficial SVT (aseptic) | Tender cord, erythema along vein | Duplex US | NSAIDs, compression, heat |
| SVT near SFJ/SPJ | Same + risk of DVT extension | Duplex US | Fondaparinux or rivaroxaban x 6 wks |
| Septic SVT | Fever, sepsis, lymphangitis | Clinical + blood cx | IV antibiotics ± vein excision |
| DVT (distal) | Calf pain/swelling | Duplex US | Anticoagulation x 3 months |
| DVT (proximal) | Leg swelling, erythema, pain | Duplex US | Anticoagulation (DOAC preferred) |
| Phlegmasia cerulea dolens | Cyanosis, gangrene risk | Clinical + imaging | CDT / surgical thrombectomy |
| Suppurative intracranial | CN palsies, headache, fever | MRI/MRV | Antibiotics 6 wks + heparin |
Sources:
- Robbins & Kumar Basic Pathology (Virchow's triad, hypercoagulability)
- Harrison's Principles of Internal Medicine 22E (suppurative thrombophlebitis)
- Rosen's Emergency Medicine (anatomy, DVT/PE pathophysiology)
- Fuster & Hurst's The Heart 15E (superficial thrombophlebitis management)
- Mulholland & Greenfield's Surgery 7E (SVT treatment, CALISTO/SURPRISE trials)
- Andrews' Diseases of the Skin (superficial thrombophlebitis, Mondor disease)
- Campbell's Operative Orthopaedics 15E 2026 (surgical prophylaxis)
- Tintinalli's Emergency Medicine (postoperative thrombophlebitis)
Dangerous fungal infection of human body
Reading File
Finding Sources
Finding Sources
Searching PubMed
invasive fungal infections mortality immunocompromised
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have rich, comprehensive content from multiple authoritative textbooks. Let me compile the full detailed answer.
Dangerous Fungal Infections of the Human Body
Fungi are eukaryotic organisms that exist as either yeasts (unicellular, replicate by budding) or molds (multicellular filamentous, grow by hyphal branching). The most dangerous infections are the invasive/disseminated mycoses - they carry mortality rates of 30-90% even with treatment and primarily strike immunocompromised hosts.
Classification of Dangerous Fungi
| Category | Examples | Hyphae Type |
|---|---|---|
| Opportunistic yeasts | Candida, Cryptococcus | Yeast forms |
| Opportunistic molds (hyaline) | Aspergillus, Fusarium | Septate |
| Opportunistic molds (mucorales) | Rhizopus, Mucor | Aseptate/sparsely septate |
| Dematiaceous (black) molds | Cladosporium, Alternaria | Septate, melanin-pigmented |
| Dimorphic endemic fungi | Histoplasma, Coccidioides, Blastomyces | Mold at 25°C, yeast at 37°C |
1. INVASIVE CANDIDIASIS
Overview
Candidemia is the 3rd or 4th most common bloodstream infection in the United States, carrying a ~40% mortality. Candida albicans causes the majority, but C. tropicalis, C. parapsilosis, C. glabrata, and C. krusei together account for the remainder. Notably, Candida auris is an emerging multidrug-resistant species of global concern.
Risk Factors
- ICU stay (>3 days)
- Broad-spectrum antibiotics (gut dysbiosis allows Candida overgrowth)
- Central venous catheters
- Total parenteral nutrition (TPN)
- Abdominal surgery / gut perforation
- Renal replacement therapy
- Hematological malignancy / bone marrow transplant
- Immunosuppression (steroids, chemotherapy)
Virulence Mechanisms
- Forms biofilms on prosthetic devices (resistant to antifungals)
- Hyphae (germ tubes) - allows tissue invasion
- Secretes proteases and phospholipases to damage host cells
- Phenotypic switching - changes surface antigens to evade immunity
Clinical Forms
| Form | Key Features |
|---|---|
| Candidemia | Persistent fever despite antibiotics; sepsis; mortality ~40% |
| Invasive candidiasis | Dissemination to eye (endophthalmitis), heart (endocarditis), kidney, bone, meninges |
| Hepatosplenic candidiasis | "Chronic disseminated candidiasis" - in neutropenic patients recovering counts; hepatosplenomegaly, multiple micro-abscesses on CT |
| Candida endocarditis | Large vegetations; high embolic risk |
| Candida meningitis | Rare; most often in neonates or those with CSF shunts |
Diagnosis
- Blood cultures (sensitivity ~50% - often misses deep infection)
- Beta-D-glucan assay (panfungal marker)
- Ophthalmology exam (all candidemic patients)
- CT chest/abdomen for organ involvement
Treatment
- Echinocandins (caspofungin, micafungin, anidulafungin) - first-line for most invasive candidiasis
- Fluconazole - step-down therapy for fluconazole-susceptible strains after clinical improvement
- Amphotericin B (liposomal) - for CNS candidiasis; C. krusei (intrinsically fluconazole resistant)
- Remove all central lines if possible
- Duration: minimum 14 days after last positive blood culture
2. INVASIVE PULMONARY ASPERGILLOSIS (IPA)
Overview
Aspergillosis is the most common invasive mold infection worldwide. Aspergillus fumigatus is the primary pathogen; conidia are 2.5-3 μm - small enough to reach the alveoli on inhalation. The organism is found in soil, decaying vegetation, potted plants, pepper, and especially construction sites.
Pathogenesis
(Medical Microbiology 9e)
In the lungs, alveolar macrophages ingest conidia while neutrophils kill the germinated hyphae. When either arm fails:
- Hyphae germinate and invade pulmonary tissue
- Hyphae penetrate alveolar capillaries and pulmonary arterioles (angioinvasion)
- This causes intravascular thrombosis, local hypoxia, and coagulative necrosis (classic "infarct-like" lesions)
- Hematogenous dissemination can reach the brain - a catastrophic complication
Aspergillus secretes:
- Gliotoxin - inhibits macrophage phagocytosis and T-cell activation
- Elastase, phospholipase, proteases - aid tissue invasion
- Catalase - inactivates host-generated hydrogen peroxide (key in chronic granulomatous disease)
Risk Factors
- Prolonged severe neutropenia (acute myelogenous leukemia, hematopoietic cell transplant) - highest risk
- Hematopoietic stem cell transplant (HCT)
- Solid organ transplant (SOT) - especially lung transplant
- High-dose corticosteroids
- Chronic granulomatous disease (CGD)
- Advanced HIV
- Critically ill ICU patients (COPD, cirrhosis, severe influenza)
- Ibrutinib (Bruton tyrosine kinase inhibitor) therapy
Spectrum of Aspergillus Disease
| Form | Host | Characteristics |
|---|---|---|
| Allergic bronchopulmonary aspergillosis (ABPA) | Asthma / cystic fibrosis | Hypersensitivity reaction; eosinophilia; mucus plugging |
| Aspergilloma | Pre-existing lung cavity (TB, sarcoid) | "Fungus ball"; hemoptysis; non-invasive |
| Chronic pulmonary aspergillosis (CPA) | Mild immunocompromise | Slowly progressive; cavities; weight loss |
| Invasive pulmonary aspergillosis (IPA) | Severe immunosuppression | Angioinvasion; infarction; dissemination; high mortality |
Clinical Features (IPA)
- Fever not responding to antibiotics
- Pleuritic chest pain, hemoptysis
- Cough, dyspnea
- Halo sign on CT: nodule surrounded by ground-glass haze (early bleeding around infarcted area)
- Air crescent sign on CT: crescent of air around a necrotic nodule (late sign, seen with neutrophil recovery)
Diagnosis
- HRCT chest (halo sign, wedge-shaped infarcts, nodules)
- Galactomannan assay - serum and/or BAL (sensitivity ~80% in neutropenic patients)
- Beta-D-glucan
- Bronchoscopy with BAL - culture + cytology
- Tissue biopsy - definitive (septate hyphae with acute-angle branching at ~45°)
- Antifungal susceptibility testing - critical because azole-resistant A. fumigatus isolates are emerging (environmental resistance via fungicide use)
Treatment
- Voriconazole - first-line (oral/IV); superior to amphotericin in landmark RCT (Herbrecht 2002)
- Isavuconazole - alternative first-line; fewer drug interactions; better tolerated
- Liposomal amphotericin B (LAMB) 3-5 mg/kg/day - for azole-refractory or intolerant cases
- Echinocandins - salvage therapy only (fungistatic against Aspergillus, not fungicidal)
- Combination (voriconazole + anidulafungin) - considered in high-risk patients (subgroup data favorable)
- Surgical resection - for lesions adjacent to great vessels or with massive hemoptysis
- Duration: minimum 6-12 weeks; continue until immunosuppression resolved
3. MUCORMYCOSIS
Overview
Mucormycosis (formerly "zygomycosis") is caused by aseptate or sparsely septate molds - principally Rhizopus, Mucor, and Lichtheimia species. It is one of the most rapidly fatal fungal infections known, with angioinvasion and tissue necrosis as hallmarks. During the COVID-19 pandemic, epidemic mucormycosis occurred in India among diabetic patients treated with corticosteroids.
Unique Risk Factors
- Diabetic ketoacidosis (DKA) - the most classic association
- Prolonged neutropenia / hematological malignancy
- Deferoxamine therapy (iron chelator provides iron to the fungus)
- Organ transplant
- Penetrating trauma / burns (cutaneous mucormycosis)
- Corticosteroid use (COVID-19 era)
Why DKA predisposes: High glucose and low pH impair neutrophil and macrophage function; elevated free iron (from acidosis) fuels fungal growth; iron-sequestration by deferoxamine paradoxically feeds the mold.
Clinical Forms
| Form | Affected Site | Key Features |
|---|---|---|
| Rhinocerebral | Sinuses → orbit → brain | Most common; starts with sinusitis, then proptosis, vision loss, and cerebral invasion; black necrotic eschar on palate/nasal turbinate |
| Pulmonary | Lungs | Similar to IPA; angioinvasion, infarction; rapidly fatal |
| Gastrointestinal | Stomach, colon | Malnourished patients; presents as bowel infarction |
| Cutaneous | Skin | Trauma, burns; locally destructive |
| Disseminated | Multiple organs | Near-universally fatal |
The "Black Eschar" Sign
The pathognomonic feature is a black necrotic lesion on the hard palate or nasal mucosa representing vascular thrombosis and tissue necrosis. Orbital involvement causes proptosis, periorbital edema, and vision loss - a surgical emergency.
Diagnosis
- CT/MRI of sinuses and brain - essential
- Tissue biopsy - definitive; shows broad, ribbon-like, aseptate hyphae with right-angle branching (contrasting with Aspergillus's acute-angle septate hyphae)
- Note: galactomannan and beta-D-glucan are negative in mucormycosis (major distinguishing feature from aspergillosis)
Treatment (triple approach - all three required simultaneously)
- Antifungal: Liposomal amphotericin B 5-10 mg/kg/day (higher doses than for aspergillosis); isavuconazole or posaconazole as step-down/salvage therapy
- Surgical debridement: Aggressive, often disfiguring. All necrotic tissue must be removed. May require orbital exenteration for orbital involvement
- Reverse the underlying predisposition: Correct DKA, reduce/stop immunosuppression
- Voriconazole has no activity against mucorales - a critical distinction when empirically treating uncertain mold infections
- Mortality: 40-80% (rhinocerebral form); >90% (disseminated form)
4. CRYPTOCOCCOSIS
Overview
Cryptococcosis is caused by Cryptococcus neoformans (global; from pigeon droppings, soil) and C. gattii (tropical, subtropical; Pacific Northwest USA/Canada outbreaks). It is one of the most common life-threatening fungal infections in HIV-infected patients and the 3rd most common IFI in solid organ transplant recipients.
Virulence Mechanisms (Medical Microbiology 9e)
Four key virulence factors:
-
Polysaccharide capsule - the most important:
- Physically blocks phagocytosis
- Suppresses both cellular and humoral immunity
- Inhibits antigen presentation to T cells
- Depletes complement components
- Reduces leukocyte migration
- Electrostatic repulsion prevents effector cell binding
-
Melanin synthesis (via membrane-bound phenoloxidase):
- Deposited in cell wall
- Increases cell wall integrity
- Protects against oxidative stress, temperature extremes, and microbicidal peptides
- Responsible for neurotropism - why the organism has a predilection for the CNS
-
Growth at 37°C - survives at body temperature
-
Alpha-mating phenotype (MATalpha) - regulates capsule and melanin gene expression
Pathogenesis
- Inhaled as small yeasts or spores
- In the lung: alveolar macrophages attempt phagocytosis but cannot reliably kill the organism
- Cryptococci replicate inside mature phagolysosomes ("Trojan horse" mechanism)
- CD4+ T cells are critical to prevent dissemination - which explains why HIV patients with CD4 <100/µL are at highest risk
- Dissemination: macrophages carrying viable yeast travel from lung → lymphatics → bloodstream → brain (facilitated by melanin-mediated neurotropism)
Clinical Manifestations
| Setting | Presentation |
|---|---|
| Immunocompetent | Often asymptomatic / mild pulmonary nodule found incidentally |
| Immunocompromised (HIV, transplant) | Severe pneumonia → rapid respiratory failure, ARDS |
| CNS (meningitis) | Subacute headache, fever, neck stiffness, altered consciousness; raised intracranial pressure |
| Skin | Papules, nodules, or umbilicated lesions resembling molluscum contagiosum (in AIDS) |
Cryptococcal meningitis is the most dangerous presentation:
- Often subacute (weeks of worsening headache)
- CSF: India ink prep shows encapsulated yeast; cryptococcal antigen (CrAg) titer - highly sensitive
- Raised intracranial pressure (ICP) is the leading cause of early death and neurological complications
- Management of raised ICP: serial lumbar punctures to remove CSF (target opening pressure <20 cmH₂O)
Treatment (HIV-associated cryptococcal meningitis)
Per WHO/IDSA guidelines:
- Induction (2 weeks): Liposomal amphotericin B + flucytosine (5-FC) - superior to amphotericin alone
- Consolidation (8 weeks): Fluconazole 400 mg/day
- Maintenance: Fluconazole 200 mg/day (until CD4 >200 for >6 months on ART)
- ICP management: serial therapeutic LPs; VP shunt in refractory cases
- Mortality: 20-40% even with optimal treatment in resource-rich settings; much higher in low-resource settings
5. HISTOPLASMOSIS (Disseminated)
Overview
Histoplasma capsulatum is a dimorphic fungus - mold in soil, yeast at 37°C in the body. Endemic to the Ohio and Mississippi River valleys (USA), Central America, and sub-Saharan Africa. Exposure through disruption of soil containing bird or bat droppings.
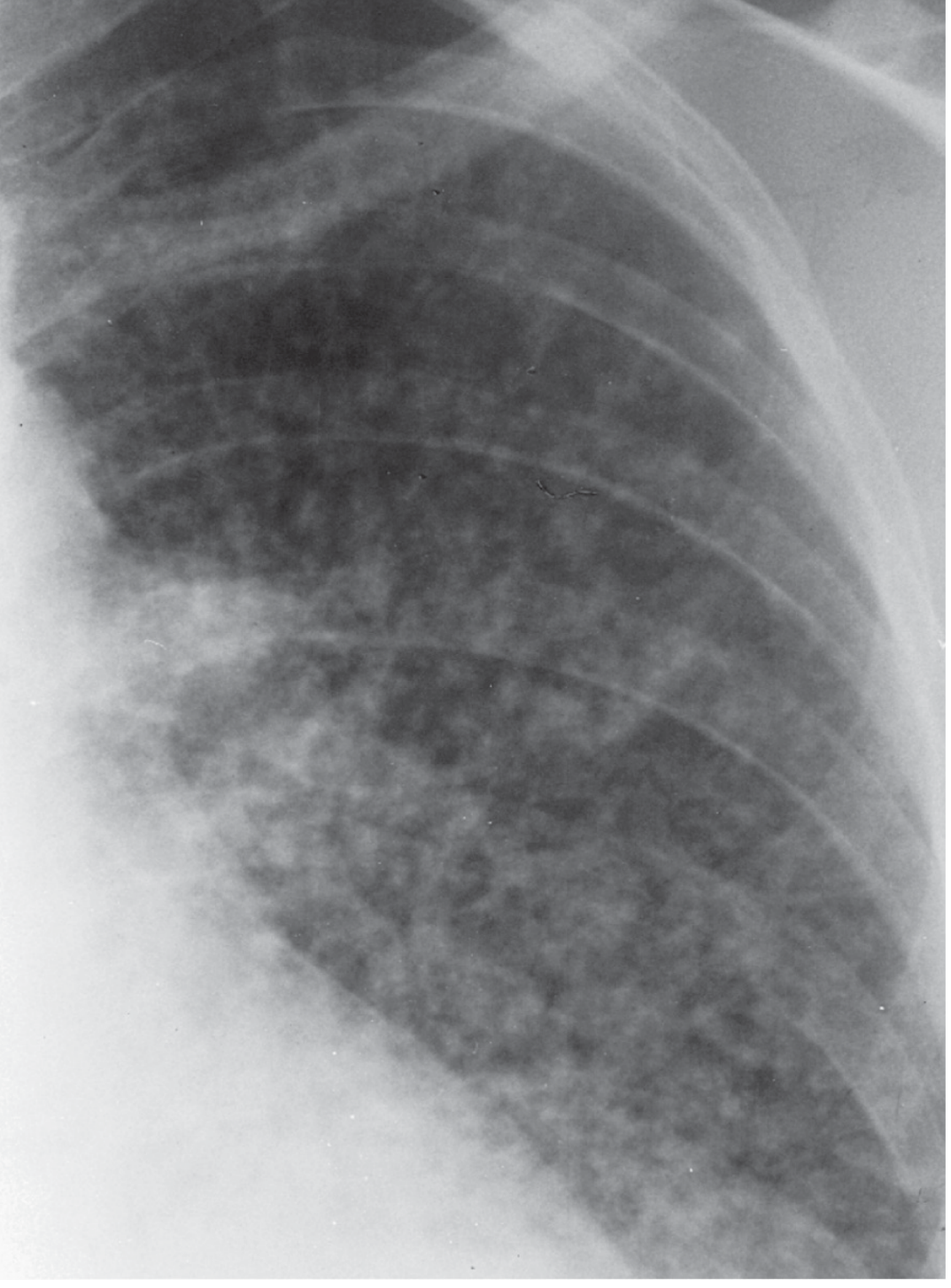
Clinical Features (HIV-associated disseminated histoplasmosis)
From Murray & Nadel's Textbook of Respiratory Medicine:
- 96% of AIDS patients present with fever and weight loss
- ~10% present with a sepsis-like syndrome: hypotension, respiratory failure, liver and renal failure, DIC
- Most cases occur with CD4+ count <100 cells/µL (often <50)
- Lab: anemia, leukopenia, thrombocytopenia; elevated LDH and serum ferritin (often markedly elevated)
- Chest X-ray: diffuse coarse reticulonodular opacities (or normal in 35-55% of disseminated cases)
Diagnosis
- Histoplasma urine antigen - detected in 100% of AIDS patients with disseminated disease (serum 92%)
- Rising antigen levels = relapse; falling = treatment response
- Cross-reacts with blastomycosis, coccidioidomycosis (false positives)
- Culture (weeks for growth)
Treatment
- Liposomal amphotericin B (induction for severe disseminated disease)
- Itraconazole (step-down and maintenance)
6. PNEUMOCYSTIS JIROVECII PNEUMONIA (PCP)
Previously classified as a protozoan, Pneumocystis jirovecii is now confirmed as a yeast-like fungus with unique biology. It causes one of the most common life-threatening AIDS-defining infections.
- Risk: CD4 <200 cells/µL (prophylaxis indicated)
- Presentation: Subacute progressive dyspnea, dry cough, fever; bilateral interstitial infiltrates; elevated LDH
- Diagnosis: Bronchoalveolar lavage (BAL) with Giemsa, methenamine silver stain; beta-D-glucan elevated
- Treatment: TMP-SMX (first-line); add prednisone if PaO₂ ≤70 mmHg (reduces mortality)
- Mortality: 5-15% (with treatment); up to 40-60% (without treatment)
Antifungal Drug Summary
| Drug Class | Mechanism | Key Indications | Major Toxicities |
|---|---|---|---|
| Polyenes (Amphotericin B, liposomal) | Binds ergosterol → pores in membrane → cell death | Broad spectrum; mucormycosis, cryptococcal meningitis, candidiasis | Nephrotoxicity, electrolyte loss (K⁺, Mg²⁺), infusion reactions |
| Azoles (fluconazole, voriconazole, itraconazole, posaconazole, isavuconazole) | Inhibit ergosterol synthesis (CYP51/14α-demethylase) | Candida (fluconazole), Aspergillus (voriconazole/isavuconazole), endemic fungi (itraconazole), mucormycosis prophylaxis (posaconazole) | QT prolongation, hepatotoxicity, CYP450 drug interactions, visual disturbances (voriconazole) |
| Echinocandins (caspofungin, micafungin, anidulafungin) | Inhibit β-1,3-D-glucan synthase → disrupts cell wall | First-line invasive candidiasis; salvage for aspergillosis | Generally well-tolerated; mild LFT elevation |
| Flucytosine (5-FC) | Inhibits DNA/RNA synthesis (converted to 5-FU intracellularly) | Combination with AmB for cryptococcal meningitis | Bone marrow suppression, GI toxicity; resistance develops rapidly if used alone |
Who Is Most at Risk?
The "deadly triad" of susceptibility:
- Neutropenia (especially prolonged, <500/µL) - key defense against molds (Aspergillus, Mucor)
- CD4 T-cell deficiency (HIV, transplant) - key defense against Cryptococcus, Histoplasma, PCP
- Loss of mucosal barriers (catheters, surgery, gut injury) - key risk for invasive Candida
Key Distinguishing Features at a Glance
| Organism | Hyphae | Galactomannan | Beta-D-glucan | Classical Host | Empiric Drug |
|---|---|---|---|---|---|
| Candida | Pseudohyphae | Neg | Pos | ICU, catheter, neutropenia | Echinocandin |
| Aspergillus | Septate, 45° branching | Pos | Pos | Neutropenia, HCT/SOT | Voriconazole |
| Mucor/Rhizopus | Aseptate, 90° branching | Neg | Neg | DKA, steroid use | Liposomal AmB |
| Cryptococcus | Encapsulated yeast | Neg | Neg | HIV CD4 <100 | AmB + 5-FC |
| Histoplasma | Dimorphic | Neg | Pos | AIDS, Ohio/Mississippi valley | Liposomal AmB → itraconazole |
| Pneumocystis | Yeast-like (unique) | Neg | Pos | HIV CD4 <200 | TMP-SMX |
Recent evidence note: A 2026 systematic review in JAMA Otolaryngol Head Neck Surg (PMID 41569597) confirmed mortality of acute invasive fungal rhinosinusitis (predominantly mucormycosis and aspergillosis) remains very high in immunocompromised populations, reinforcing the need for early diagnosis and aggressive surgical + antifungal management. Rezafungin (new echinocandin - once-weekly dosing) was non-inferior to caspofungin for invasive candidiasis per a 2025 systematic review (PMID 40651396), representing an emerging treatment option.
Sources:
- Murray & Nadel's Textbook of Respiratory Medicine (opportunistic mycoses, cryptococcosis, histoplasmosis)
- Medical Microbiology 9e (Cryptococcus neoformans virulence; Aspergillus pathogenesis)
- Current Surgical Therapy 14e (invasive candidiasis mortality data)
- Tietz Textbook of Laboratory Medicine 7e (candidemia bloodstream infection)
- Fitzpatrick's Dermatology (mucormycosis)
This is a shared conversation. Sign in to Orris to start your own chat.