Hey there i have viva and practicak examination of anatomy on tuesday what tips would u give to viva and osteology
Reading File
Finding Sources
Searching the Web
anatomy viva examination tips osteology bones landmarks medical student
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
Excellent! I have all the diagrams and content needed. Here is a thorough, well-organized answer:
Anatomy Viva & Osteology Practical - Complete Preparation Guide
(Source: Gray's Anatomy for Students)
PART 1: VIVA TIPS - How to Excel
Before the Exam
- Revise using the ABCN formula for every structure: Artery, Borders/relations, Clinical points, Nerve supply
- For each bone, know: name, type, side, identify by a unique feature, attachments, articulations, and clinical relevance
- Practice describing bones out loud - saying it aloud is very different from just reading
At the Viva Table
Bone identification - do this every time:
- Pick it up correctly - hold it confidently
- State the name - "This is the right femur"
- State how you identified it - give 2-3 distinctive features
- Side determination - explain your reasoning (e.g., "the head is medial, the greater trochanter is lateral")
- Orient it anatomically - hold it in the correct position
When asked about attachments:
- Go region by region (proximal to distal)
- Name the muscle + its action
- The examiner loves when you link the muscle action to the attachment site
Clinically impress the examiner:
- Always connect fractures to nerves at risk (e.g., surgical neck of humerus - axillary nerve)
- Mention "clinically important" features unprompted
Communication tips:
- If you don't know, say "I'm not sure of the exact detail, but I know that..." - never stay completely silent
- Use proper anatomical terms: "superior", "medial", "proximal" - not "up", "inside", "top"
- Think step by step out loud - examiners give credit for reasoning
PART 2: KEY BONES FOR OSTEOLOGY
HUMERUS (Upper Limb - Most Common Viva Bone)
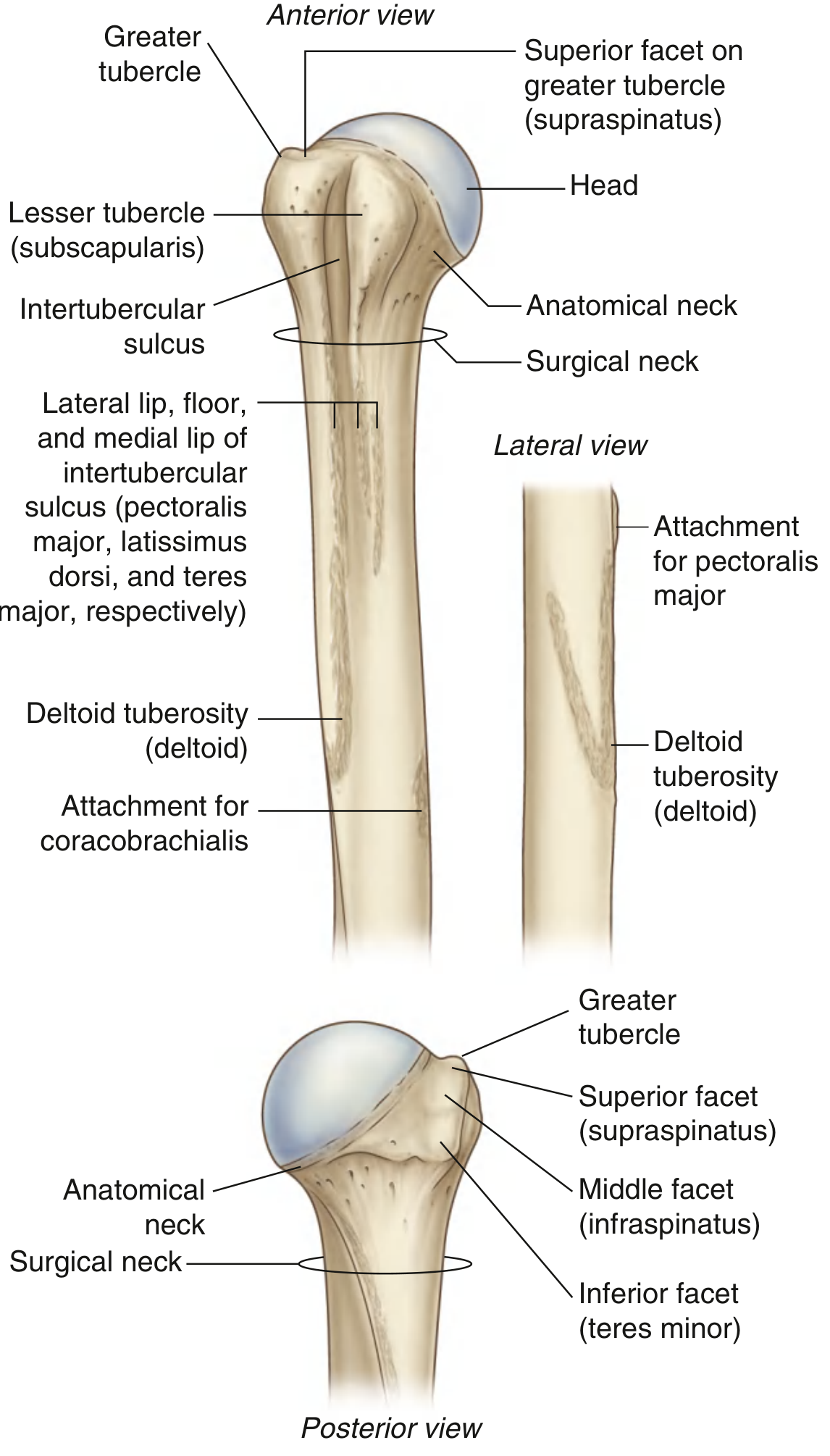
How to identify the side: Head points medially + greater tubercle is lateral
Rotator Cuff Attachments on Greater Tubercle (remember: SIT on the greater - Supraspinatus, Infraspinatus, Teres minor):
| Facet | Muscle |
|---|---|
| Superior facet | Supraspinatus |
| Middle facet | Infraspinatus |
| Inferior facet | Teres minor |
Lesser Tubercle: Subscapularis (the 4th rotator cuff muscle - the only one on the anterior/lesser side)
Intertubercular (Bicipital) Groove:
- Lateral lip - Pectoralis major
- Floor - Latissimus dorsi
- Medial lip - Teres major
- Tendon of long head of biceps passes through the groove
Shaft landmarks:
- Deltoid tuberosity (lateral, midshaft) - attachment for deltoid
- Coracobrachialis attaches on the medial surface at roughly the same level
Surgical neck - radial nerve runs in the spiral groove; axillary nerve and posterior circumflex humeral artery pass posteriorly to the surgical neck - fracture here can injure the axillary nerve (test deltoid and skin over lateral shoulder)
(Gray's Anatomy for Students, p. 822-823)
SCAPULA (Frequently Asked)
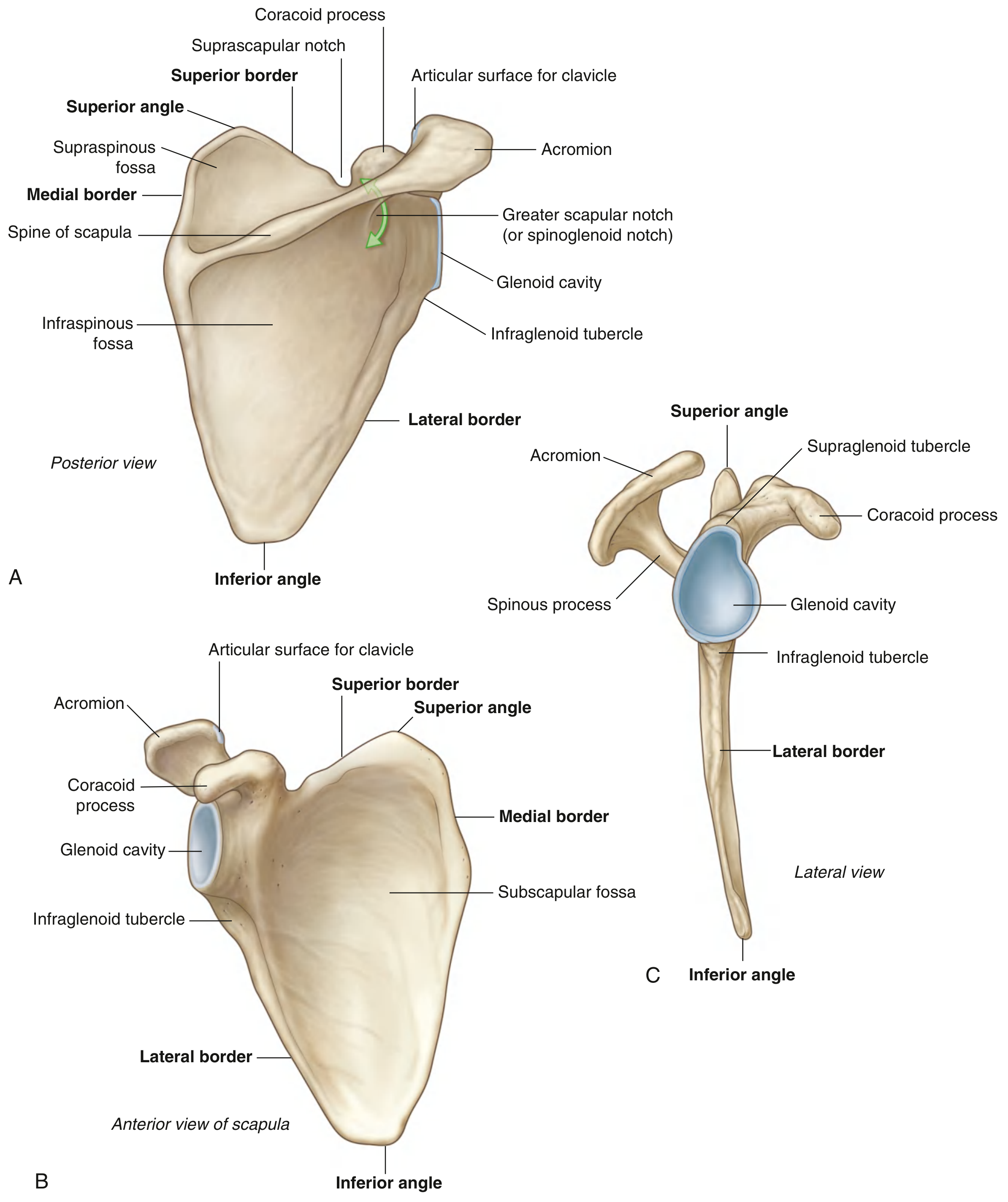
Key features to know:
- Spine divides posterior surface into supraspinous fossa (supraspinatus) and infraspinous fossa (infraspinatus)
- Acromion - articulates with clavicle; arches over glenohumeral joint
- Coracoid process - hook-like, projects anterolaterally; attachment for short head of biceps, coracobrachialis, pectoralis minor
- Suprascapular notch - suprascapular nerve passes through (but artery passes over - "lawyers pass under the bridge, soldiers pass over")
- Subscapular fossa (anterior/costal surface) - subscapularis muscle
- Glenoid cavity - articulates with head of humerus
- Supraglenoid tubercle - long head of biceps origin
- Infraglenoid tubercle - long head of triceps origin
- Lateral border is thick and strong (muscle attachment); medial border is thin and sharp
(Gray's Anatomy for Students, p. 821-822)
FEMUR (Lower Limb - Most Common Viva Bone)
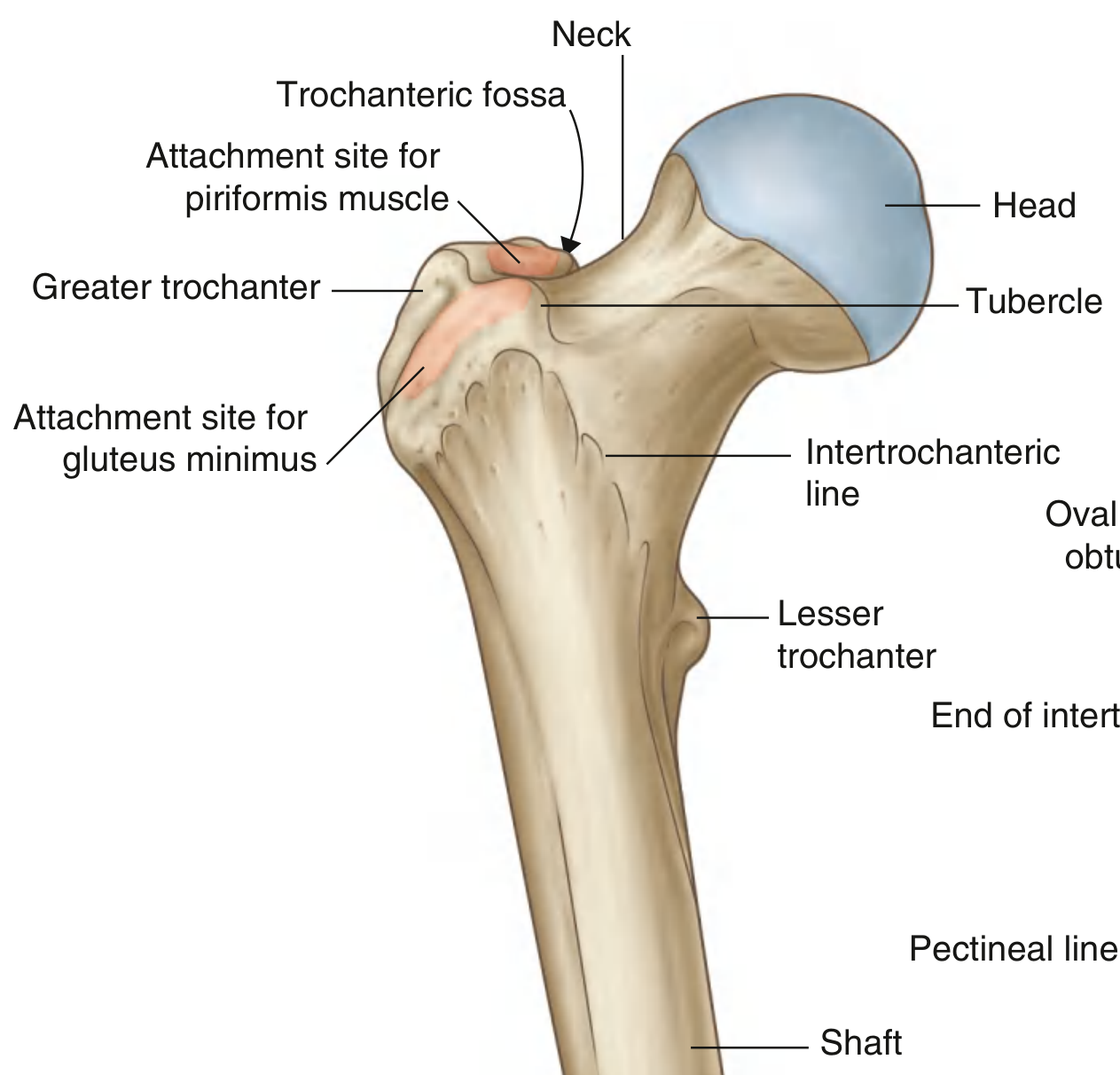
How to identify the side: Head is medial + greater trochanter is lateral; lesser trochanter is posteromedial (visible from behind)
Neck angle: ~125 degrees to the shaft (abnormal = coxa vara/valga)
Greater Trochanter attachments:
- Gluteus medius - posterolateral ridge
- Gluteus minimus - anterolateral ridge
- Obturator externus - oval depression in trochanteric fossa
- Obturator internus + gemelli - medial aspect, just above trochanteric fossa
- Piriformis - just above and behind obturator internus
Lesser Trochanter: Iliopsoas (psoas major + iliacus) - the prime hip flexor
Intertrochanteric line (anterior surface) - iliofemoral ligament (strongest ligament in the body) attaches here
Intertrochanteric crest (posterior surface) - quadratus femoris attaches to the quadrate tubercle on this crest
Clinical: Femoral neck fractures can disrupt blood supply to the femoral head (mainly from medial circumflex femoral artery) causing avascular necrosis - a classic viva question!
(Gray's Anatomy for Students, p. 657)
PART 3: HIGH-YIELD OSTEOLOGY VIVA Q&A
| Question | Key Answer |
|---|---|
| Which nerve is at risk in surgical neck of humerus fracture? | Axillary nerve |
| Which nerve is at risk in mid-shaft humerus fracture? | Radial nerve (in spiral groove) |
| What passes through the bicipital groove? | Tendon of long head of biceps |
| Which is the weakest part of the humerus? | Surgical neck |
| What attaches to lesser trochanter? | Iliopsoas (psoas major + iliacus) |
| What is the angle of femoral neck? | ~125 degrees |
| What passes through suprascapular notch? | Suprascapular nerve (not artery) |
| Which tubercle is for long head of biceps origin? | Supraglenoid tubercle |
| Which tubercle is for long head of triceps origin? | Infraglenoid tubercle |
| Blood supply to femoral head (main)? | Medial circumflex femoral artery |
PART 4: QUICK REVISION STRATEGY FOR TUESDAY
- Sunday (today): Upper limb bones - clavicle, scapula, humerus, radius, ulna
- Monday: Lower limb bones - hip bone (ilium, ischium, pubis), femur, tibia, fibula; revise nerve injuries
- Monday night: Do 1 full practice run - pick up each bone, state name, side, 3 features, and 3 muscle attachments out loud
The golden rule: Every examiner asks "What is the clinical importance?" after you identify a feature. Have a clinical point ready for every major landmark.
Good luck on Tuesday - you've got this!
This is a shared conversation. Sign in to Orris to start your own chat.