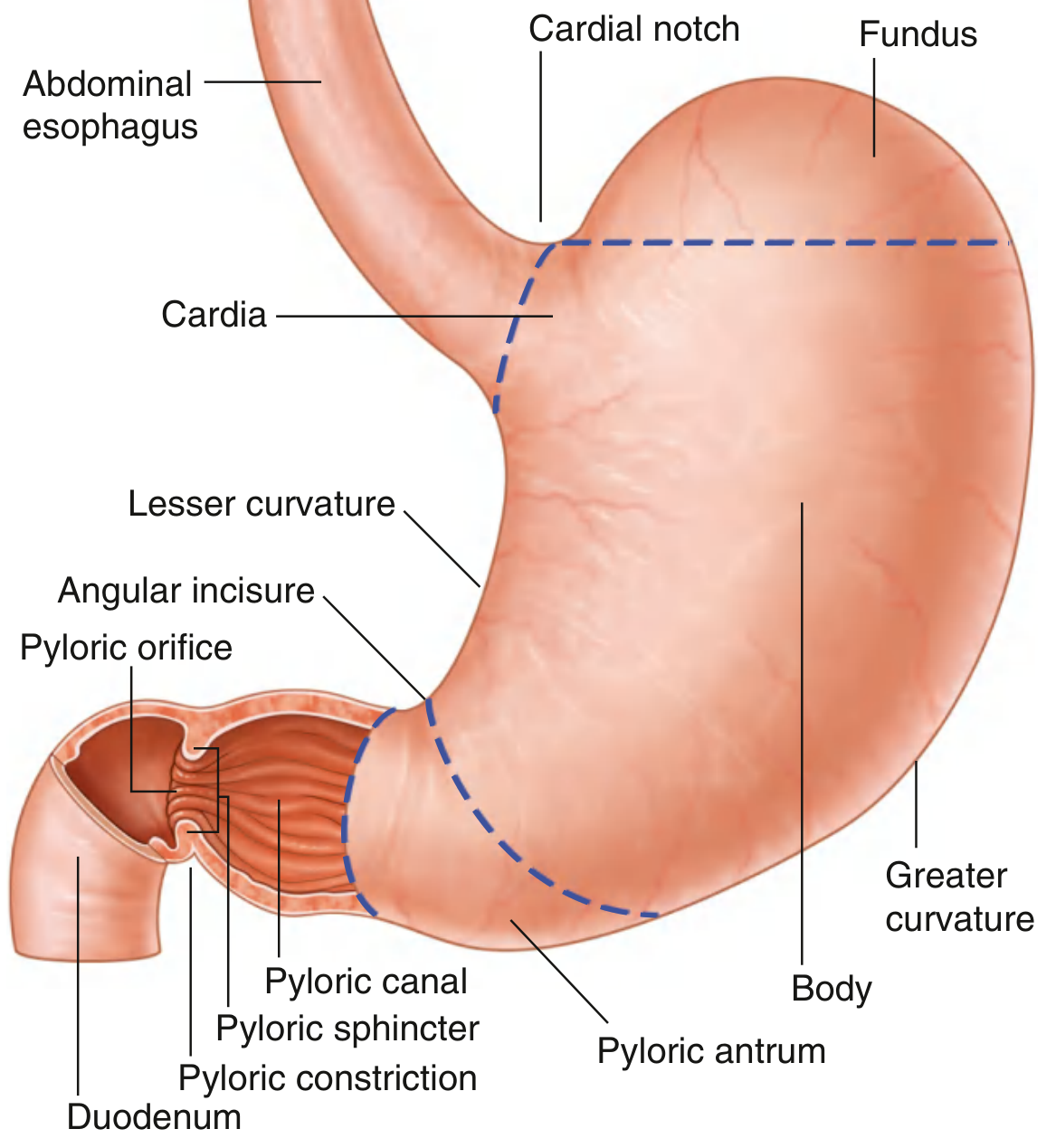
Stomach bed
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have comprehensive textbook content. The textbooks don't use the phrase "stomach bed" explicitly (it's a classic anatomy term), but all the posterior relations are well described. Let me compile the complete, detailed answer from the sources gathered.
Stomach Bed
The stomach bed is a classic anatomical term referring to the structures that form the posterior wall/floor of the lesser sac (omental bursa), against which the posterior surface of the stomach rests. When the stomach is lifted forward, these structures are exposed on the posterior abdominal wall.
Structures Forming the Stomach Bed
The stomach bed consists of the following structures (from above downward and from left to right):
| Structure | Region of Stomach Related To |
|---|---|
| Diaphragm | Fundus and upper posterior body |
| Left suprarenal (adrenal) gland | Upper posterior body |
| Upper part of left kidney | Posterior body |
| Splenic artery (along upper border of pancreas) | Posterior body |
| Body and tail of pancreas | Posterior body and antrum |
| Transverse mesocolon | Lower posterior body/antrum |
| Spleen (via gastrosplenic ligament) | Fundus and upper greater curvature |
The anterior surface of the pancreatic body is covered by the peritoneum of the lesser sac (omental bursa), which separates the stomach from the pancreas. This means the pancreas is the most direct and clinically important posterior relation.
- Sleisenger and Fordtran's GI and Liver Disease: "The anterior surface of the body [of pancreas] is covered by peritoneum of the omental bursa, which separates the stomach from the pancreas. The antrum and body of the stomach and the transverse mesocolon contact the body anteriorly."
Key Points
The lesser sac (omental bursa) lies between the posterior surface of the stomach and the stomach bed structures. The stomach bed is therefore the posterior wall of the lesser sac.
The diaphragm separates the fundus of the stomach from the heart above - "The fundus is separated from the heart only by the central tendon of the diaphragm." (Color Atlas of Human Anatomy, Vol 2)
The left kidney and adrenal form important posterior relations in the upper body region. The anterior surface of the left kidney contacts the stomach, spleen, jejunum, colon, and pancreas.
The pancreatic body and tail run obliquely across the posterior abdominal wall directly behind the stomach. In abdominal trauma, the body of the pancreas overlies the lumbar spine and is the most vulnerable part to injury when the stomach is full and compresses it against the spine.
The splenic artery runs a tortuous course along the upper border of the pancreas forming part of the posterior relation before entering the splenorenal ligament.
The transverse mesocolon attaches along the inferior aspect of the stomach bed, separating the supracolic from the infracolic compartments.
Clinical Relevance
-
Posterior gastric ulcer perforation: A posterior gastric ulcer can perforate into the lesser sac and erode into the structures of the stomach bed, most classically the splenic artery (causing massive hemorrhage) or the pancreas (causing pancreatitis/fistula).
-
Carcinoma of the stomach (posterior wall): Spread posteriorly can involve the pancreas, left kidney, adrenal, or splenic vessels - making surgical resection difficult or impossible.
-
Pancreatic pseudocyst: Can bulge anteriorly into the lesser sac between the stomach and the stomach bed, and is seen just posterior to the stomach on imaging. As noted in Schwartz's Principles of Surgery: "Once the gastrocolic omentum is divided, the body and tail of the pancreas can be seen along the floor of the lesser sac, just posterior to the stomach."
-
Splenic surgery and left kidney exposure: Surgeons approach the left kidney and adrenal gland through the stomach bed by entering the lesser sac.
Summary Mnemonic - "DSAKPT"
- D - Diaphragm (left crus and dome)
- S - Spleen (left end)
- A - Adrenal (left suprarenal gland)
- K - Kidney (upper left)
- P - Pancreas (body and tail)
- T - Transverse mesocolon (and splenic artery along pancreatic upper border)
Sources: Gray's Anatomy for Students; Color Atlas of Human Anatomy Vol. 2, Internal Organs; Sleisenger and Fordtran's GI and Liver Disease; Schwartz's Principles of Surgery, 11e
Prostate cancer (may cause meta stasis in brain) Meckles diverticulum Hemmoroids Varicocoel Umphalocoel(umbilical hernia) Faecal fistula Cremasteric reflex
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Here is a structured breakdown of all 7 topics:
1. Prostate Cancer - Brain Metastasis
Overview
Prostate cancer is one of the most common solid tumors and can metastasize widely. Its most frequent metastatic site is bone (especially the axial skeleton - vertebrae, pelvis, ribs, proximal femur), but brain metastasis does occur, particularly in advanced/castration-resistant disease.
Routes of Metastasis
Batson's Plexus (most important route):
The paravertebral venous plexus (Batson's plexus) is a valveless network of veins along the anterior epidural space that allows retrograde spread from the prostate to the vertebral column, sacrum, and skull base without passing through the pulmonary circulation. As noted in Harrison's Principles of Internal Medicine: "Metastases from prostate and ovarian cancer occur disproportionately in the sacral and lumbar vertebrae, probably from spread through Batson's plexus."
Hematogenous spread to brain:
- Brain is the most common intracranial site of metastases generally
- Prostate cancer has a particular predilection for the dura (dural metastases), and may be the only site of metastasis in otherwise well-treated patients
- Goldman-Cecil Medicine: "Dural metastases most commonly arise from breast or prostate cancer, frequently from a metastasis."
- Plum and Posner's Stupor and Coma: "Breast and prostate cancer and M4-type acute myelomonocytic leukemia have a particular predilection for the dura."
Key Clinical Points
| Feature | Detail |
|---|---|
| Commonest mets site | Bone (osteoblastic/sclerotic lesions) |
| Brain mets type | Dural > parenchymal |
| Spread route to spine/brain | Batson's paravertebral plexus |
| Marker | PSA (Prostate Specific Antigen) |
| Castration-resistant disease | Higher risk of brain/visceral spread |
2. Meckel's Diverticulum
Definition
A true diverticulum - remnant of the vitello-intestinal (omphalomesenteric) duct that normally disappears by week 7 of fetal life.
Rule of 2s (Classic Mnemonic)
- 2% of the population
- 2 inches (~5 cm) long
- 2 feet (~60 cm) from the ileocaecal valve
- 2 types of ectopic mucosa (gastric most common, pancreatic)
- 2 times more symptomatic in males
- 2 years - most present before age 2
Location: on the antimesenteric border of the ileum (unlike jejunal diverticula which arise from the mesenteric border).
Complications (from Bailey and Love's and S Das)
| Complication | Notes |
|---|---|
| Haemorrhage | Ectopic gastric mucosa causes peptic ulceration → painless dark rectal bleeding; diagnosed by Tc-99m scan |
| Diverticulitis | Mimics appendicitis; perforation resembles perforated DU |
| Intestinal obstruction | By fibrous band from apex to umbilicus; can cause volvulus |
| Intussusception | Diverticulum acts as lead point for ileoileal or ileocolic intussusception |
| Littre's Hernia | Meckel's diverticulum within a hernial sac (inguinal or femoral) |
| Perforation | Rare |
| Peptic ulcer | From heterotopic gastric mucosa |
Surgical Rule
- Wide-mouthed, non-thickened incidental Meckel's = can leave alone
- Symptomatic or narrow-necked = diverticulectomy or segmental ileal resection (for bleeding, as the ulcer is usually adjacent to the diverticulum, not inside it)
3. Haemorrhoids (Piles)
Definition
Symptomatic enlargements of the anal cushions - normal vascular structures in the submucosal layer of the anal canal that aid in fine continence.
Anatomy
- Internal haemorrhoids: above the dentate line; covered by mucosa; arise from the internal haemorrhoidal (superior rectal) plexus
- External haemorrhoids: below the dentate line; covered by squamous skin; arise from the inferior haemorrhoidal plexus
- Classic positions: 3, 7, and 11 o'clock (patient in lithotomy position) = right anterior, right posterior, left lateral
Pathophysiology
- Upright posture + no venous valves in the portal system + raised intra-abdominal pressure (straining, pregnancy) → venous congestion
- Shearing forces → mucosal trauma (bleeding) and caudal displacement (prolapse)
Degrees of Internal Haemorrhoids
| Degree | Feature |
|---|---|
| 1st | Bleed only; do not prolapse |
| 2nd | Prolapse on straining; reduce spontaneously |
| 3rd | Prolapse; need manual reduction |
| 4th | Permanently prolapsed; irreducible |
Symptoms
- Bright red, painless bleeding (on paper or splash in pan)
- Pruritus (from mucus discharge)
- Pain = suggests another diagnosis (fissure, thrombosed external haemorrhoid)
- Mucus discharge, prolapse
Treatment
- 1st/2nd degree: dietary advice, rubber band ligation, sclerotherapy
- 3rd/4th degree: haemorrhoidectomy (Milligan-Morgan)
4. Varicocele
Definition
Abnormal dilation and tortuosity of the pampiniform plexus of veins within the spermatic cord - essentially varicose veins of the testis.
Anatomy of the Pampiniform Plexus
The pampiniform plexus is a network of testicular veins that surround the testicular artery, allowing countercurrent heat exchange to keep the testis cooler than core body temperature (essential for spermatogenesis).
Epidemiology & Laterality
- 90% left-sided (due to the right-angle drainage of the left testicular vein into the left renal vein vs. the oblique drainage of the right testicular vein into the IVC)
- Also: angulation at the left testicular vein-renal vein junction, greater hydrostatic pressure on the left
- Isolated right-sided varicocele = red flag - must exclude retroperitoneal mass or renal tumour (right testicular vein drains at an acute angle to the IVC; right-sided obstruction suggests extrinsic compression)
Clinical Features
- Dragging discomfort in the scrotum, worse at end of day / when standing
- On examination (standing): "bag of worms" feel on palpation
- Varicocele decompresses when lying down (distinguishes from secondary obstruction)
- Long-standing cases: testicular atrophy and reduced sperm quality
Grading (Clinical)
- Grade I: palpable only on Valsalva
- Grade II: palpable without Valsalva
- Grade III: visible through scrotal skin
Secondary Varicocele
- Left renal cell carcinoma compressing the left renal vein → left testicular vein obstruction
- Does NOT decompress on lying down
Treatment
- Surgical ligation (inguinal/subinguinal/retroperitoneal approach)
- Radiological embolization via right femoral → IVC → left renal vein → left testicular vein
5. Omphalocele vs. Umbilical Hernia
Omphalocele (Exomphalos)
A congenital abdominal wall defect at the umbilicus due to failure of the intestines to return to the abdominal cavity during the 10th week of fetal life.
Key features:
- Covered by a sac of fused amnion + peritoneum (avascular)
- Umbilical cord inserts into the apex of the sac
- Abdominal wall musculature is intact around the defect
- Large omphaloceles contain liver and spleen outside the cavity
- Associated anomalies in ~50-75% of cases:
- Beckwith-Wiedemann syndrome (gigantism, macroglossia, umbilical defect, hypoglycemia)
- Chromosomal anomalies (trisomies 13, 15, 18, 21)
- OEIS complex (Omphalocele, Exstrophy, Imperforate anus, Spinal defects)
- Cardiac defects, pentalogy of Cantrell
Umbilical Hernia
A different condition from omphalocele. Occurs when intestines return to the abdomen during fetal life but then herniate again through an imperfectly closed umbilical ring after birth.
Key differences:
| Feature | Omphalocele | Umbilical Hernia |
|---|---|---|
| Sac covering | Amnion + peritoneum | Skin |
| Umbilical cord | Inserts into sac | Normal insertion |
| Abdominal wall | Defect present | Ring not fully closed |
| Timing | Congenital | Acquired (or congenital in neonates) |
| Associated anomalies | Common (50-75%) | Less common |
| Treatment | Surgical repair mandatory | Often closes spontaneously by age 2-5 |
Acquired umbilical hernia is common in adults associated with obesity, multiple pregnancies, ascites, and hepatic cirrhosis.
6. Faecal Fistula
Definition
An abnormal communication between the bowel lumen (large or small intestine) and the skin (enterocutaneous fistula) or another hollow organ, resulting in passage of faecal/intestinal content.
Types
- Faecal fistula from large bowel - may develop due to leakage from a suture line or anastomosis
- Umbilical faecal fistula - due to a patent vitello-intestinal (omphalomesenteric) duct (the same duct remnant as Meckel's diverticulum); presents as faecal discharge from the umbilicus
- Gastrocolic fistula - communication between stomach and colon; causes faeculent vomiting
- Enterovaginal / enterovesical fistula - bowel to vagina or bladder
Causes
- Post-operative anastomotic leak (most common in surgical practice)
- Crohn's disease
- Diverticular disease
- Radiation enteritis
- Malignancy
- Trauma
- Patent vitello-intestinal duct (congenital)
Management (Intestinal Fistula)
- Conservative: NBM + NG drainage + IV nutrition (TPN) + fluid/electrolyte replacement; may take weeks to seal
- Contrast studies to identify the fistula level and check for distal obstruction
- If conservative fails or there is distal obstruction: surgical resection of fistulated segment
- Small bowel fistulae are more serious (loss of digestive enzymes causes skin excoriation and significant fluid/electrolyte losses)
7. Cremasteric Reflex
Definition
A superficial reflex in males where stroking the inner thigh causes ipsilateral elevation of the testis due to contraction of the cremaster muscle.
Reflex Arc
| Component | Structure |
|---|---|
| Afferent | Femoral branch of genitofemoral nerve (sensory - inner thigh) |
| Spinal level | L1-L2 |
| Efferent | Genital branch of genitofemoral nerve (motor - cremaster muscle) |
| Response | Ipsilateral cremaster contraction → testis rises |
The cremaster muscle and cremasteric fascia form the middle (second) covering of the spermatic cord. (Gray's Anatomy for Students)
Clinical Significance
-
Testicular Torsion: Absence of the cremasteric reflex on the affected side is a key clinical sign. Campbell Walsh Urology: "The most common physical findings are generalized testicular tenderness, abnormal orientation of the testis, and absent cremasteric reflex." However, a present cremasteric reflex does NOT rule out torsion (sensitivity 73-96%).
-
Spinal cord assessment: Tests the integrity of the L1-L2 spinal segment. Absent in L2 lesions.
-
Age-related variation: More active in children; tends to diminish with age; may be absent in certain neurological disorders.
-
Genitofemoral nerve injury: e.g., during inguinal hernia repair - can abolish the cremasteric reflex on the ipsilateral side.
Sources: Bailey and Love's Short Practice of Surgery, 28e; Gray's Anatomy for Students; S Das - A Manual on Clinical Surgery, 13e; Campbell-Walsh-Wein Urology; Harrison's Principles of Internal Medicine, 22e; Goldman-Cecil Medicine; Sleisenger and Fordtran's GI and Liver Disease; Localization in Clinical Neurology, 8e; Developing Human - Clinically Oriented Embryology
This is a shared conversation. Sign in to Orris to start your own chat.