Cataract all details
Reading File
Finding Sources
Searching PubMed
cataract surgery outcomes complications
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
I now have extensive material to compile a comprehensive answer. Here is the full detailed coverage of cataracts:
Cataract - Complete Overview
Source: Kanski's Clinical Ophthalmology (10th ed.), Goldman-Cecil Medicine, Robbins Pathology
1. Definition
A cataract is any opacification of the crystalline lens. It is the commonest cause of reversible visual disability in the world. There is no medical treatment to prevent or arrest cataract; phacoemulsification with intraocular lens (IOL) implantation is the only effective management and is the most commonly performed surgical procedure worldwide.
2. Lens Anatomy (Foundation)
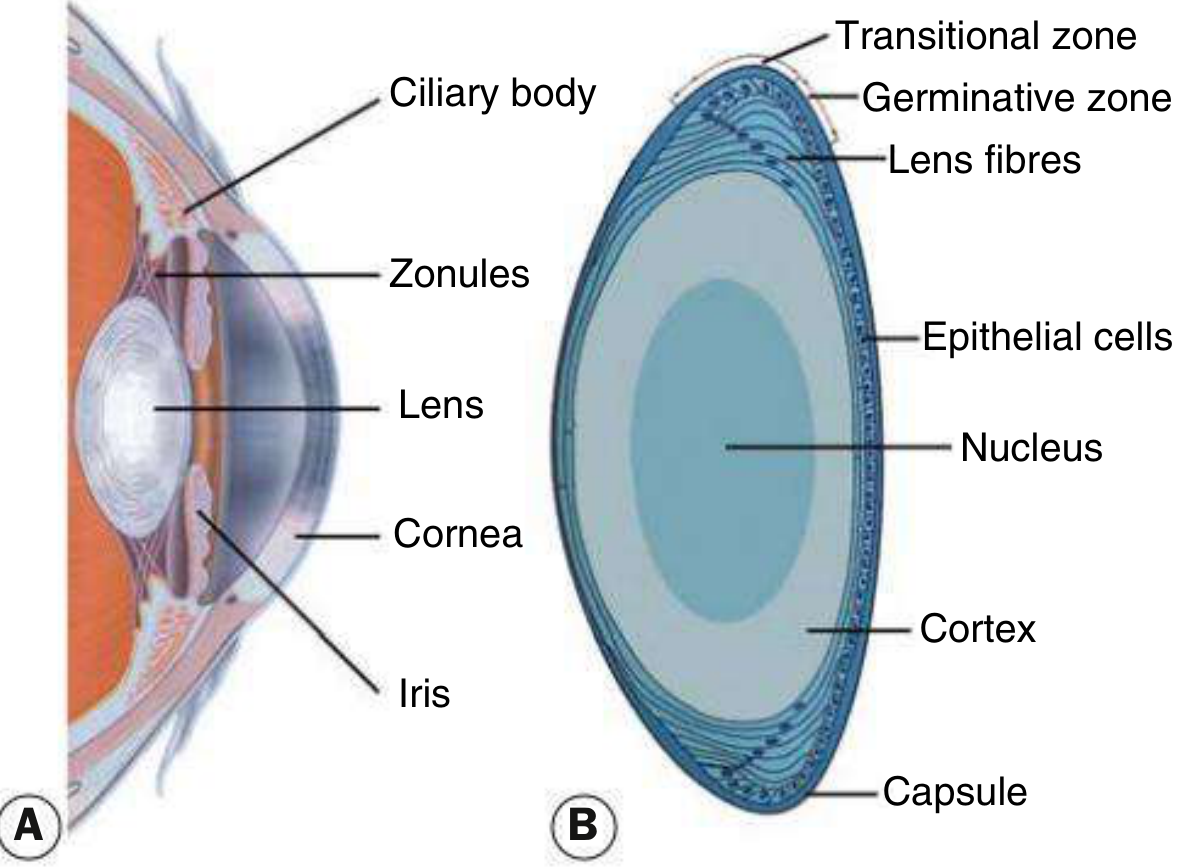
Fig. 10.1 - (A) Anterior segment cross-section; (B) Lens histology
| Structure | Detail |
|---|---|
| Capsule | Acellular membrane enclosing the lens |
| Epithelium | Cuboid cells under the anterior capsule; cells in the germinative zone divide continuously and differentiate into lens fibres |
| Cortex | Newly formed lens fibres - the outermost zone |
| Nucleus | Compressed older fibres at the centre - cannot be shed into the aqueous |
| Zonules | Suspend the lens from the ciliary body |
The lens doubles in volume between birth and age 70. Older fibres in the nucleus are compressed and gradually lose transparency. By age 45, loss of lens elasticity causes presbyopia (loss of accommodation for near objects). Further nuclear condensation eventually causes cataract.
3. Effects on Vision
Effects depend on:
- Type and location of the opacity
- Density of the opacity
- Pupil size - small pupils worsen posterior subcapsular (PSC) symptoms
Cataracts often develop slowly; early changes may be subtle. Common symptoms include:
- Progressive, painless blurring of vision
- Glare (especially PSC and cortical types)
- Monocular diplopia
- Colour desaturation
- Frequent changes in spectacle prescription
- "Second sight" - temporary improvement in near vision with nuclear cataracts (nuclear myopia)
4. Classification
A. Age-Related (Acquired) Cataracts
1. Posterior Subcapsular Cataract (PSC)
- Lies just in front of the posterior capsule
- Granular/plaque-like on oblique slit lamp; black and vacuolated on retroillumination
- Vacuoles are swollen migratory "Wedl" (bladder) cells
- Located at the nodal point of the eye - profound effect on vision even when small
- Symptoms: glare (especially from oncoming car headlights), worse in bright light (miosis) and near vision tasks
- Associations: steroids, radiation, diabetes, myotonic dystrophy
2. Nuclear Sclerotic Cataract
- Exaggeration of normal aging change
- Progressive yellowing due to deposition of urochrome pigment
- Advanced stages turn brown (brunescent), rarely black (cataracta nigra)
- Associated with myopia ("second sight of the aged") - increased refractive index of the nucleus
- Best assessed with oblique slit lamp beam; retroillumination shows good red reflex with subtle nucleus/cortex distinction
3. Cortical Cataract
- Starts as clefts and vacuoles between lens fibres due to cortical hydration
- Progresses to cuneiform (wedge-shaped) or spoke-like opacities often beginning inferonasally
- Glare is a common symptom
4. Christmas Tree Cataract
- Uncommon; polychromatic needle-like formations in the deep cortex and nucleus
- Associated with myotonic dystrophy
B. Cataract Maturity
| Stage | Features |
|---|---|
| Immature | Partially opaque; red reflex present |
| Mature | Completely opaque lens; no red reflex; white/grey appearance |
| Hypermature | Wrinkling of the anterior capsule (shrinkage) |
| Morgagnian | Total liquefaction of cortex; nucleus sinks inferiorly (visible through capsule) |

Fig. 10.3C - Hypermature cataract with wrinkling of the anterior capsule
5. Cataract in Systemic Disease
| Disease | Cataract Type |
|---|---|
| Diabetes mellitus | "Snowflake" cataract (bilateral, rapid-onset cortical or PSC in young; in older patients indistinguishable from age-related) |
| Myotonic dystrophy | PSC with distinctive stellate (star-shaped) spoke pattern |
| Atopic dermatitis | Bilateral, rapid-onset; shield-like dense anterior subcapsular plaque + PSC; occurs in 2nd-4th decades |
| Neurofibromatosis type 2 | PSC |
| Acute angle closure (glaucoma) | Glaukomflecken - focal grey-white subcapsular opacities at pupillary area; represent lens epithelial infarcts; pathognomonic of previous acute angle closure |
| High myopia | PSC + early nuclear sclerosis |
| Retinitis pigmentosa / hereditary retinal dystrophies | PSC (most common) |
6. Secondary (Drug-Induced) Cataracts
| Drug/Agent | Cataract Type |
|---|---|
| Corticosteroids (systemic and topical) | PSC - visually debilitating despite good acuity |
| Chlorpromazine (long-term) | Anterior star-shaped opacity |
| Amiodarone | Anterior capsular microdeposits |
| Busulfan, miotics | PSC |
7. Traumatic Cataract
Concussive (blunt) injury:
- "Rosette" cataract - feathery, stellate pattern beginning at the posterior pole of the lens
- Can resolve spontaneously if mild; progresses in more severe cases
Penetrating injury:
- Rapid opacification - white, fluffy appearance; if capsule is breached, aqueous rapidly penetrates and causes the lens to swell and opacify
Siderosis:
- Iron foreign body causes progressive brownish subcapsular deposits and eventually complete opacification
Radiation:
- PSC, particularly from X-ray and neutron radiation (infrared, microwave, and UV may contribute)
Electric shock:
- PSC; usually in the anterior subcapsular region
Chemical (alkali):
- Anterior subcapsular opacity; rapid if severe (alkali penetrates rapidly)
8. Congenital Cataract
Epidemiology
- ~3 per 10,000 live births
- Two-thirds are bilateral
- One-third associated with systemic disease; one-third inherited; one-third unknown
- Unilateral cataracts are usually sporadic
Aetiology
Inherited: Autosomal dominant is most common
Metabolic:
| Disorder | Feature |
|---|---|
| Galactosaemia (GALT enzyme deficiency - AR) | "Oil droplet" nuclear opacity in first days/weeks; dietary exclusion of galactose may reverse early changes |
| Lowe (oculo-cerebro-renal) syndrome (X-linked) | Universal cataract; microphakia; congenital glaucoma in ~50%; female carriers have minor cortical opacities |
| Mannosidosis (AR, α-mannosidase deficiency) | Spoke-like opacities in posterior cortex; corneal clouding |
| Hypo/pseudo-hypoparathyroidism | Various opacities |
Intrauterine infections (TORCH):
| Infection | Features |
|---|---|
| Rubella | Pearly nuclear or diffuse; unilateral or bilateral; occurs in ~15%; with other features of congenital rubella syndrome |
| Toxoplasmosis | Cataract + chorioretinitis + microphthalmos + optic atrophy |
| CMV | Jaundice, thrombocytopenia + cataract |
Chromosomal: Down syndrome (trisomy 21), Turner syndrome, Edwards syndrome, Patau syndrome
Other systemic: Lowe syndrome, Alport syndrome, Nance-Horan syndrome (X-linked, cataract + dental abnormalities), peroxisomal disorders
Management of Congenital Cataract
- Dense unilateral or bilateral central cataracts must be treated urgently to prevent amblyopia
- Surgery (lensectomy and anterior vitrectomy with or without primary IOL) followed by optical correction and patching of the better eye (amblyopia therapy)
- Visual prognosis for unilateral is much worse than bilateral unless detected and treated early
- Timing: surgery within first 6-8 weeks for dense unilateral cataracts
9. Management of Acquired Cataract
Indications for Surgery
Surgery is elective and indicated when:
- The cataract is the main cause of reduced visual acuity affecting daily activities (driving, reading, work)
- Refractive needs cannot be met by glasses or contact lenses
- Visually significant anisometropia
- Lens-induced complications (phacolytic glaucoma, phacomorphic glaucoma, lens-particle uveitis)
Preoperative Assessment
- Biometry: Measurement of axial length (A-scan ultrasound or optical coherence biometry) and keratometry to calculate correct IOL power
- Formulae: SRK/T, Haigis, Holladay 2, Barrett Universal II for IOL power calculation; newer AI-based formulas increasingly used
- Slit lamp examination: anterior segment, red reflex, iris, corneal integrity
- Posterior pole examination: exclude macular disease (AMD, diabetic maculopathy) that may limit postoperative visual gain
- Systemic assessment: diabetes control (affects healing), anticoagulant management, allergy to anaesthetic agents
- Refraction: document current spectacle prescription (important for "refractive surprise" detection)
Anaesthesia
| Type | Details |
|---|---|
| Topical | Proxymetacaine 0.5%, tetracaine 1%, lidocaine 2% gel; augmented with intracameral preservative-free lidocaine 0.2-1%; most common for routine phaco; no akinesia |
| Sub-Tenon block | Blunt cannula through conjunctival incision 5mm from limbus inferonasally; good anaesthesia, minimal complications; variable akinesia |
| Peribulbar block | 1-inch needle through skin or conjunctiva; effective anaesthesia + akinesia; rare but serious globe penetration risk - avoid in long eyes |
| Retrobulbar | Less used now; higher complication risk |
| General anaesthesia | Children, young adults, dementia, epilepsy, head tremor, very anxious patients |
Phacoemulsification (Standard Technique)
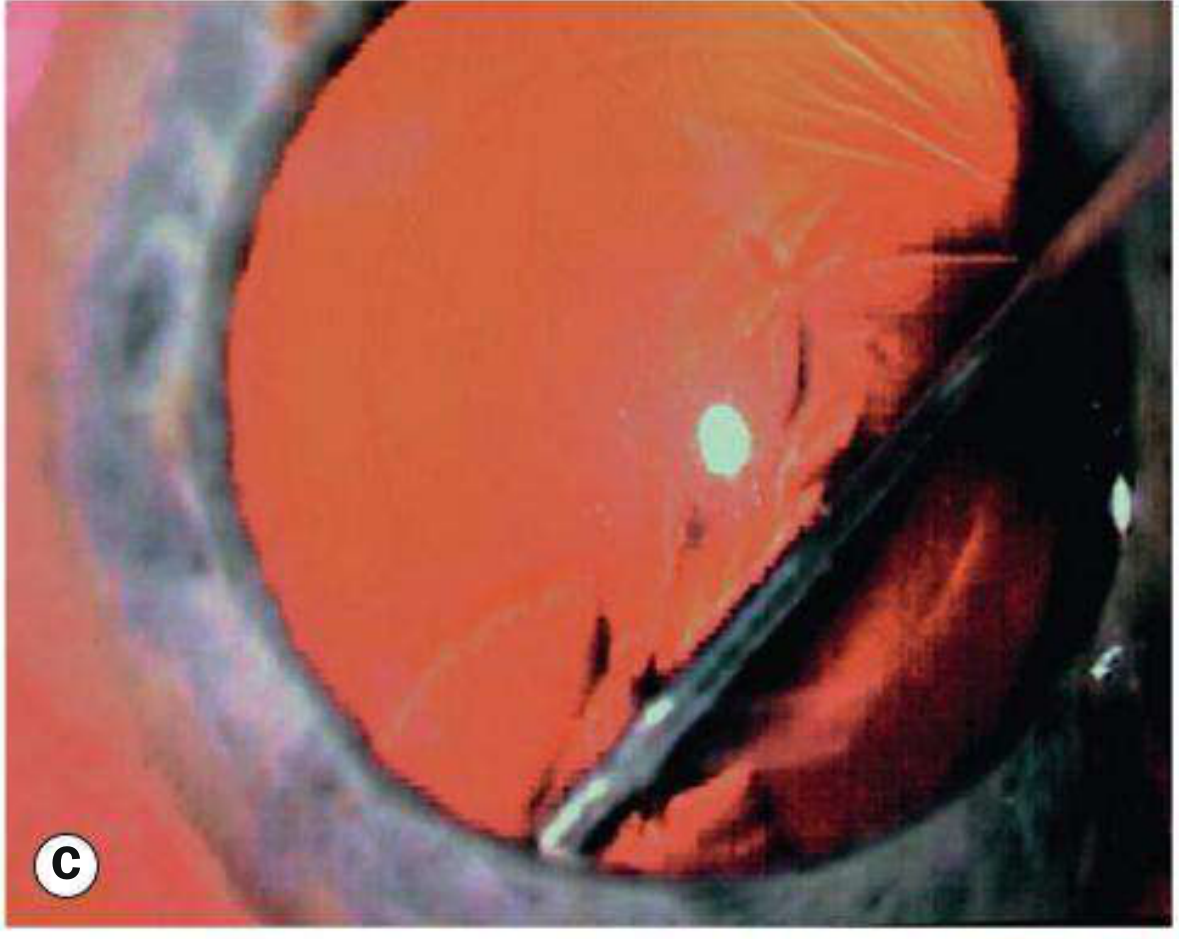
Fig. 10.14C - Hydrodissection
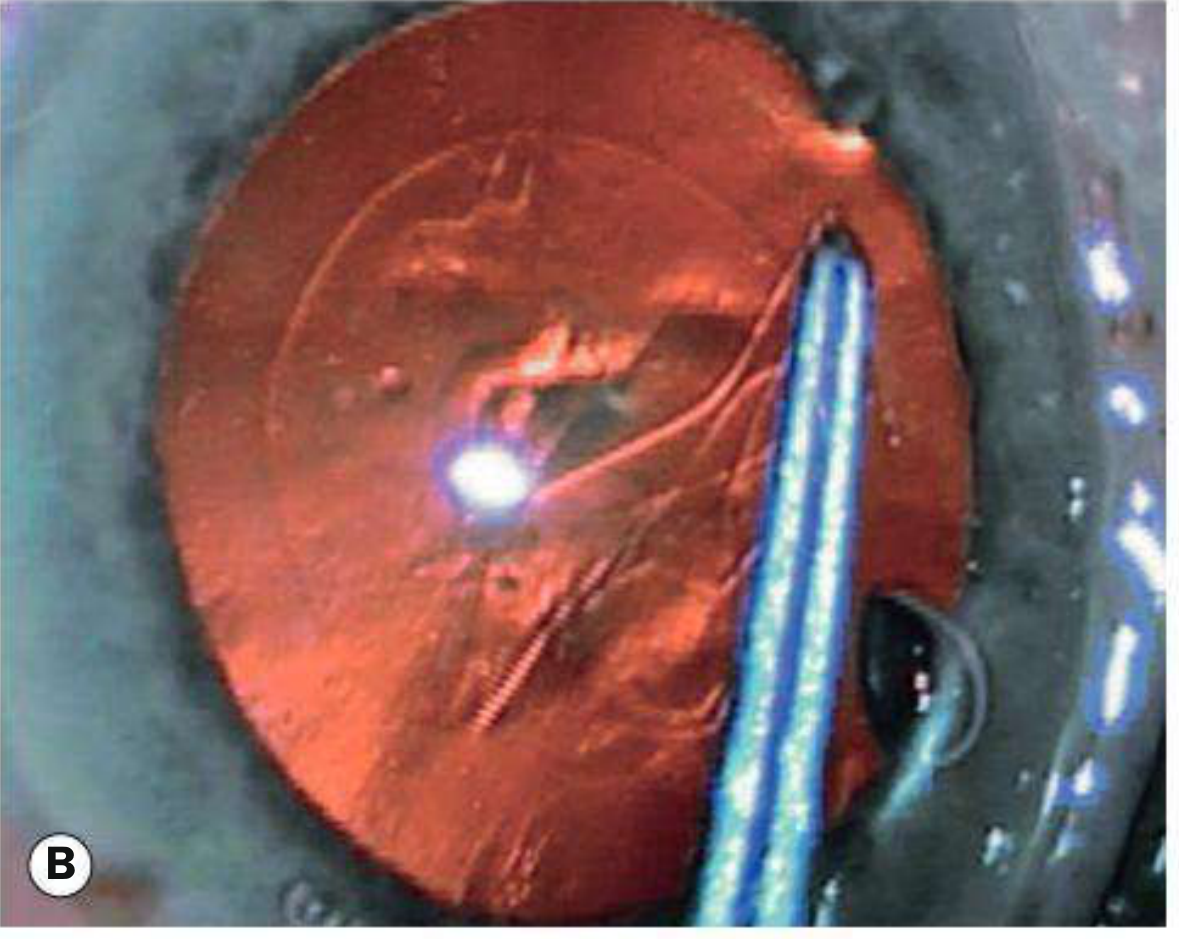
Fig. intraoperative - posterior capsule rupture with vitreous prolapse
Steps:
- Antisepsis: 5% povidone-iodine in conjunctival fornix (minimum 3 minutes), lid cleaning
- Draping - exclude lashes and lid margins
- Side port incision (60° left of main incision in right-handed surgeons)
- Viscoelastic injected into anterior chamber
- Main corneal incision (self-sealing; temporal location gives better access but slightly higher endophthalmitis risk)
- Continuous curvilinear capsulorhexis (CCC) - with cystotome or capsule forceps; 5-6mm diameter
- Hydrodissection - fluid injected beneath capsule edge to free nucleus from cortex
- Nucleus removal techniques:
- Divide and conquer: Two perpendicular grooves (sculpting) → crack into quadrants → emulsify each
- Phaco chop (horizontal/vertical): Less phaco energy, faster, requires more experience
- Stop and chop: Combination technique
- Cortical aspiration - automated coaxial or bimanual, or manual (Simcoe cannula)
- IOL insertion - capsular bag filled with cohesive viscoelastic; foldable IOL loaded in injector and deployed through main incision
- Wound hydration - to ensure self-seal; suture if needed
- Subconjunctival antibiotic + steroid injection, or topical antibiotic drops
Femtosecond laser-assisted cataract surgery (FLACS): Laser performs the incisions, capsulorhexis, and nuclear fragmentation; standard phacoemulsification provides results as good as FLACS overall.
10. Intraocular Lenses (IOLs)
| IOL Type | Details |
|---|---|
| Monofocal | Standard; corrects for one distance (usually distance); patient needs reading glasses |
| Toric IOL | Integral cylindrical component corrects pre-existing corneal astigmatism; risk of rotation in bag (may require surgical repositioning) |
| Bifocal/Multifocal | Refractive or diffractive optics to provide range of focal distances; increased spectacle independence but may have haloes/glare |
| Extended depth of focus (EDOF) | Elongated focal range with fewer dysphotopsias vs trifocal; recent meta-analyses compare favourably with trifocal for certain patients |
| Accommodative | Attempts to flex to alter focal length; in practice amplitude is slight |
| Adjustable (Light Adjustable Lens) | UV irradiation post-implantation alters polymer structure to fine-tune spherical and cylindrical power; performed ~1 week after surgery at slit lamp |
| Anterior chamber IOL (AC-IOL) | Used when insufficient capsular support; requires iridectomy (pupillary block); higher complication rate than PC-IOL |
11. Complications
Intraoperative
| Complication | Notes |
|---|---|
| Posterior capsule rupture (PCR) | Most important intraop complication; manifest as sudden AC deepening + pupil dilation; requires dispersive viscoelastic, possible conversion to ECCE, vitrectomy for prolapsed vitreous |
| Vitreous prolapse | Often accompanies PCR; must be cleared before IOL insertion |
| Posterior loss of lens fragments | Nucleus/cortex dislocated into vitreous; causes glaucoma, chronic uveitis, retinal detachment, CMO; managed by pars plana vitrectomy if fragments are large |
| Suprachoroidal haemorrhage (expulsive) | Rare, sudden; close wound immediately; drain if large haemorrhage at 7-14 days once liquefied |
| Zonular dehiscence | Risk in pseudoexfoliation, Marfan, trauma, mature cataracts |
Postoperative - Early
| Complication | Notes |
|---|---|
| Acute endophthalmitis | ~0.1% incidence; most commonly Staph. epidermidis (~90% Gram-positive); presents 2-7 days post-op with pain, decreased vision, hypopyon; diagnosed by aqueous/vitreous culture; treat with intravitreal antibiotics (vancomycin + ceftazidime) ± vitrectomy (Endophthalmitis Vitrectomy Study) |
| Corneal oedema | Due to endothelial damage; usually resolves; persistent cases → bullous keratopathy |
| Elevated IOP | From retained viscoelastic or inflammatory debris |
| Cystoid macular oedema (CMO) | "Irvine-Gass syndrome"; ~1-2%; peaks at 4-12 weeks; topical NSAIDs + steroids |
| Wound leak | Seidel test positive; Aqueous leaks from incision; re-suture if not self-sealing |
| Uveitis/Fibrin reaction | Toxic Anterior Segment Syndrome (TASS) - sterile inflammation from contaminated irrigating fluid or viscoelastic |
Postoperative - Late
| Complication | Notes |
|---|---|
| Posterior capsule opacification (PCO) | Most common late complication; occurs in up to 25-50%; "after-cataract"; due to residual lens epithelial cell proliferation (Wedl/bladder cells); treated by Nd:YAG laser capsulotomy |
| IOL dislocation | Late zonular weakness; more common in pseudoexfoliation syndrome |
| Retinal detachment | Increased risk post-phacoemulsification (especially in myopes, PCR cases) |
| Dry eye | Damage to conjunctival goblet cells and corneal nerves; common (systematic review 2025 confirms significant prevalence post-cataract surgery [PMID: 39806338]) |
| Diplopia | Muscle imbalance unmasked post-surgery; rare |
12. Posterior Capsule Opacification (PCO) - "After Cataract"
- Commonest late complication
- Lens epithelial cells remaining at the equator proliferate, migrate across the posterior capsule
- Produces visual blurring, glare, similar to original cataract symptoms
- Treatment: Nd:YAG laser posterior capsulotomy - creates a central opening in the opacified posterior capsule; quick, outpatient, effective
- Complications of YAG capsulotomy: raised IOP (transient), IOL damage (pitting), retinal detachment (slight increased risk), cystoid macular oedema
13. Special Situations
Phacomorphic Glaucoma
- Intumescent (swollen, hypermature) lens physically pushes iris anteriorly, closing the angle
- Presents as acute angle closure
- Emergency: IOP reduction + urgent cataract surgery
Phacolytic Glaucoma
- Hypermature cataract leaks lens proteins through intact (but permeable) capsule
- Macrophages laden with lens material block trabecular meshwork
- Presents as open-angle inflammatory glaucoma with milky aqueous
- Emergency: cataract surgery
Phacoanaphylaxis (Phacoantigenic Uveitis)
- Granulomatous inflammation triggered by lens protein acting as antigen
- Can occur after trauma or spontaneously in hypermature cataract
14. Cataract and Ectopia Lentis
Causes of subluxed/dislocated lens:
- Marfan syndrome (upward and temporal displacement - fibrillin-1 mutation)
- Homocystinuria (downward and nasal - treat with pyridoxine/methionine restriction)
- Weill-Marchesani syndrome (microspherophakia)
- Trauma
- Pseudoexfoliation syndrome (most common cause of acquired zonular weakness)
15. Prevention and Risk Factors for Age-Related Cataract
Risk factors include:
- Age (most important)
- UV-B radiation exposure
- Smoking
- Diabetes mellitus
- Corticosteroid use (systemic > topical)
- Nutritional deficiencies (antioxidants - vitamins C, E, carotenoids)
- Myopia
- Dehydration/diarrhoeal illness (especially in developing nations)
- Low socioeconomic status
No proven pharmacological agent prevents or reverses cataract formation. Ultraviolet-blocking sunglasses and smoking cessation are the most evidence-based preventive measures.
16. Epidemiology
- Leading cause of treatable blindness worldwide - responsible for ~51% of world blindness (WHO estimates)
- Cataract surgery is the most frequently performed surgical procedure in most countries
- Age-related cataract affects ~50% of people aged 65-74 and nearly 70% of those aged 75+
- In developing countries, "cataract blindness" remains prevalent due to limited surgical access
Key Clinical Points Summary
| Feature | Detail |
|---|---|
| Commonest cause of reversible blindness | Cataract (worldwide) |
| Commonest type in elderly | Nuclear sclerosis |
| Worst glare symptoms | PSC |
| Most profound effect on vision for size | PSC (at nodal point) |
| "Second sight" | Nuclear cataract (myopic shift) |
| Pathognomonic of past acute angle closure | Glaukomflecken |
| Galactosaemia cataract | Oil droplet opacity |
| Lowe syndrome | Universal cataract + microphakia + glaucoma |
| Congenital rubella | Pearly nuclear cataract |
| Steroid cataract | PSC |
| Chlorpromazine | Anterior star-shaped opacity |
| Most common intraoperative complication | Posterior capsule rupture |
| Most common late postoperative complication | PCO (after-cataract) |
| Treatment of PCO | Nd:YAG laser capsulotomy |
| Most common endophthalmitis pathogen | Staph. epidermidis |
Sources: Kanski's Clinical Ophthalmology, 10th ed., p. 308-343 | Goldman-Cecil Medicine, p. 4131 | Robbins Pathology
Recent evidence: A 2025 systematic review (PMID 39806338) confirms dry eye as a significant and common complication after cataract surgery. A 2024 Cochrane meta-analysis (PMID 38984608) comparing trifocal vs EDOF IOLs shows trifocals provide better near vision while EDOF lenses have fewer dysphotopsias - relevant when counselling patients on premium IOL choice.
This is a shared conversation. Sign in to Orris to start your own chat.