Biphasic t waves
Reading File
Finding Sources
Searching the Web
biphasic T waves ECG causes clinical significance
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Here is a thorough breakdown of biphasic T waves based on authoritative medical textbooks.
Biphasic T Waves
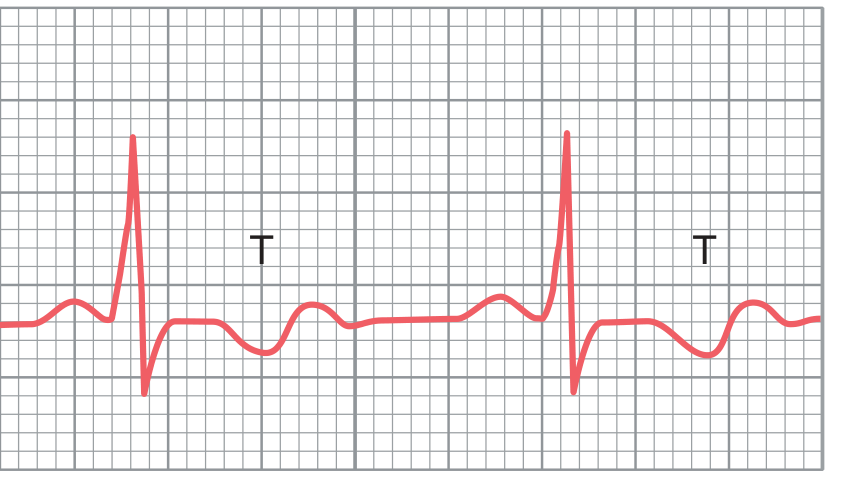
Definition
A biphasic T wave has two phases - it deflects in opposite directions within the same beat. There are two patterns:
- Positive-negative: starts upright then dips below the isoelectric line
- Negative-positive: starts with a downward deflection then rises above the isoelectric line
Physiology (Why Biphasic T Waves Form)
The T wave reflects ventricular repolarization. Normally, repolarization proceeds from epicardium to endocardium (apex to base), producing a single upright deflection.
When depolarization duration is unequal across different regions of the ventricular wall - some areas depolarizing shorter than others - the repolarization sequence becomes disorganized. This creates opposing vectors occurring at different times within the same T-wave window, producing the biphasic morphology.
As Guyton and Hall explains: "When the ischemia occurs in only one area of the heart, the depolarization period of this area decreases out of proportion to that in other portions. As a result, changes in the T-wave morphology, such as inversion or biphasic waveforms, can be evidence of myocardial ischemia."
Causes
1. Myocardial Ischemia
The most common cause. Focal ischemia shortens the action potential in that region via increased K+ channel conductance, causing that area to repolarize out of sync with the rest. This is most significant when new biphasic T waves appear in a symptomatic patient.
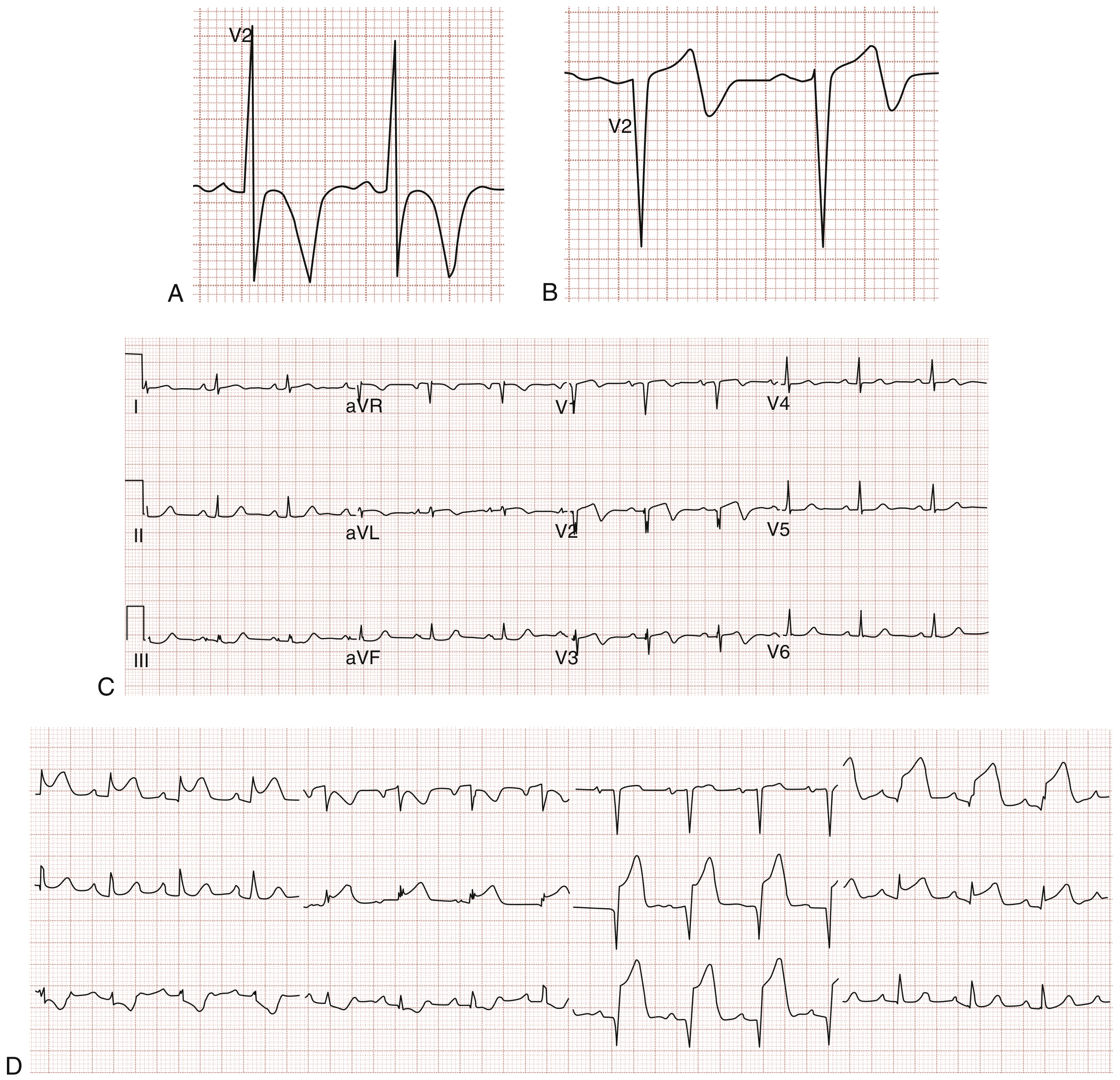
2. Wellens Syndrome (HIGH PRIORITY - Do Not Miss)
Wellens syndrome is a pattern of T-wave changes in the anterior precordial leads (V2-V3) that signals critical LAD stenosis. Two patterns exist:
| Pattern | T-Wave Morphology | Frequency |
|---|---|---|
| Type A (Type II) | Biphasic T waves (positive-negative) | ~25% of cases |
| Type B (Type I) | Deep symmetrical T-wave inversions | ~75% of cases |
Key diagnostic criteria for Wellens syndrome (from Tintinalli's):
- History of episodic chest pain consistent with unstable angina
- ECG taken when pain-free shows the T-wave changes
- Abnormal T waves most prominent in V2 and V3
- No pathologic Q waves or loss of R waves
- Normal or minimally elevated ST segments
- Normal or minimally elevated cardiac biomarkers
The natural history is progression to anterior wall STEMI if not recognized and treated. These patients require urgent angiography and should NOT be subjected to stress testing (risk of precipitating MI).
3. Hypokalemia
Severe hypokalemia (K+ < 2.5 mEq/L) classically produces:
- Depressed ST segment
- Biphasic T wave
- Prominent U wave
This is due to altered membrane repolarization kinetics from low extracellular potassium. (Harriet Lane Handbook)
4. Digitalis Effect / Toxicity
Digitalis overdose can cause unequal prolongation of depolarization in different ventricular regions, resulting in biphasic T waves. This is sometimes called the "digitalis effect" and may be accompanied by ST sagging and shortened QT. (Guyton & Hall, Goodman & Gilman)
5. Brugada Syndrome (Type 2 Pattern)
The Type 2 (saddleback) Brugada pattern features ST elevation of 2 mm followed by a trough, then continued ST elevation ≥1 mm with a positive or biphasic T wave in V1-V2. Note: only the Type 1 (coved) pattern is diagnostic of Brugada; Type 2 is suggestive but not specific. (Washington Manual)
6. Post-Reperfusion
After reperfusion of a STEMI, T-wave inversions may follow ST elevation in a biphasic or deeply inverted morphology, similar to Wellens syndrome changes. (Rosen's Emergency Medicine)
Summary Table
| Cause | Lead Distribution | Key Associated Features |
|---|---|---|
| Wellens syndrome (LAD stenosis) | V2-V3 (anterior precordial) | Chest pain history, pain-free when ECG taken, no Q waves |
| Myocardial ischemia | Variable | May accompany ST changes, symptoms |
| Hypokalemia | Diffuse | Prominent U waves, ST depression |
| Digitalis toxicity | Variable | ST sagging, short QT, dig level elevated |
| Brugada Type 2 | V1-V2 | Saddleback ST morphology, RBBB pattern |
| Post-reperfusion | Anterior leads | Follows STEMI treatment |
Clinical Pearl
When biphasic T waves are found in V2-V3 in a patient with a recent chest pain history who is now pain-free, always consider Wellens syndrome and treat it as a pre-infarction pattern. Avoid stress testing. Refer urgently for coronary angiography.
Sources: Guyton & Hall Medical Physiology | Tintinalli's Emergency Medicine | Rosen's Emergency Medicine | Harriet Lane Handbook | Washington Manual of Medical Therapeutics | Goodman & Gilman's Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.