Anatomy of interstitium of lung and clinical significance Full details for md exams 10 marks
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have excellent material from Murray & Nadel's Textbook of Respiratory Medicine and supporting anatomy texts. Let me compose the comprehensive MD exam answer.
Anatomy of the Interstitium of the Lung and Clinical Significance
I. INTRODUCTION
The interstitium of the lung is the connective tissue framework that gives the lung its structural integrity while remaining thin enough to permit efficient gas exchange. It is not a cavity but a three-dimensional scaffolding of fibrous proteins, proteoglycans, cells, and fluid that exists between the epithelial and endothelial cell layers throughout the lung.
II. GROSS AND SUBGROSS ORGANISATION - THE TWO COMPARTMENTS
As described by Hayek and detailed in Murray & Nadel's Textbook of Respiratory Medicine, the lung contains two well-defined interstitial connective tissue compartments arranged in series:
1. Parenchymal (Alveolar Wall) Interstitium
- Located within the walls of the alveoli (interalveolar septa)
- Forms the air-blood barrier
- Contains fused basement membranes of epithelium and endothelium
- Very thin on the "thin side" (~0.3-0.7 µm) and thicker on the "thick side"
2. Loose-Binding (Extra-Alveolar) Connective Tissue
- Comprises the peribronchovascular sheaths, interlobular septa, and the visceral pleura
- Serves as the structural envelope surrounding airways, vessels, and lobules
- Is a potential space that becomes visible only when pathologically expanded (edema, emphysema, lymphangitis)
The diagram below (Hayek's plan) shows these two compartments:

Figure: General plan of the interstitial connective tissue compartments. The alveolar walls form the parenchymal interstitium; all extra-alveolar support structures (airways, blood vessels, interlobular septa, visceral pleura) form the loose-binding compartment. (From Hayek, 1960)
III. MICROANATOMY OF THE ALVEOLAR WALL INTERSTITIUM
The alveolar wall (interalveolar septum) has an asymmetric structure with a thin side and a thick side:
Thin Side (Gas-exchange side)
- Type I pneumocyte (epithelium) → fused basement membranes of epithelium + endothelium → capillary endothelium → plasma → red blood cell
- Total thickness: ~0.3 µm
- This is the minimal-resistance pathway for O2 and CO2 diffusion
Thick Side (Support/structural side)
- Type I pneumocyte → basement membrane → interstitial space containing elastin (EL), collagen (COL), and proteoglycan matrix → capillary endothelium
- This side is widened to accommodate connective tissue elements
- Contains interstitial cells (fibroblasts, myofibroblasts) and occasional inflammatory cells
The electron micrograph below illustrates this asymmetry:
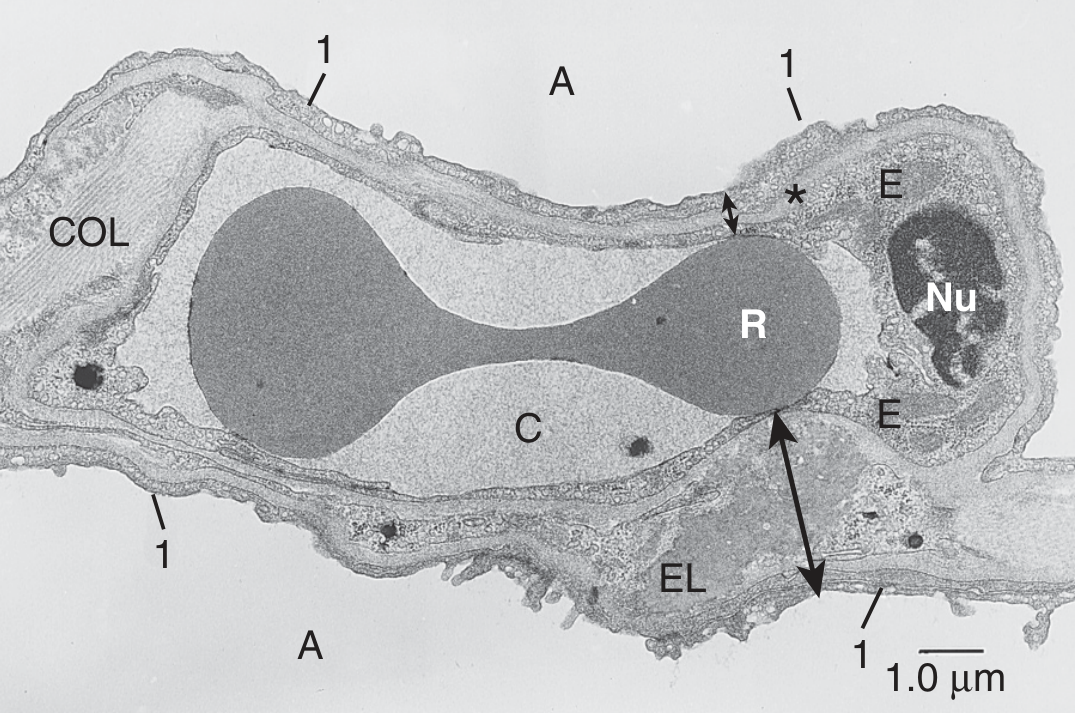
Figure: Cross-section of alveolar wall. Thin side () = type I epithelium (1) + fused basal laminae + capillary endothelium (E) + plasma (C) + RBC (R). Thick side (long arrow) = accumulation of elastin (EL) and collagen (COL). A = alveolus, Nu = nucleus of endothelial cell. (Human lung, TEM, Murray & Nadel)*
IV. CELLULAR COMPONENTS OF THE INTERSTITIUM
| Cell Type | Location | Function |
|---|---|---|
| Type I pneumocytes | >90% alveolar surface | Gas exchange; form thin side |
| Type II pneumocytes | 10% alveolar surface | Surfactant production (MUC5B); stem cells for Type I |
| Capillary endothelial cells | Alveolar capillaries | Gas exchange, fluid filtration |
| Fibroblasts (contractile + non-contractile) | Interstitial space | Collagen/elastin production, structural support |
| Myofibroblasts | Interstitial space | Wound repair, fibrosis in disease |
| Mast cells | Bronchial connective tissue, alveolar septa | Allergic/inflammatory responses |
| Plasma cells & occasional leukocytes | Interstitial space | Immune surveillance |
| Alveolar macrophages | Surface/within septa | Phagocytosis, innate immunity |
V. EXTRACELLULAR MATRIX (ECM) OF THE INTERSTITIUM
The bulk of the interstitium is occupied by a gel-like proteoglycan matrix containing:
- Collagens (type I, III, IV) - tensile strength; forms basket-like 3D structure around alveoli and airways
- Elastin - allows lung to expand and recoil; forms part of the "elastic continuum"
- Reticulin fibrils - fine network supporting alveolar walls
- Proteoglycans and glycosaminoglycans - versican, decorin, hyaluronan; form the gel matrix (~30 different core proteins); give the matrix its gel-like, low-compliance character
- Fibronectin - cell adhesion, wound repair
- Tenascin - expressed in inflammation and injury
- Laminin - basement membrane component
The connective tissue fibrils in the parenchymal interstitium are continuous extensions of the coarser fibers in the loose-binding tissue. Thus, mechanical stresses at the alveolar wall are transmitted to adjacent alveoli, bronchioles, and ultimately the visceral pleura - this has major clinical implications.
VI. LYMPHATICS OF THE INTERSTITIUM
- Lymphatic capillaries originate in the alveolar wall interstitium (parenchymal compartment) and drain toward the peribronchovascular sheaths
- They are arranged to drain primarily the alveolar wall interstitium
- Lymph flows centrally toward hilar lymph nodes
- Lymphatics also run along interlobular septa and the visceral pleura
Important functional point: Most interstitial water in pulmonary edema accumulates in the peribronchovascular loose connective tissue - and lymphatic capillaries cannot efficiently drain this compartment. This is why clearing interstitial edema depends on active sodium/water transport across the epithelium back into alveoli and then into the circulation.
VII. MECHANICAL/FUNCTIONAL ROLE
The basket-like arrangement of collagen, elastin, and reticulin fibrils allows the lung to:
- Expand in all directions during inspiration without excessive tissue recoil
- Maintain alveolar geometry and prevent alveolar collapse
- Transmit mechanical forces from the alveolar level to the pleura (interdependence)
- Provide alveolar interdependence - neighboring alveoli splint each other open
VIII. CLINICAL SIGNIFICANCE
1. Pulmonary Edema (Cardiogenic and Non-Cardiogenic)
- Fluid first accumulates in the loose peribronchovascular connective tissue (peribronchial cuffing on CXR/CT)
- Progresses to interlobular septa (Kerley B lines on CXR)
- Finally floods the alveoli (alveolar edema = air-space shadowing)
- Pathway: pulmonary capillary pressure ↑ → fluid enters alveolar wall interstitium → drains down pressure gradient into peribronchovascular loose tissue → can track to visceral pleura → pleural effusion
- Treatment targets: diuresis, PEEP to reduce hydrostatic forces, active sodium transport restoration
2. Interstitial Lung Disease (ILD)
- Any injury to the alveolar wall interstitium can trigger fibroblast activation and collagen deposition
- TGF-β1 plays a central role, activating myofibroblast transdifferentiation
- Results in interstitial fibrosis: thickened alveolar walls → ↑ diffusion distance → ↓ gas exchange → restrictive pattern on PFTs
- Key conditions: IPF (UIP pattern), NSIP, DIP, COP, hypersensitivity pneumonitis, sarcoidosis, drug-induced ILD
- CXR/HRCT: ground-glass opacification, honeycombing, traction bronchiectasis, septal thickening
- An increase in connective tissue in alveolar septa leads to pulmonary fibrosis with impaired diffusion (Color Atlas of Human Anatomy, Vol 2)
3. Idiopathic Pulmonary Fibrosis (IPF)
- Recurrent microinjuries to alveolar epithelium → abnormal wound healing
- ECM changes: ↑ collagen (COL1A1), ↑ elastin, ↑ versican, ↑ FN-EDA, ↑ tenascin-C, ↓ decorin (normally downregulates TGF-β1)
- ↑ LOXL2 (collagen cross-linking enzyme) → irreversible fibrosis
- Fibroblastic foci (myofibroblasts) are the histological hallmark
- PI3K-Akt signaling, focal adhesion pathways altered
- Treatment: nintedanib and pirfenidone slow progression by targeting fibroblast signaling
4. Interstitial Emphysema
- Air (from ruptured alveoli) enters the loose-binding connective tissue
- Dissects along peribronchovascular sheaths toward the hilum
- Tracks along lobular septa to the visceral pleura
- Can cause pneumomediastinum and pneumothorax
- Seen in: mechanical ventilation (barotrauma), birth asphyxia in neonates, whooping cough
5. Sarcoidosis
- Non-caseating granulomas form in the peribronchial, perivascular, and subpleural interstitium
- Follow lymphatic distribution (peribronchovascular distribution on HRCT)
- Hilar lymphadenopathy is prominent (lymphatics drain into hilar nodes)
6. Lymphangitic Carcinomatosis
- Metastatic tumor cells spread along lymphatics in interlobular septa and peribronchovascular sheaths
- CXR/CT: septal thickening, nodular thickening along fissures and bronchovascular bundles
- Clinical: severe dyspnea disproportionate to radiological extent
- Primary tumors: breast, lung, stomach, colon, pancreas
7. ARDS (Acute Respiratory Distress Syndrome)
- Diffuse alveolar damage injures both the alveolar epithelium and capillary endothelium
- Protein-rich fluid floods the interstitium and then the alveoli
- Fibroproliferative phase: fibroblasts proliferate in the interstitium → organizing fibrosis
- Pathological changes include: hyaline membrane formation, interstitial inflammation, and fibrosis
8. Pulmonary Hypertension
- Increased elastin and collagen deposition in the adventitia of pulmonary vessels (part of loose-binding interstitium)
- Vascular remodeling involves all three layers of the vessel wall
- ECM changes contribute to irreversible vascular remodeling
9. Pneumoconiosis (occupational)
- Inhaled particles (silica, coal dust, asbestos) reach the alveolar interstitium
- Activate macrophages → release fibrogenic cytokines → collagen deposition in interstitium
- Silicosis: nodular fibrosis in upper lobes
- Asbestosis: lower lobe interstitial fibrosis; asbestos bodies (ferruginous bodies) in interstitium
- Pleural plaques (from visceral pleural involvement via interstitial pathway)
10. Mast Cells and Bronchial Asthma
- Mast cells reside in the bronchial connective tissue and alveolar septa
- In allergic asthma, mast cell activation → histamine, leukotrienes → bronchoconstriction
- Chronic remodeling with sub-epithelial fibrosis of the lamina propria (part of airway interstitium)
IX. RADIOLOGY OF THE INTERSTITIUM
| Pattern | Pathological Correlate |
|---|---|
| Kerley B lines (horizontal, peripheral) | Thickened interlobular septa (fluid, tumor, lymphoma) |
| Kerley A lines (longer, hilum-directed) | Deep interstitial edema in peribronchovascular sheaths |
| Peribronchial cuffing | Peribronchovascular edema / inflammation |
| Ground glass opacification | Alveolar wall interstitial thickening (edema, inflammation, early fibrosis) |
| Honeycombing | Destroyed alveolar walls replaced by fibrous tissue (end-stage ILD) |
| Septal thickening (nodular) | Lymphangitic carcinomatosis, sarcoidosis |
| Traction bronchiectasis | Fibrotic distortion of peribronchovascular interstitium |
X. SUMMARY TABLE - ANATOMY vs. CLINICAL DISEASE
| Anatomical Compartment | Anatomical Structures | Clinical Disease |
|---|---|---|
| Parenchymal (alveolar wall) interstitium | Type I/II pneumocytes, fused BM, capillary endothelium, elastin, collagen | IPF, NSIP, ARDS, diffusion impairment |
| Peribronchovascular loose CT | Sheaths around bronchi and pulmonary arteries, lymphatics | Pulmonary edema (Kerley A), sarcoidosis, lymphangitic Ca |
| Interlobular septa | Connective tissue partitions between lobules | Kerley B lines, pulmonary edema, lymphangitic Ca |
| Visceral pleura | Continuation of interstitial connective tissue | Pleural plaques (asbestosis), pleural effusion, pneumothorax |
REFERENCES
- Murray & Nadel's Textbook of Respiratory Medicine, 7th Edition - Chapter 1: Gross and Subgross Organization; Chapter: Lung Fibrosis; Chapter: Pulmonary Edema
- Color Atlas of Human Anatomy, Vol 2 (Internal Organs) - Gas-exchanging Portion
- Hayek H. The Human Lung. New York: Hafner; 1960
Exam Tip: For a 10-mark question, structure your answer as: (1) Definition and compartments (2 marks), (2) Microanatomy of alveolar wall - thin/thick sides (2 marks), (3) Cellular and ECM components (2 marks), (4) Lymphatics and fluid dynamics (1 mark), (5) Clinical significance with at least 5 conditions and their pathological basis linking to anatomy (3 marks). Include at least one diagram of the thin/thick sides of the alveolar wall.
This is a shared conversation. Sign in to Orris to start your own chat.