Drugs use in peptic ulcer classify, pharmacological basis of uses, omeprazole moa, adverse effect Metoclopramide moa, therapeutic uses adverse effect Prokinetic agents define, example, therapeutic uses, adverse effect Lactulose moa, therapeutic uses adverse effect Laxative classify moa indication of any two classes, contraindications, therapeutic uses Detail answer 2nd yr mbbs pharmacology refer kd tripati
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from the textbooks. Let me compile the full detailed answer based on KD Tripathi-style 2nd year MBBS pharmacology, supplemented by Lippincott, Katzung, and Goodman & Gilman.
Gastrointestinal Pharmacology - 2nd Year MBBS Notes
(Based on KD Tripathi Essentials of Medical Pharmacology, Lippincott, Katzung)
PART 1: DRUGS USED IN PEPTIC ULCER DISEASE (PUD)
Classification
Peptic ulcer disease arises from two main causes: H. pylori infection and NSAID use. The pharmacological approach targets acid suppression, mucosal protection, and bacterial eradication.
A. Drugs Reducing Gastric Acid Secretion
-
Proton Pump Inhibitors (PPIs)
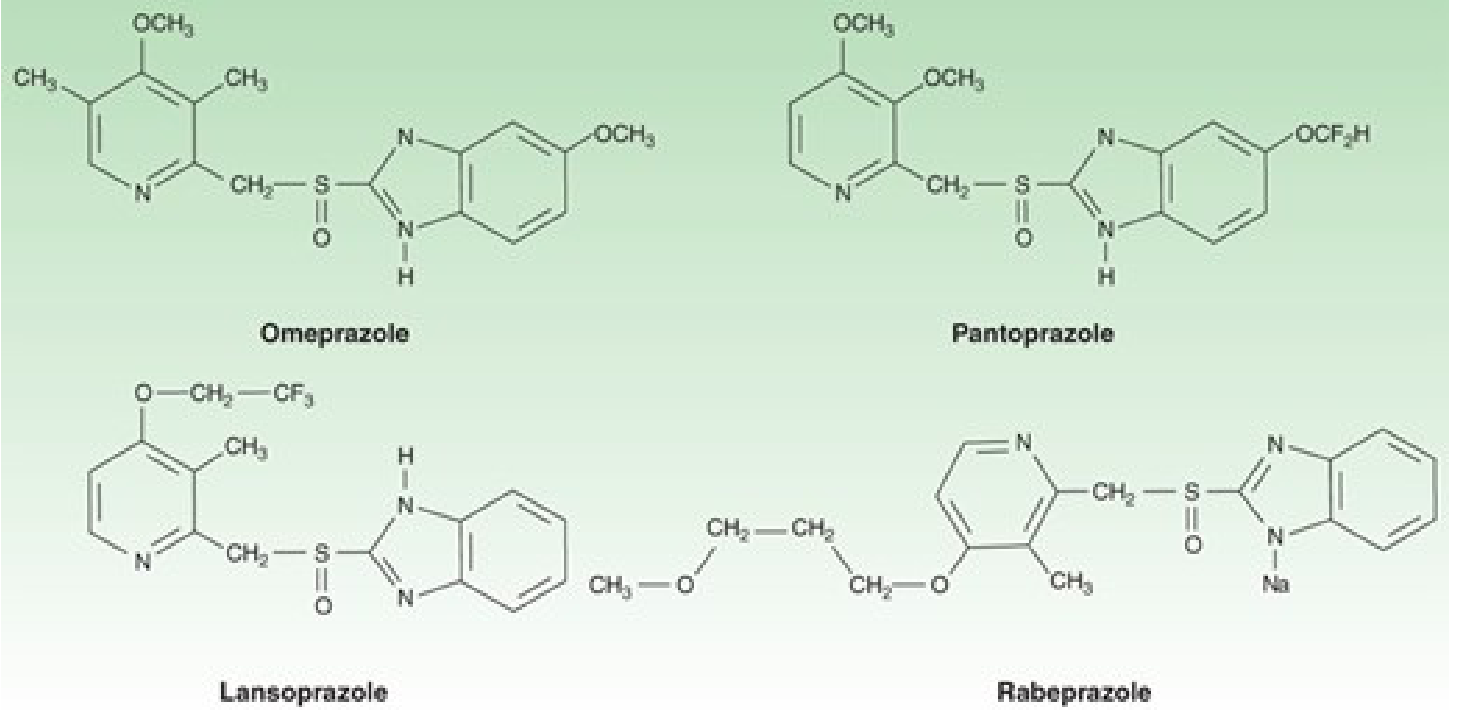
- Omeprazole, Esomeprazole, Lansoprazole, Pantoprazole, Rabeprazole, Dexlansoprazole
-
H2 Receptor Antagonists
- Cimetidine, Famotidine, Nizatidine (Note: Ranitidine withdrawn from market due to NDMA carcinogen contamination)
-
Anticholinergics (rarely used now)
- Pirenzepine (selective M1 blocker)
B. Antacids (Neutralize Acid)
- Aluminium hydroxide, Magnesium hydroxide, Calcium carbonate, Sodium bicarbonate
C. Mucosal Protective Agents (Cytoprotective)
- Sucralfate
- Bismuth subsalicylate
- Misoprostol (Prostaglandin E1 analogue)
- Carbenoxolone
D. Anti-H. pylori (Antimicrobials)
- Amoxicillin, Clarithromycin, Metronidazole, Tetracycline, Bismuth compounds
Pharmacological Basis of Drug Use in PUD
| Drug Class | Mechanism | Basis of Use |
|---|---|---|
| PPIs | Block H+/K+-ATPase irreversibly | Most potent acid suppressors; heal ulcers fastest |
| H2 blockers | Competitive block of histamine H2 receptors on parietal cells | Reduce ~70% of acid; good for nocturnal acid |
| Antacids | Chemical neutralization of HCl | Rapid symptom relief; no healing effect |
| Sucralfate | Polymerizes in acid, forms protective coat on ulcer base | Physical barrier; also stimulates mucus/prostaglandin |
| Misoprostol | PGE1 analogue - inhibits acid, enhances mucus/HCO3 | NSAID-induced ulcer prevention |
| Bismuth | Coats ulcer, kills H. pylori, stimulates mucus | Component of H. pylori regimens |
| Antibiotics | Eradicate H. pylori | Curative treatment; reduces recurrence from 60-100%/yr to <15% |
Acid secretion from parietal cells is stimulated by three pathways: acetylcholine (via vagus), histamine (via H2 receptors), and gastrin. All converge on activation of the H+/K+-ATPase proton pump to secrete H+ ions. PPIs block the final common pathway, making them the most effective class.
(Lippincott Pharmacology, p. 1419)
PART 2: OMEPRAZOLE - DETAIL
Mechanism of Action
Omeprazole is a substituted benzimidazole prodrug. Its MOA is:
- Administered as an inactive prodrug (enteric coated to protect from gastric acid)
- Absorbed in the alkaline small intestine and transported to the parietal cell via blood
- Being a lipophilic weak base (pKa ~4), it diffuses across lipid membranes and accumulates in the acidic secretory canaliculus of the parietal cell
- In the acidic environment, it undergoes protonation and rapid molecular conversion to an active sulfenamide cation
- This active form forms a covalent disulfide bond with cysteine residues on the H+/K+-ATPase (proton pump), causing irreversible inactivation
The result: Omeprazole blocks H+ secretion regardless of the stimulus (histamine, gastrin, or ACh), making it superior to H2 blockers.
Key pharmacokinetic points:
- Must be taken 30-60 minutes before meals (only active pumps are inhibited; fed state activates more pumps)
- Short plasma half-life (~0.5-1 hr) but acid inhibition lasts up to 24 hours (irreversible pump inactivation)
- New pumps take ~18 hours to synthesize
- Full effect takes 3-4 days of daily dosing (not all pumps blocked with first dose)
- Metabolized by CYP2C19 (genetic polymorphism affects response) (Katzung Basic & Clinical Pharmacology, 16th Ed.)
Therapeutic Uses of PPIs (Omeprazole)
- Peptic ulcer disease (duodenal and gastric ulcers)
- Gastroesophageal reflux disease (GERD) - first line
- Zollinger-Ellison syndrome (massive acid hypersecretion)
- H. pylori eradication - always used as the acid suppressor component of triple/quadruple therapy
- NSAID-induced ulcer - treatment and prevention
- Stress ulcer prophylaxis in ICU patients
Adverse Effects of Omeprazole
| System | Effect |
|---|---|
| GI | Nausea, diarrhea, abdominal pain, constipation, flatulence |
| CNS | Headache, dizziness, drowsiness |
| Endocrine | Hypomagnesemia (with long-term use) |
| Bone | Osteoporosis/fractures (reduced calcium absorption; long-term use) |
| Infections | Increased risk of C. difficile, pneumonia, enteric infections (due to loss of acid barrier) |
| Renal | Acute interstitial nephritis (rare) |
| Haematological | Vitamin B12 deficiency (impaired absorption with long-term use) |
| Rebound | Acid hypersecretion on sudden withdrawal |
| Drug interactions | Reduces absorption of ketoconazole, itraconazole, iron salts; may increase levels of warfarin, diazepam (CYP2C19 competition) |
PART 3: METOCLOPRAMIDE
Mechanism of Action
Metoclopramide's MOA is complex and multi-receptor:
- Dopamine D2 receptor antagonist (primary mechanism): Dopamine normally inhibits cholinergic smooth muscle stimulation in the GI tract. By blocking D2 receptors, metoclopramide releases this inhibition, restoring coordinated peristalsis
- 5-HT4 receptor agonist: Enhances ACh release from myenteric plexus neurons, increasing peristaltic amplitude
- 5-HT3 receptor antagonist (vagal and central): Contributes to antiemetic effect
- Sensitizes muscarinic receptors on smooth muscle (possible additional prokinetic mechanism)
- Blocks D2 receptors in the chemoreceptor trigger zone (CTZ)/area postrema - produces powerful antiemetic effect
Net result: Increases esophageal peristaltic amplitude, increases lower esophageal sphincter (LES) pressure, and enhances gastric emptying. No effect on small intestine or colonic motility.
(Goodman & Gilman, Katzung 16th Ed.)
Therapeutic Uses
- Gastroparesis (diabetic, post-surgical) - first-line prokinetic
- GERD - increases LES pressure; used with antisecretory agents in refractory cases
- Prevention and treatment of nausea and vomiting (postoperative, drug-induced, migraine-associated)
- Chemotherapy-induced emesis (high-dose IV)
- Nonulcer dyspepsia - symptomatic relief
- Facilitate nasoenteric tube advancement in hospitalized patients
- Migraine - parenteral use for acute relief
Adverse Effects
| Category | Effect |
|---|---|
| CNS (most common) | Restlessness, drowsiness, insomnia, anxiety, agitation (10-20% patients, especially elderly) |
| Extrapyramidal (EPS) | Acute dystonia, akathisia, Parkinsonism (25% at high doses, 5% long-term) - due to central D2 blockade |
| Tardive dyskinesia | Sometimes irreversible; with long-term use - FDA Black Box Warning |
| Endocrine | Hyperprolactinaemia - galactorrhoea, amenorrhoea, gynaecomastia (D2 block → prolactin release) |
| Cardiac | QT prolongation at high IV doses |
| GI | Diarrhea |
Contraindications: Parkinson's disease, GI obstruction/perforation, pheochromocytoma (may cause hypertensive crisis)
PART 4: PROKINETIC AGENTS
Definition
Prokinetic agents are drugs that enhance coordinated gastrointestinal motility by increasing the frequency and force of propulsive contractions, without producing abnormal (non-propulsive) contractions. They accelerate gastric emptying and intestinal transit.
Classification and Examples
| Class | Mechanism | Drugs |
|---|---|---|
| D2 antagonists | Block dopaminergic inhibition of GI motility | Metoclopramide, Domperidone |
| 5-HT4 agonists | Stimulate ACh release via myenteric neurons | Cisapride (withdrawn), Mosapride, Tegaserod |
| Motilin receptor agonists | Stimulate motilin receptors | Erythromycin (macrolide antibiotic) |
| Cholinomimetics | Muscarinic M3 stimulation | Bethanechol, Neostigmine |
| Ghrelin receptor agonists | Stimulate gastric motility | Relamorelin (investigational) |
Therapeutic Uses of Prokinetics
- Gastroparesis (diabetic, idiopathic, post-surgical) - primary indication
- GERD - increase LES tone; used adjunctively with PPIs
- Functional dyspepsia / nonulcer dyspepsia
- Nausea and vomiting (metoclopramide as antiemetic)
- Intestinal pseudo-obstruction (Ogilvie syndrome - neostigmine IV)
- Facilitate enteral tube feeding
- Pre-anesthesia (metoclopramide to reduce aspiration risk)
Adverse Effects (General Class)
- Metoclopramide/Domperidone: EPS reactions, tardive dyskinesia, hyperprolactinaemia (domperidone is safer - does not cross BBB as readily)
- Cisapride: Withdrawn due to fatal cardiac arrhythmias (QT prolongation - Torsades de pointes) from hERG channel block
- Erythromycin: Nausea, abdominal cramping, diarrhea, antibiotic resistance, drug interactions (CYP3A4)
- Bethanechol: Cholinergic effects (excessive salivation, bronchospasm, bradycardia, GI cramping)
PART 5: LACTULOSE
Mechanism of Action
Lactulose is a synthetic disaccharide (galactose + fructose). Its MOA:
- Not hydrolyzed by GI enzymes - reaches the colon intact
- Colonic bacteria degrade lactulose into lactic acid, formic acid, and acetic acid (short-chain organic acids)
- This lowers the intraluminal pH and increases osmotic pressure, drawing water into the colon
- Results in: fluid accumulation, colon distension, soft stools, and defecation
For hepatic encephalopathy (additional mechanism):
- Acidification of colonic contents converts NH3 (ammonia, which is absorbed) into NH4+ (ammonium ion, which is non-absorbable and trapped in the colon)
- This reduces colonic ammonia production and absorption
- Colonic bacteria that produce ammonia are also suppressed by the acidic environment
- The cathartic effect shortens gut transit time, further limiting ammonia absorption (Lippincott Pharmacology, p. 1440)
Therapeutic Uses
- Constipation - osmotic laxative
- Hepatic encephalopathy - primary treatment to lower blood ammonia
- Portal-systemic encephalopathy - chronic use to prevent recurrence
- Sometimes used in hyperammonaemia of other causes
Adverse Effects
- Flatulence, bloating, and cramping (from bacterial fermentation and gas production) - most common; may reduce compliance
- Diarrhea (if dose is too high)
- Nausea and vomiting
- Electrolyte disturbances - hypokalemia, hyponatremia with excessive use
- Abdominal distension
- Long-term use: possible lactic acidosis (rare)
- Caution in diabetics - contains small amounts of lactose and galactose (generally safe but monitor)
PART 6: LAXATIVES - CLASSIFICATION, MOA, AND INDICATIONS
Classification
1. Bulk-Forming Laxatives
- Psyllium (Isabgol), Methylcellulose, Bran
2. Osmotic Laxatives
- Lactulose, Polyethylene glycol (PEG), Magnesium hydroxide (Milk of Magnesia), Magnesium citrate, Magnesium sulfate (Epsom salt), Sodium sulfate
3. Stimulant (Irritant) Laxatives
- Senna (sennosides), Bisacodyl, Castor oil, Cascara sagrada, Dantron
4. Stool Softeners (Emollient/Surfactant Laxatives)
- Docusate sodium, Docusate calcium
5. Lubricant Laxatives
- Mineral oil, Glycerin (as suppository)
6. Chloride Channel Activators (newer)
- Lubiprostone
7. Guanylate Cyclase Agonists (newer)
- Linaclotide, Plecanatide
MOA and Indications: Two Selected Classes
CLASS 1: STIMULANT (IRRITANT) LAXATIVES
Examples: Senna, Bisacodyl, Castor oil
MOA:
- Senna: Contains anthraquinone glycosides (sennosides). After oral ingestion, colonic bacteria hydrolyze sennosides to active anthrones. These act directly on nerve fibers in the colonic mucosa, stimulating the myenteric plexus and increasing peristalsis. Also increase electrolyte and water secretion into the bowel.
- Bisacodyl: Acts directly on nerve fibers in the mucosa of the colon, stimulating mass peristaltic movement. Available as suppositories (act within 15-60 min) and enteric-coated tablets (act in 6-10 hrs).
- Castor oil: Hydrolyzed in small intestine to ricinoleic acid, which is irritating to the GI mucosa, stimulating increased peristalsis. Onset 2-6 hours. Avoided now due to poor palatability and risk of intense cramping.
Onset: 6-12 hours (oral senna/bisacodyl); 15-60 minutes (bisacodyl suppository)
Indications:
- Acute constipation requiring rapid relief
- Pre-procedural bowel preparation (colonoscopy, surgery)
- Opioid-induced constipation - senna + docusate combination is standard
- Bedridden patients needing regular bowel management
- Post-hemorrhoidectomy/anorectal surgery (suppository form)
CLASS 2: BULK-FORMING LAXATIVES
Examples: Psyllium (Isabgol), Methylcellulose, Bran, Sterculia
MOA:
- These are hydrophilic colloids derived from indigestible plant material (cellulose, hemicellulose, gums)
- They absorb water in the large intestine, swell, and form a viscous gel
- This increases stool bulk and softness, distending the bowel
- Intestinal distension stimulates the defecation reflex and peristaltic activity
- Transit time is reduced
- They mimic the natural physiological effect of dietary fibre
Onset: 12-72 hours (slowest acting laxatives); must be taken with adequate water
Indications:
- Chronic constipation - safest for long-term use; drug of first choice
- Irritable bowel syndrome (IBS-C)
- Hemorrhoids and anorectal disorders (softens stool, reduces straining)
- Diverticular disease - reduce intraluminal pressure
- Post-bariatric surgery constipation
- Hypercholesterolemia - psyllium reduces LDL cholesterol (additional benefit)
- Diabetes mellitus - psyllium reduces postprandial blood glucose
Contraindications of Laxatives (General)
| Contraindication | Reason |
|---|---|
| Bowel obstruction | May worsen obstruction; risk of perforation |
| Undiagnosed abdominal pain | May mask appendicitis or other acute abdomen |
| GI perforation or ileus | Risk of peritonitis |
| Inflammatory bowel disease (acute flare) | May worsen inflammation |
| Megacolon / toxic megacolon | Risk of perforation |
| Nausea/vomiting with unknown cause | Possible bowel obstruction |
| Pregnancy (stimulant/osmotic laxatives) | May stimulate uterine contractions (castor oil - avoided; senna - cautious) |
| Immobile patients (bulk laxatives) | Risk of intestinal obstruction if inadequate water intake |
| Children < 6 months (mineral oil) | Aspiration risk causing lipoid pneumonia |
| Fecal impaction (bulk laxatives) | May worsen impaction |
| Renal failure (magnesium salts) | Risk of hypermagnesaemia |
| Heart failure / edema (sodium-containing antacids) | Sodium load worsens fluid retention |
Therapeutic Uses of Laxatives (Summary)
| Class | Primary Use |
|---|---|
| Bulk laxatives | Chronic constipation, IBS-C, diverticular disease - safest long-term |
| Osmotic (PEG, lactulose) | Chronic constipation, hepatic encephalopathy (lactulose), bowel prep (PEG) |
| Stimulant (senna, bisacodyl) | Acute constipation, opioid-induced constipation, pre-procedure |
| Stool softeners (docusate) | Post-operative, post-MI, anorectal disorders - prevents straining |
| Lubricant (mineral oil) | Short-term, elderly patients with hard stools - not long-term |
| Lactulose specifically | Hepatic encephalopathy, chronic constipation in elderly |
Quick Reference Summary Table
| Drug | Class | MOA | Key Adverse Effect |
|---|---|---|---|
| Omeprazole | PPI | Irreversible H+/K+-ATPase blockade | Hypomagnesaemia, C. diff, B12 deficiency |
| Cimetidine | H2 blocker | Competitive H2 receptor antagonism | Anti-androgenic, CYP450 inhibitor |
| Sucralfate | Cytoprotective | Acid-activated polymer; coats ulcer | Constipation, binds other drugs |
| Misoprostol | Prostaglandin | Inhibits acid; enhances mucus | Diarrhea, uterine contractions |
| Metoclopramide | Prokinetic | D2 antagonist + 5-HT4 agonist | Tardive dyskinesia, EPS |
| Domperidone | Prokinetic | D2 antagonist (peripheral) | Hyperprolactinaemia, QT prolongation |
| Lactulose | Osmotic laxative | Osmotic + acidification of colon | Flatulence, bloating, diarrhea |
| Senna | Stimulant laxative | Nerve stimulation via anthrones | Cramping, electrolyte loss with abuse |
| Psyllium | Bulk laxative | Hydrophilic gel formation | Bloating, obstruction if dry |
| Bisacodyl | Stimulant laxative | Mucosal nerve stimulation | Cramping, hypokalemia |
References:
- KD Tripathi, Essentials of Medical Pharmacology, 8th Ed. - Chapter on Drugs for Peptic Ulcer, GI Motility
- Lippincott Illustrated Reviews Pharmacology, 8th Ed. - Ch. 42 (GI Drugs)
- Katzung Basic & Clinical Pharmacology, 16th Ed. - Ch. 62 (GI Pharmacology)
- Goodman & Gilman's Pharmacological Basis of Therapeutics - Metoclopramide section
Drugs use in peptic ulcer classify, pharmacological basis of uses, omeprazole moa, adverse effect Detail answer 2nd yr mbbs pharmacology refer kd tripati
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent - I have all the content and diagrams needed. Here is the complete, exam-ready answer:
DRUGS USED IN PEPTIC ULCER DISEASE
2nd Year MBBS Pharmacology - KD Tripathi Reference
PATHOPHYSIOLOGY OVERVIEW (Basis for Drug Use)
Peptic ulcer results from an imbalance between aggressive and defensive factors:
| Aggressive Factors | Defensive Factors |
|---|---|
| Hydrochloric acid (HCl) | Mucus secretion |
| Pepsin | Bicarbonate secretion |
| H. pylori | Mucosal blood flow |
| NSAIDs | Prostaglandins |
| Bile reflux | Epithelial cell renewal |
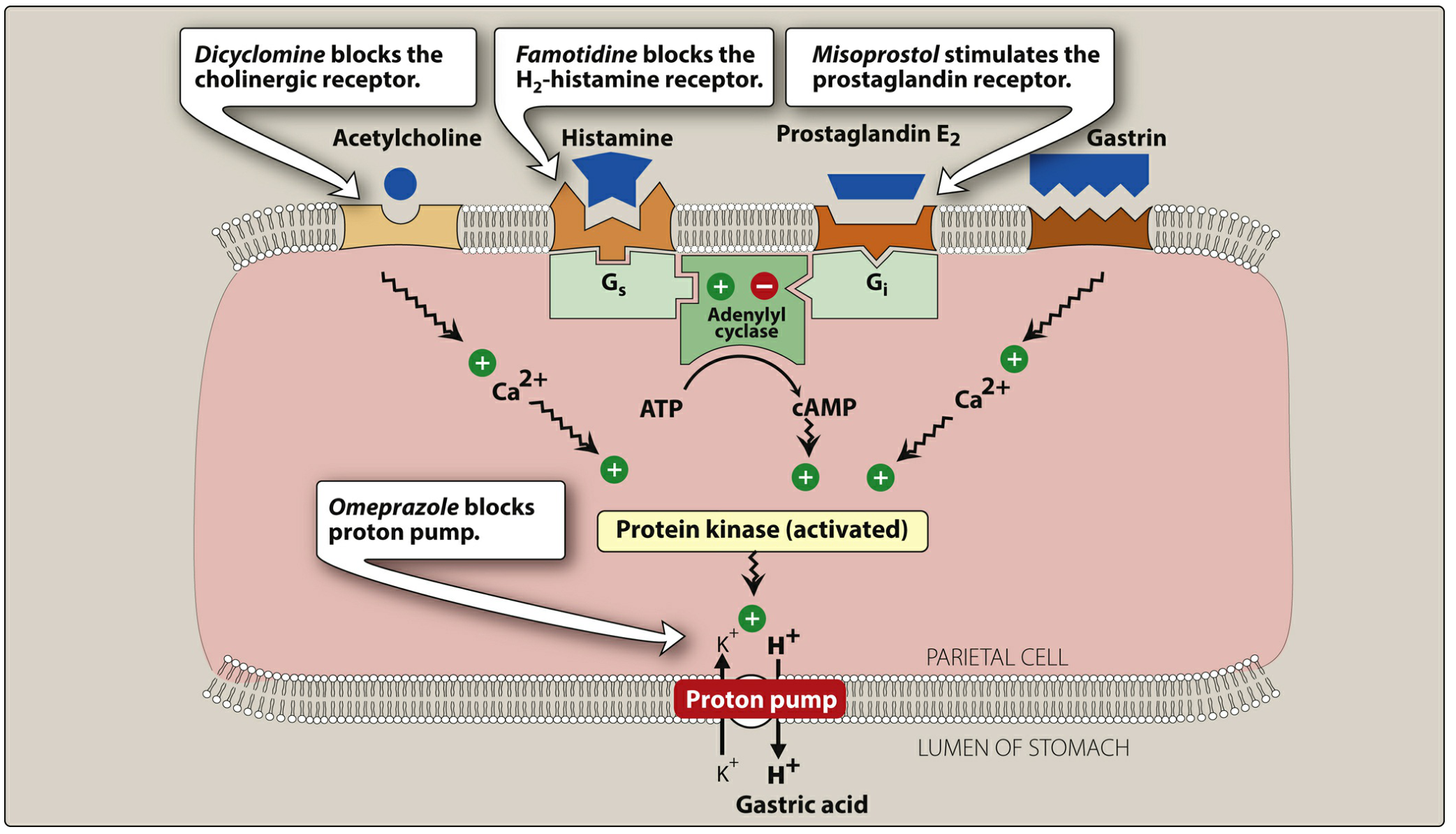
Gastric acid secretion is stimulated by three pathways acting on the parietal cell:
- Acetylcholine (via vagus nerve, M1/M3 receptors) - raises intracellular Ca2+
- Histamine (from ECL cells, via H2 receptors) - raises cAMP via Gs-adenylyl cyclase
- Gastrin (from G cells) - raises intracellular Ca2+
All three converge on activating the H+/K+-ATPase (proton pump) - the final common pathway of acid secretion.
CLASSIFICATION OF DRUGS USED IN PEPTIC ULCER
GROUP I: DRUGS THAT REDUCE ACID SECRETION (Antisecretory Drugs)
A. Proton Pump Inhibitors (PPIs) - Most potent
- Omeprazole, Esomeprazole, Lansoprazole, Pantoprazole, Rabeprazole, Dexlansoprazole
B. H2 Receptor Antagonists
- Cimetidine, Famotidine, Nizatidine
- (Ranitidine withdrawn due to NDMA carcinogen contamination)
C. Anticholinergics (rarely used now)
- Pirenzepine (selective M1 blocker)
- Dicyclomine, Propantheline
GROUP II: ANTACIDS (Acid Neutralizers)
- Aluminium hydroxide Al(OH)3
- Magnesium hydroxide Mg(OH)2
- Calcium carbonate CaCO3
- Sodium bicarbonate NaHCO3
- Combinations: Magaldrate (Mg-Al complex)
GROUP III: MUCOSAL PROTECTIVE / CYTOPROTECTIVE AGENTS
A. Prostaglandin analogues
- Misoprostol (PGE1 analogue)
B. Sucralfate (aluminium hydroxide + sulfated sucrose)
C. Bismuth compounds
- Bismuth subsalicylate, Colloidal bismuth subcitrate (CBS/De-Nol)
D. Carbenoxolone (liquorice derivative - rarely used)
GROUP IV: ANTI-H. PYLORI (ERADICATION THERAPY)
- Amoxicillin
- Clarithromycin
- Metronidazole / Tinidazole
- Tetracycline
- Bismuth compounds (dual role)
PHARMACOLOGICAL BASIS OF EACH GROUP'S USE
1. Proton Pump Inhibitors
Basis: Block the final common pathway of acid secretion - the H+/K+-ATPase enzyme - regardless of the stimulus (ACh, histamine, gastrin). This makes them superior to H2 blockers which only block one stimulatory pathway.
- Inhibit 90-98% of 24-hour acid secretion (vs ~70% by H2 blockers)
- Heal >90% of duodenal ulcers within 4 weeks
- Heal >90% of gastric ulcers within 6-8 weeks
- Essential component of H. pylori eradication regimens (also raise gastric pH, which increases antibiotic efficacy against H. pylori)
2. H2 Receptor Antagonists
Basis: Competitively and reversibly block H2 receptors on the basolateral membrane of parietal cells. Since histamine is the dominant paracrine stimulus for acid secretion:
- Suppress ~70% of 24-hour acid secretion
- Particularly effective against nocturnal acid (night-time secretion is mostly histamine-driven with little food stimulation)
- Healing duodenal ulcers in 4-8 weeks; best given as a single evening dose
3. Antacids
Basis: Are weak bases that chemically neutralize HCl already secreted:
- Raise gastric pH above 4, at which point pepsin becomes inactive (additional benefit)
- Provide rapid symptomatic relief (within minutes)
- Do NOT reduce acid production; do NOT heal ulcers
- Used for symptomatic relief - taken after meals and at bedtime
4. Anticholinergics (Pirenzepine)
Basis: Block M1 receptors on parietal cells and myenteric plexus neurons, reducing vagal stimulation of acid secretion. Reduce acid secretion by ~40-50%. Rarely used now due to availability of superior agents and systemic anticholinergic side effects.
5. Misoprostol (Prostaglandin)
Basis: Prostaglandin E1 analogue. Normally, mucosal PGE1/PGE2:
- Inhibit adenylyl cyclase via Gi → reduce cAMP → decrease acid secretion
- Stimulate mucus and bicarbonate secretion
- Maintain mucosal blood flow
NSAIDs inhibit COX enzymes → reduce prostaglandin synthesis → loss of these protective effects → ulcer formation. Misoprostol replaces these prostaglandins.
Primary use: Prevention of NSAID-induced gastric ulcers in high-risk patients (elderly, prior ulcer history).
6. Sucralfate
Basis: In an acidic environment (pH < 4), sucralfate polymerizes and becomes a viscous paste. It:
- Binds to proteins at the ulcer base forming a physical protective barrier against acid and pepsin
- Stimulates mucus and bicarbonate secretion
- Stimulates prostaglandin synthesis
- Adsorbs pepsin and bile acids
Requires acidic environment; should NOT be combined with PPIs, H2 blockers, or antacids.
7. Bismuth
Basis: Acts as both an antimicrobial and mucosal protector:
- Antimicrobial: Directly kills H. pylori (disrupts bacterial cell wall and membrane)
- Coats the ulcer crater with a protective layer
- Inhibits pepsin activity
- Stimulates mucus secretion
Used as a component of quadruple H. pylori eradication therapy.
8. Antibiotics (H. pylori Eradication)
Basis: H. pylori infection is the primary cause of ~90% of duodenal ulcers and ~70-80% of gastric ulcers. Eradication:
- Achieves >90% cure rate when combined with PPI
- Reduces ulcer recurrence from 60-100% per year to <15%
- Standard regimens:
- Triple therapy (14 days): PPI + Clarithromycin + Amoxicillin (or Metronidazole)
- Quadruple therapy (14 days - first line now): PPI + Bismuth + Metronidazole + Tetracycline
- Concomitant quadruple (no bismuth): PPI + Amoxicillin + Clarithromycin + Metronidazole
OMEPRAZOLE - DETAILED PHARMACOLOGY
Chemistry
Omeprazole is a substituted benzimidazole - a racemic mixture of R- and S-isomers. It is chemically and structurally related to H2 blockers but has a completely different mechanism.
Mechanism of Action (Step-by-Step)
Omeprazole is an inactive prodrug and requires activation in the acidic environment of the parietal cell:
Step 1 - Prodrug protection:
Administered as enteric-coated capsules/tablets. The enteric coat protects omeprazole from destruction by gastric acid in the stomach lumen.
Step 2 - Intestinal absorption:
In the alkaline small intestine, the enteric coat dissolves and omeprazole is absorbed into the bloodstream.
Step 3 - Selective accumulation:
Omeprazole is a lipophilic weak base (pKa ~4). After absorption, it diffuses across lipid membranes and passes from blood into the secretory canaliculus of the parietal cell - which has a very acidic environment (pH ~1-2).
Step 4 - Acid-activated conversion:
In the acidic canaliculus, omeprazole is rapidly protonated (trapped by Henderson-Hasselbalch mechanism, concentrated >1000-fold). It undergoes a chemical conversion to form an active sulfenamide cation (also called sulfenic acid intermediate).
Step 5 - Irreversible enzyme binding:
The active sulfenamide forms covalent disulfide bonds with cysteine residues (Cys813 and Cys892) on the alpha-subunit of the H+/K+-ATPase (proton pump). This irreversibly inactivates the enzyme.
Result: Omeprazole blocks H+ secretion into the stomach regardless of what stimulus is activating the parietal cell (histamine, gastrin, or acetylcholine).
PRODRUG (inactive) → absorbed intestinally → enters parietal cell canaliculus
→ acid-activated to SULFENAMIDE → covalent bond to H+/K+-ATPase → IRREVERSIBLE inhibition
→ H+ secretion blocked → gastric pH rises
Pharmacokinetics of Omeprazole
| Parameter | Value |
|---|---|
| Bioavailability | 40-65% (first-pass metabolism) |
| Plasma half-life | 0.5-1 hour |
| Duration of acid suppression | Up to 24 hours (despite short t½) |
| Protein binding | ~95% |
| Metabolism | Hepatic - primarily CYP2C19 (genetic polymorphism) |
| Excretion | ~80% urine; ~20% faeces |
| Standard dose | 20-40 mg once daily |
| Onset of full effect | 3-4 days of daily dosing |
Key pharmacokinetic explanations:
-
Why short t½ but long action? The pump is inactivated irreversibly. Even though omeprazole is cleared in ~1 hour, acid suppression continues until new proton pumps are synthesized (~18 hours for new pump synthesis). Full acid secretion returns only 3-4 days after stopping the drug.
-
Why take 30-60 minutes before meals? Only actively secreting pumps are in the canaliculus and susceptible to inhibition. Fasting state → only ~10% of pumps active. Meals stimulate pump activation. Taking omeprazole 30-60 minutes before breakfast ensures peak drug levels coincide with maximum pump activity.
-
Why 3-4 days for full effect? Not all pumps are inactivated with the first dose (some pumps are in quiescent vesicles and not yet accessible). Progressive inactivation with each daily dose until steady-state suppression is achieved.
-
CYP2C19 polymorphism: "Poor metabolizers" (higher drug levels) have better acid suppression. "Ultra-rapid metabolizers" may need higher doses.
Therapeutic Uses of Omeprazole / PPIs
- Peptic ulcer disease (gastric and duodenal ulcers) - first-line treatment
- GERD / erosive esophagitis - first-line; heals erosions in 85-90% with once-daily dosing
- Zollinger-Ellison syndrome (gastrinoma-driven massive acid hypersecretion) - high-dose PPIs
- H. pylori eradication - always the PPI component in all regimens
- NSAID-induced ulcers - treatment and prophylaxis (preferred over misoprostol)
- Stress ulcer prophylaxis - in ICU patients (IV esomeprazole/pantoprazole)
- GI bleed from peptic ulcer - high-dose IV PPI (omeprazole 80 mg bolus + 8 mg/hr infusion) reduces rebleeding
- Barrett's esophagus - long-term acid suppression
- Nonulcer dyspepsia - modest benefit
Adverse Effects of Omeprazole
SHORT-TERM (Common, usually mild)
| Adverse Effect | Details |
|---|---|
| Headache | Most common CNS effect |
| Diarrhea / constipation | 1-5% of patients |
| Abdominal pain, nausea, flatulence | GI side effects |
| Dizziness | Occasional |
LONG-TERM (Important - high-yield for exams)
| Adverse Effect | Mechanism | Clinical Significance |
|---|---|---|
| Hypomagnesaemia | Decreased intestinal Mg2+ absorption | Life-threatening hypomagnesaemia with secondary hypocalcaemia; FDA Black Box Warning; monitor Mg in patients on diuretics |
| Osteoporosis / Hip fractures | Reduced calcium absorption (acid needed for insoluble Ca salts); possible osteoclast inhibition | FDA warning for fracture risk (hip, spine, wrist) - monitor bone density in long-term use |
| Vitamin B12 deficiency | Acid needed to release B12 from food proteins; PPI reduces this | Can occur with prolonged use (>3 years) |
| Iron deficiency | Reduced non-heme iron absorption (requires acidic pH) | Relevant in patients with borderline iron stores |
| Clostridium difficile infection | Loss of gastric acid barrier → gut colonization; 2-3x increased risk | Significant in hospitalized patients |
| Community-acquired pneumonia | Gastric bacteria colonize oropharynx | Modest association |
| Enteric infections | Salmonella, Shigella, E. coli, Campylobacter | Especially when travelling |
| Acute Interstitial Nephritis | Immune-mediated; mechanism unclear | Rare but serious; chronic kidney disease risk in long-term users |
| Rebound acid hypersecretion | Hypergastrinaemia during PPI use → ECL cell hyperplasia → excess acid when drug stopped | Occurs 2-4 weeks after stopping; worsened GERD symptoms |
| ECL cell hyperplasia | Hypergastrinaemia stimulates ECL cell proliferation | Carcinoid risk theoretical (proven in rats, not humans) |
DRUG INTERACTIONS
| Interaction | Mechanism | Clinical Impact |
|---|---|---|
| Clopidogrel | Omeprazole/esomeprazole inhibit CYP2C19 → reduced activation of clopidogrel prodrug | Reduced antiplatelet effect; AVOID omeprazole + clopidogrel; use pantoprazole instead |
| Ketoconazole, Itraconazole, iron, atazanavir | These require acidic pH for absorption | Reduced absorption - give 2 hrs apart or avoid |
| Warfarin, diazepam, phenytoin | CYP2C19 competition → increased levels | Monitor INR; adjust doses |
| Methotrexate | PPIs reduce renal tubular secretion | Methotrexate toxicity |
CONTRAINDICATIONS
- Hypersensitivity to benzimidazoles
- Concurrent use with sucralfate (requires acidic pH for activation - PPIs reduce efficacy)
- Caution: severe hepatic impairment (dose reduction needed)
SUMMARY TABLE: KEY DRUG COMPARISONS
| Drug | Class | MOA | Key Adverse Effect | Dose |
|---|---|---|---|---|
| Omeprazole | PPI | Irreversible H+/K+-ATPase blockade (covalent bond) | Hypomagnesaemia, C. diff, B12 deficiency | 20-40 mg OD |
| Famotidine | H2 blocker | Competitive reversible H2 receptor antagonism | Well tolerated; headache, diarrhea | 20-40 mg BD |
| Cimetidine | H2 blocker | Same as above | Anti-androgenic (gynaecomastia, impotence), CYP450 inhibitor - most drug interactions | 400 mg BD |
| Sucralfate | Cytoprotective | Acid-activated polymer; coats ulcer base | Constipation; binds other drugs | 1 g QID |
| Misoprostol | PGE1 analogue | Inhibits acid + stimulates mucus/HCO3 | Diarrhea (dose-limiting); uterine contractions - CONTRAINDICATED in pregnancy | 200 mcg QID |
| Antacids | Acid neutralizer | Chemical: base + HCl → H2O + salt | Al: constipation; Mg: diarrhea; Ca: acid rebound | PRN after meals |
| Bismuth | Mucoprotective + antimicrobial | Coats ulcer; kills H. pylori | Black stools/tongue; constipation; encephalopathy with excess long-term use | Part of quad therapy |
References:
- Lippincott Illustrated Reviews Pharmacology, 8th Ed. - Ch. 42: Gastrointestinal Drugs (p. 1415-1428)
- Katzung Basic & Clinical Pharmacology, 16th Ed. - Ch. 62: Drugs Used in the Treatment of Gastrointestinal Diseases (p. 1699-1708)
- Goodman & Gilman's Pharmacological Basis of Therapeutics - Ch. 53: Pharmacotherapy of Gastric Acidity, Peptic Ulcers, and GERD (p. 1076-1088)
- KD Tripathi Essentials of Medical Pharmacology, 8th Ed. - Section IX: GI Pharmacology
Drugs use in peptic ulcer classify, moa, pharmacological basis of uses, advers effect omeprazole moa, adverse effect Detail answer 2nd yr mbbs pharmacology refer kd tripati
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
All content and images are ready. Here is the complete, detailed, exam-standard answer:
DRUGS USED IN PEPTIC ULCER DISEASE
2nd Year MBBS Pharmacology | KD Tripathi / Lippincott / Katzung Reference
BACKGROUND: PATHOPHYSIOLOGY (Basis for Drug Therapy)
Peptic ulcer is caused by an imbalance between aggressive and defensive factors:
| Aggressive Factors | Defensive Factors |
|---|---|
| Hydrochloric acid (HCl) | Mucus secretion |
| Pepsin | Bicarbonate (HCO3-) secretion |
| H. pylori | Mucosal blood flow |
| NSAIDs / aspirin | Prostaglandins (PGE1, PGE2) |
| Bile salts | Epithelial cell renewal |
Two main causes of PUD:
- Helicobacter pylori infection (~90% of duodenal, ~70-80% of gastric ulcers)
- NSAID/aspirin use (inhibit COX → reduce mucosal prostaglandins)
Physiology of gastric acid secretion - Three stimuli activate the parietal cell:
- Acetylcholine (from vagus nerve, via M1/M3 receptors) → raises intracellular Ca2+
- Histamine (from ECL cells, via H2 receptors) → activates Gs → adenylyl cyclase → raises cAMP
- Gastrin (from G cells, via CCK-B receptors) → raises intracellular Ca2+
All three pathways converge on activating protein kinases → which stimulate the H+/K+-ATPase (proton pump) to secrete H+ ions into the stomach lumen in exchange for K+. This is the final common pathway of acid secretion.
CLASSIFICATION OF ANTIULCER DRUGS
GROUP I: DRUGS THAT REDUCE ACID SECRETION (Antisecretory)
A. Proton Pump Inhibitors (PPIs) ← Most potent class
- Omeprazole, Esomeprazole, Lansoprazole, Pantoprazole, Rabeprazole, Dexlansoprazole
B. H2 Receptor Antagonists
- Cimetidine, Famotidine, Nizatidine
- (Ranitidine withdrawn worldwide due to NDMA carcinogen contamination)
C. Anticholinergics (rarely used now)
- Pirenzepine (selective M1 antagonist)
- Propantheline, Dicyclomine
GROUP II: ANTACIDS (Acid Neutralizers)
- Aluminium hydroxide - Al(OH)3
- Magnesium hydroxide - Mg(OH)2
- Calcium carbonate - CaCO3
- Sodium bicarbonate - NaHCO3
- Combinations: Magaldrate (hydroxymagnesium aluminate)
GROUP III: MUCOSAL PROTECTIVE / CYTOPROTECTIVE AGENTS
A. Prostaglandin analogues
- Misoprostol (PGE1 analogue)
B. Sucralfate (aluminium hydroxide + sulfated sucrose)
C. Bismuth compounds
- Colloidal bismuth subcitrate (CBS / De-Nol)
- Bismuth subsalicylate (Pepto-Bismol)
D. Carbenoxolone (liquorice derivative - rarely used now)
GROUP IV: ANTI-H. PYLORI DRUGS (Eradication Therapy)
- Amoxicillin
- Clarithromycin
- Metronidazole / Tinidazole
- Tetracycline
- Bismuth compounds (dual role - also cytoprotective)
MOA + PHARMACOLOGICAL BASIS OF EACH GROUP
1. PROTON PUMP INHIBITORS (PPIs)
Chemistry: Substituted benzimidazoles (inactive prodrugs)
MOA (Step by Step):
- Administered as enteric-coated inactive prodrug (protects from gastric acid)
- Absorbed in the alkaline small intestine → enters blood
- Being a lipophilic weak base (pKa ~4), diffuses across membranes and selectively accumulates in the acidic secretory canaliculus of parietal cells (concentrated >1000-fold by Henderson-Hasselbalch trapping)
- In the acidic canaliculus, the prodrug is protonated and rapidly converted to an active sulfenamide cation
- The active form forms a covalent disulfide bond with cysteine residues on the H+/K+-ATPase → irreversible inactivation
Result: Block acid secretion regardless of stimulus (histamine, ACh, or gastrin) - they inhibit the final common pathway. Suppress 90-98% of 24-hour acid secretion.
Pharmacological basis of superiority:
- H2 blockers only block histamine stimulation (one of three pathways)
- PPIs block the pump itself - blocking all stimuli simultaneously
- Heal >90% of duodenal ulcers in 4 weeks, >90% of gastric ulcers in 6-8 weeks
- PPIs raise gastric pH, which also increases the efficacy of co-administered antibiotics against H. pylori
Key pharmacokinetic points (Katzung):
| Parameter | Omeprazole | Notes |
|---|---|---|
| Bioavailability | 40-65% | First-pass hepatic metabolism |
| Plasma t½ | 0.5-1 hour | Short, but irreversible action |
| Duration of effect | Up to 24 hours | New pump synthesis takes ~18 hrs |
| Full effect | 3-4 days of daily dosing | Not all pumps blocked with first dose |
| Metabolism | CYP2C19 (major), CYP3A4 (minor) | Genetic polymorphism affects response |
| Dose | 20-40 mg once daily, before meals |
Why take 30-60 min before breakfast? Only actively secreting pumps (in canaliculus) are susceptible. Fasting → only ~10% pumps active. A meal activates more pumps. Taking PPI before breakfast aligns peak drug levels with maximum pump activity.
2. H2 RECEPTOR ANTAGONISTS
Examples: Cimetidine, Famotidine, Nizatidine
MOA:
- Competitively and reversibly block H2 receptors on the basolateral membrane of parietal cells
- Histamine H2 receptor → Gs protein → adenylyl cyclase → cAMP → protein kinase A → activates proton pump
- H2 blockers block this entire signaling cascade by competitive antagonism at the H2 receptor
- They are selective for H2 receptors and have no effect on H1 receptors
- Reduce acid secretion by approximately 70% (basal, food-stimulated, and nocturnal)
Pharmacological basis:
- Nocturnal acid secretion is predominantly histamine-mediated (less food, vagal input minimal)
- H2 blockers are therefore particularly effective for nocturnal acid suppression - important in healing duodenal ulcers
- Evening single dose is sufficient for most patients
- Less potent than PPIs; cannot block gastrin- or ACh-stimulated acid completely
- Tolerance develops with continuous use (tachyphylaxis) - PPIs do not show this
Pharmacokinetics:
- Oral: rapid absorption, peak levels in 1-3 hours
- Widely distributed (including breast milk, across placenta)
- Excreted mainly by kidneys - dose reduction in renal failure
- Famotidine available IV; cimetidine IV/IM
Therapeutic uses:
- Peptic ulcer (duodenal > gastric) - healing in 4-8 weeks
- GERD / heartburn (mild-moderate)
- Stress ulcer prophylaxis (IV infusion in ICU patients)
- Zollinger-Ellison syndrome (adjunct, high doses)
Adverse effects:
| Drug | Adverse Effects |
|---|---|
| All H2 blockers | Headache, diarrhea, constipation, dizziness, fatigue |
| All (IV, elderly) | CNS effects: confusion, delirium, hallucinations |
| Cimetidine specifically | - Anti-androgenic: gynaecomastia, impotence, loss of libido (blocks androgen receptors) |
| - Inhibits CYP450 enzymes (1A2, 2C9, 2D6, 3A4) → increases levels of warfarin, phenytoin, theophylline, diazepam, propranolol - most drug interactions of any H2 blocker | |
| - Hyperprolactinaemia (galactorrhoea) | |
| All (long-term) | Thrombocytopenia, Vitamin B12 deficiency |
| All (renal impairment) | Drug accumulation - dose reduction required |
3. ANTACIDS
Examples: Al(OH)3, Mg(OH)2, CaCO3, NaHCO3
MOA:
- Weak bases that chemically neutralize HCl already present in the stomach lumen:
- Al(OH)3 + 3HCl → AlCl3 + 3H2O
- Mg(OH)2 + 2HCl → MgCl2 + 2H2O
- CaCO3 + 2HCl → CaCl2 + H2O + CO2
- Raise gastric pH above 4 → pepsin becomes inactive (pepsin is inactive at pH >4) → additional benefit
- Do NOT reduce acid production; merely neutralize acid already secreted
Pharmacological basis of use:
- Provide rapid symptomatic relief (within minutes) - faster than any antisecretory drug
- Short duration of action (30-60 min if fasting; up to 3 hrs if taken after meals - food delays gastric emptying)
- Used after meals for maximum effectiveness
- Used as adjuncts - not primary healing agents
Adverse effects:
| Antacid | Adverse Effect | Mechanism |
|---|---|---|
| Aluminium hydroxide | Constipation | Aluminium inhibits bowel motility |
| Magnesium hydroxide | Diarrhea | Mg2+ draws water into bowel osmotically |
| Combination Al+Mg | Balanced bowel effect | Offsetting effects |
| Calcium carbonate | Acid rebound (milk-alkali syndrome with excess) | Calcium stimulates gastrin release |
| Sodium bicarbonate | Systemic alkalosis, sodium load, CO2 belching | Absorbed systemically |
| All antacids | Impair absorption of other drugs (tetracyclines, fluoroquinolones, iron, ketoconazole) | Chelation / pH alteration |
| Mg2+, Al3+ antacids | Accumulate in renal failure → hypermagnesaemia, aluminium toxicity | Reduced renal clearance |
4. ANTICHOLINERGICS (Pirenzepine)
MOA:
- Pirenzepine is a selective M1 muscarinic receptor antagonist
- Blocks M1 receptors on parietal cells and on myenteric plexus neurons (which mediate vagal stimulation)
- Reduces vagal (ACh-mediated) stimulation of acid secretion by ~40-50%
Pharmacological basis: Vagal activation is the primary stimulus during the cephalic phase (sight/smell/taste of food). Blocking M1 reduces this. Less potent than PPIs or H2 blockers.
Adverse effects: Dry mouth, blurred vision, urinary retention, constipation, tachycardia (classic anticholinergic effects) - limits use considerably. Pirenzepine is selective and has fewer systemic effects than non-selective anticholinergics.
Now rarely used - replaced by PPIs and H2 blockers.
5. MISOPROSTOL (Prostaglandin Analogue)
MOA:
- Synthetic analogue of Prostaglandin E1 (PGE1)
- PGE1 normally acts via Gi protein → inhibits adenylyl cyclase → reduces cAMP → decreases acid secretion from parietal cells
- Also directly stimulates mucus and bicarbonate secretion from gastric epithelial cells (cytoprotective effect)
- Maintains mucosal blood flow
Normal PGE1/PGE2 in the stomach is produced via the COX-1 enzyme. NSAIDs/aspirin inhibit COX-1 → reduce mucosal prostaglandins → loss of protection → ulcer formation.
Misoprostol replaces these prostaglandins, restoring both the acid-suppressive and cytoprotective functions.
Pharmacological basis:
- Specifically used for prevention of NSAID-induced gastric ulcers in high-risk patients (elderly, prior ulcer history, high-dose NSAID users)
- PPIs are now preferred for this indication due to better tolerability
Adverse effects:
- Diarrhea (dose-limiting, occurs in ~30%) - most common reason for discontinuation
- Abdominal cramping
- Uterine contractions - CONTRAINDICATED IN PREGNANCY (used medically for abortion/cervical ripening)
- Nausea, vomiting
6. SUCRALFATE
Chemistry: Complex of aluminium hydroxide + sulfated sucrose
MOA:
- In an acidic environment (pH < 4), sucralfate undergoes polymerization into a viscous, sticky gel
- Binds to positively charged proteins at the base of the ulcer crater (especially in necrotic tissue), forming a physical protective barrier
- This barrier protects the ulcer from acid, pepsin, and bile salts
- Also stimulates mucus and bicarbonate secretion
- Adsorbs pepsin and bile salts directly
- Stimulates prostaglandin synthesis locally
- Promotes epithelial cell growth and healing
Pharmacological basis:
- Acts locally; minimal systemic absorption
- Effective for duodenal ulcers and stress ulcer prophylaxis
Requires acidic pH for activation - therefore should NOT be combined with PPIs, H2 blockers, or antacids.
Adverse effects:
- Constipation (most common - due to Al content)
- Binds other drugs and impairs their absorption (tetracyclines, fluoroquinolones, digoxin, phenytoin) - take 2 hours apart
- Nausea, dry mouth
7. BISMUTH COMPOUNDS
MOA (dual action):
A. Antimicrobial:
- Directly kills H. pylori - disrupts bacterial cell wall, prevents adhesion to gastric mucosa, inhibits urease, phospholipase, and proteases of the bacteria
B. Mucoprotective:
- Coats the ulcer crater with a glycoprotein-bismuth complex
- Inhibits pepsin activity
- Stimulates mucus secretion
- Binds to glycoproteins in necrotic mucosal tissue
Pharmacological basis: Used as a fourth drug in quadruple H. pylori eradication therapy (PPI + Bismuth + Metronidazole + Tetracycline). The dual antimicrobial + mucoprotective mechanism makes it particularly valuable.
Adverse effects:
- Black stools and black tongue (bismuth sulfide - harmless, warn patients)
- Constipation
- Bismuth encephalopathy with excessive long-term use (now rare with recommended doses)
- Nausea
8. ANTI-H. PYLORI DRUGS
MOA: Standard antibiotics acting on H. pylori cell wall synthesis (amoxicillin, tetracycline), protein synthesis (clarithromycin), and DNA/nitroreductase mechanism (metronidazole).
Pharmacological basis:
- H. pylori causes 90% of duodenal ulcers. Eradication achieves true cure
- Recurrence rate with acid suppression alone = 60-100% per year
- Recurrence after successful eradication = <15%
- PPI is always co-administered to: (a) suppress acid directly, (b) raise gastric pH → increases antibiotic efficacy against H. pylori
Standard regimens:
- Triple therapy (14 days): PPI (BD) + Clarithromycin 500 mg (BD) + Amoxicillin 1g (BD) [or Metronidazole if penicillin allergy]
- Quadruple therapy (14 days, now first-line): PPI (BD) + Bismuth 524 mg (QID) + Metronidazole 500 mg (QID) + Tetracycline 500 mg (QID)
- Eradication success rate: >90% with quadruple therapy
OMEPRAZOLE - COMPLETE DETAILED PHARMACOLOGY
Chemistry
A substituted benzimidazole - racemic mixture of R- and S-isomers (S-isomer = esomeprazole, which has slightly higher bioavailability). Contains a pyridine ring and a benzimidazole ring connected by a sulfinyl group.
Mechanism of Action - Detailed (Most Asked in Exams)
Omeprazole is an inactive prodrug that requires activation in the acidic environment of the parietal cell.
Step 1: Administered as enteric-coated capsule - protects the acid-labile prodrug from destruction in stomach lumen.
Step 2: The coating dissolves in the alkaline small intestine → drug is absorbed into bloodstream.
Step 3: Being a lipophilic weak base (pKa ~4), omeprazole diffuses freely across membranes. It enters the parietal cell and accumulates in the secretory canaliculus (pH ~1-2). The Henderson-Hasselbalch principle causes it to become protonated and trapped there - concentrated >1000-fold.
Step 4: In this intensely acidic environment, omeprazole undergoes rapid chemical conversion → active sulfenamide cation (also called sulfenic acid/thioether).
Step 5: The active sulfenamide forms a covalent disulfide bond with cysteine residues (Cys813 and Cys892) on the alpha-subunit of H+/K+-ATPase. This bond is IRREVERSIBLE.
Step 6: The H+/K+-ATPase is permanently inactivated → H+ ions cannot be secreted → acid secretion stops.
PRODRUG (inactive, acid labile)
↓ [enteric-coated → intestinal absorption]
Bloodstream → parietal cell
↓ [accumulates in canaliculus, pH 1-2]
Active SULFENAMIDE CATION
↓ [covalent bond to Cys813/892]
H+/K+-ATPase - IRREVERSIBLY INACTIVATED
↓
No H+ secreted → Gastric pH rises
Why omeprazole is the most potent antiulcer drug:
- Blocks all three stimulatory pathways (ACh, histamine, gastrin) simultaneously by acting at the final common pump
- H2 blockers only block histamine (one of three); gastrin and ACh pathways still active
- PPIs achieve 90-98% suppression of 24-hour acid; H2 blockers achieve only ~70%
Pharmacokinetics
| Parameter | Detail |
|---|---|
| Formulation | Enteric-coated capsule/tablet (protect from gastric acid) |
| Absorption | Intestinal; food reduces bioavailability by ~50% - take on empty stomach |
| Bioavailability | 40-65% (increases with repeated doses due to reduced first-pass as gastric pH rises) |
| Plasma protein binding | ~95% |
| Plasma t½ | 0.5-1 hour |
| Duration of acid suppression | Up to 24 hours (irreversible pump inactivation) |
| Onset of full effect | 3-4 days of daily dosing |
| Metabolism | CYP2C19 (major) + CYP3A4 (minor); hepatic |
| Excretion | ~80% urine as metabolites; ~20% feces |
| Dose | 20-40 mg once daily, 30-60 min before breakfast |
Key explanations students must know:
-
Short t½ (~1 hr) but 24-hr action: Pump inactivation is irreversible. Even after omeprazole is cleared from plasma, the pump remains inactive until new H+/K+-ATPase is synthesized (~18 hours). Hence acid suppression outlasts drug levels.
-
Why 3-4 days for full effect: Only actively secreting pumps (those in the canaliculus) are accessible to omeprazole. On day 1, many pumps are quiescent (in tubulovesicles) and not blocked. With each daily dose more pumps are inactivated as they activate. Full suppression (~70% of all pumps) is achieved by day 3-4.
-
Take before breakfast: Meals stimulate pumps to move from vesicles to canaliculus (active state). Taking omeprazole 30-60 min before breakfast ensures peak drug concentration coincides with maximum pump activation, maximizing the number of pumps blocked.
Therapeutic Uses of Omeprazole
- Peptic ulcer disease (duodenal and gastric) - first-line; heals >90% in 4-8 weeks
- GERD / erosive esophagitis - first-line; 85-90% symptom relief and healing with once-daily dose
- Zollinger-Ellison syndrome - high doses (60-120 mg/day omeprazole) for massive acid hypersecretion from gastrinoma
- H. pylori eradication - always the PPI component in all triple/quadruple regimens (acid suppression + enhances antibiotic efficacy)
- NSAID-induced ulcers - treatment and prevention (preferred over misoprostol)
- Stress ulcer prophylaxis in ICU patients (IV esomeprazole/pantoprazole)
- GI bleed from peptic ulcer - high-dose IV PPI (80 mg bolus + 8 mg/hr infusion) reduces rebleeding by raising pH >6, promoting clot stability
- Barrett's esophagus - long-term maintenance
- Nonulcer dyspepsia - modest benefit
Adverse Effects of Omeprazole
SHORT-TERM (Common)
| Effect | Frequency | Notes |
|---|---|---|
| Headache | Common | Most frequent CNS complaint |
| Diarrhea | 1-5% | |
| Abdominal pain / nausea | 1-5% | GI discomfort |
| Flatulence, constipation | Occasional | |
| Dizziness | Rare |
LONG-TERM (High Yield - Exams)
| Adverse Effect | Mechanism | Details |
|---|---|---|
| Hypomagnesaemia ⭐ | Reduced intestinal Mg2+ absorption | Life-threatening; secondary hypocalcaemia; FDA Black Box Warning; monitor Mg in patients on diuretics; reverses on stopping PPI |
| Osteoporosis / Fractures ⭐ | Reduced Ca2+ absorption (acid needed for insoluble Ca salts) + possible osteoclast inhibition | FDA mandated warning for hip, spine, wrist fractures with long-term use; supplement calcium + monitor bone density |
| Vitamin B12 deficiency | Acid needed to cleave B12 from food proteins; PPI reduces this | Occurs with >3 years use; monitor B12 in long-term users |
| Iron deficiency | Non-heme iron absorption requires acidic pH | Risk in patients with borderline stores |
| C. difficile infection ⭐ | Loss of gastric acid barrier → gut colonization; 2-3x increased risk | Significant in hospitalized patients |
| Community-acquired pneumonia | Gastric bacteria ascend to oropharynx → aspiration | Modest association |
| Enteric infections | Salmonella, Shigella, E. coli, Campylobacter, etc. | Loss of acid barrier; risk when travelling |
| Acute interstitial nephritis | Immune-mediated renal inflammation | Rare but serious; long-term use associated with chronic kidney disease |
| Rebound acid hypersecretion | PPI → hypergastrinaemia → ECL cell hyperplasia → excess pumps → acid surge when drug stopped | Occurs 2-4 weeks after stopping; may worsen GERD transiently |
| Hypergastrinaemia | Acid suppression removes feedback inhibition of gastrin secretion | Gastrin rises 1.5-2x; ECL hyperplasia in long-term users (carcinoid risk theoretical, not documented in humans) |
DRUG INTERACTIONS (High Yield)
| Drug | Interaction | Mechanism | Action |
|---|---|---|---|
| Clopidogrel ⭐ | Reduced antiplatelet effect | Omeprazole/esomeprazole inhibit CYP2C19 → impair activation of clopidogrel prodrug | AVOID combination; use pantoprazole instead |
| Warfarin | Increased anticoagulant effect | CYP2C19 inhibition → raised warfarin levels | Monitor INR |
| Diazepam, phenytoin | Increased drug levels | CYP2C19/3A4 competition | Monitor and adjust |
| Ketoconazole, itraconazole, iron, atazanavir | Reduced absorption | These require acidic gastric pH for dissolution/absorption | Separate administration; consider alternative |
| Methotrexate | Methotrexate toxicity | PPIs reduce renal tubular secretion | Use with caution |
| Sucralfate | Reduced sucralfate efficacy | Sucralfate requires acid (pH<4) for activation; PPI raises pH | Do not co-administer |
COMPARATIVE SUMMARY TABLE
| Drug | Class | MOA | Acid Suppression | Heals Ulcer | Key Adverse Effect |
|---|---|---|---|---|---|
| Omeprazole | PPI | Irreversible H+/K+-ATPase block | 90-98% | Yes (4-8 wks) | Hypomagnesaemia, C. diff, B12 deficiency, fractures |
| Famotidine | H2 blocker | Competitive H2 receptor block | ~70% | Yes (4-8 wks) | Well tolerated; headache, diarrhea |
| Cimetidine | H2 blocker | Same as above | ~70% | Yes | Anti-androgenic, multiple CYP450 drug interactions |
| Misoprostol | PGE1 analogue | Inhibits acid + stimulates mucus | Moderate | Yes | Diarrhea, uterine contractions; avoid in pregnancy |
| Sucralfate | Cytoprotective | Coats ulcer physically (acid-activated polymer) | None | Yes (duodenal) | Constipation, binds other drugs |
| Antacids | Neutralizer | Chemical neutralization of HCl | None (neutralize) | No | Al: constipation; Mg: diarrhea; Ca: rebound |
| Bismuth | Antimicrobial + mucoprotective | Kills H. pylori + coats ulcer | None | As part of regimen | Black stools/tongue, encephalopathy (excess) |
QUICK MEMORY AID - Drug Classification (KD Tripathi Style)
ANTIULCER DRUGS
│
├─ REDUCE ACID SECRETION
│ ├─ PPIs: Omeprazole, Lansoprazole, Pantoprazole, Esomeprazole, Rabeprazole
│ ├─ H2 Blockers: Cimetidine, Famotidine, Nizatidine
│ └─ Anticholinergics: Pirenzepine (M1 selective)
│
├─ NEUTRALIZE ACID
│ └─ Antacids: Al(OH)3, Mg(OH)2, CaCO3, NaHCO3
│
├─ PROTECT MUCOSA (Cytoprotective)
│ ├─ Misoprostol (PGE1 analogue)
│ ├─ Sucralfate
│ ├─ Bismuth compounds
│ └─ Carbenoxolone
│
└─ ERADICATE H. PYLORI
└─ Antibiotics: Amoxicillin, Clarithromycin, Metronidazole, Tetracycline + Bismuth
Sources:
- KD Tripathi, Essentials of Medical Pharmacology, 8th Ed. - Ch. Drugs for Peptic Ulcer
- Lippincott Illustrated Reviews Pharmacology, 8th Ed. - Ch. 42, pp. 1415-1428
- Katzung Basic & Clinical Pharmacology, 16th Ed. - Ch. 62, pp. 1699-1708
- Goodman & Gilman's Pharmacological Basis of Therapeutics - Ch. 53
This is a shared conversation. Sign in to Orris to start your own chat.