Schannoma
Reading File
Finding Sources
Finding Sources
Searching PubMed
schwannoma diagnosis treatment
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent - I now have rich, comprehensive information from multiple authoritative textbooks. Here is the full clinical overview:
Schwannoma (Neurilemmoma)
Definition & Origin
A schwannoma is a generally benign, encapsulated tumor arising from Schwann cells of peripheral, cranial, or spinal nerve sheaths. Also called a neurilemmoma, it is the most common benign peripheral nerve sheath tumor. Unlike neurofibromas, schwannomas do not infiltrate adjacent nerve fascicles - they push the nerve fibers aside, which is the key to nerve-sparing surgery.
- Harrison's Principles of Internal Medicine 22E, p. 765
- Andrews' Diseases of the Skin, p. 719
Epidemiology & Associations
| Feature | Detail |
|---|---|
| Sex | More common in women (peripheral type) |
| Usual presentation | Solitary, sporadic |
| NF2 (chromosome 22) | Bilateral vestibular schwannomas; multiple schwannomas |
| NF1 (chromosome 17q11.2) | Spinal nerve root schwannomas (less commonly) |
| Carney syndrome | Melanotic psammomatous schwannoma + spotty pigmentation + myxomas + endocrine overactivity |
Multiple schwannomas without NF features may be sporadic or familial (schwannomatosis).
Clinical Types & Locations
1. Vestibular Schwannoma (Acoustic Neuroma) - Most Common
- Arises from the vestibular portion of CN VIII
- Accounts for ~9% of all primary brain tumors
- Symptoms: Progressive unilateral hearing loss, tinnitus, dizziness; with large tumors - brainstem/cerebellar compression
- NF2 patients get bilateral vestibular schwannomas
2. Peripheral Schwannoma
- Solitary nodule, 3-30 mm in diameter
- Soft/firm, pale pink or yellowish
- Common sites: flexor surfaces of arms/wrists/knees, scalp, neck, tongue
- May or may not be painful; positive Tinel sign is characteristic
3. Plexiform Schwannoma
- Involves multiple fascicles; occurs as solitary or multiple lesions
- May be isolated or associated with NF1, NF2, or schwannomatosis
4. Ancient Schwannoma
- Long-standing schwannoma with nuclear atypia - a benign degenerative change, NOT malignant
- No mitotic figures; must be distinguished from malignant peripheral nerve sheath tumor (MPNST)
Imaging (MRI)
MRI is the investigation of choice:
- Fusiform mass along the course of a major peripheral nerve
- "Split fat sign" on T1: a rim of fat surrounding the lesion
- "Target sign" on T2 (seen in ~50%): decreased central T2 signal with increased peripheral T2 signal - suggests benign diagnosis
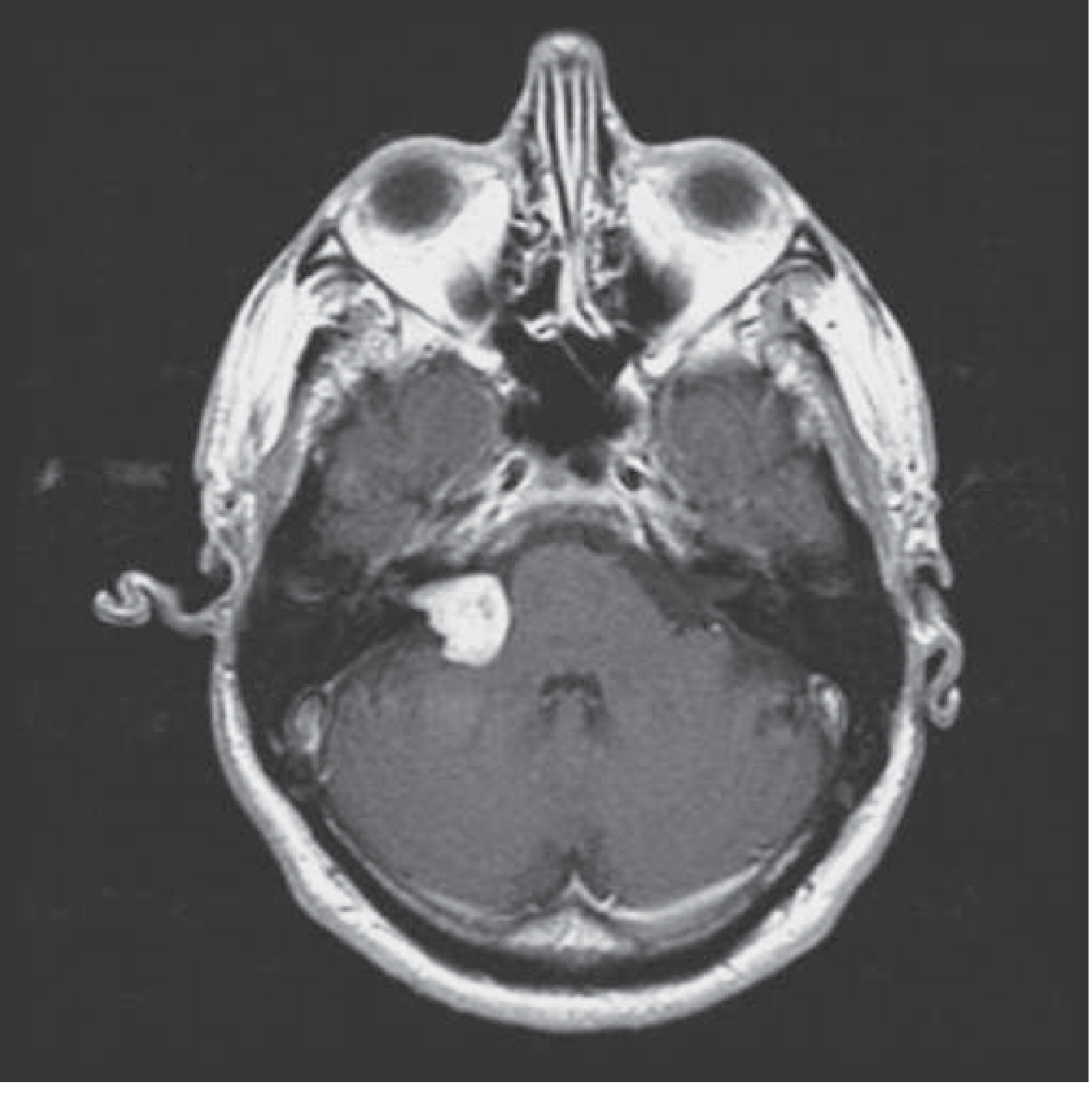
- Vestibular schwannoma: densely enhancing lesion, enlarges the internal auditory canal, extends into the cerebellopontine angle (CPA)
Postgadolinium MRI of right vestibular schwannoma (Harrison's, p. 765):
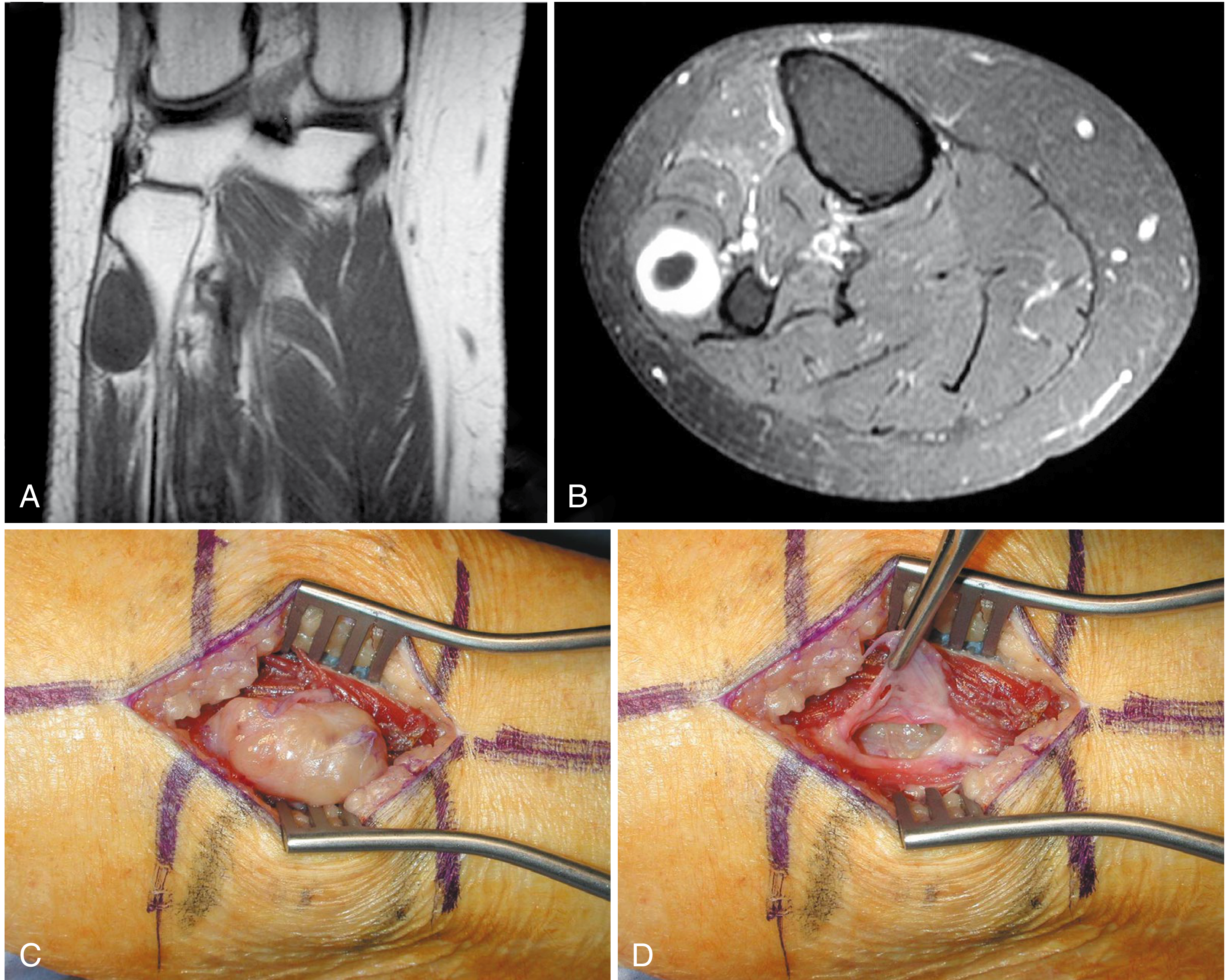
Peripheral schwannoma of peroneal nerve with intraoperative view (Campbell's Orthopaedics 15e):
Red flags for malignancy on imaging:
- Rapid size increase
- Peripheral enhancement pattern
- Perilesional soft-tissue edema
- Cystic change within the tumor
- Increased FDG uptake on PET scan
Histopathology - The Key Features
Schwannomas have two characteristic tissue patterns:
| Pattern | Description | Gross appearance |
|---|---|---|
| Antoni A | Compact spindle cells with marked nuclear palisading; Verocay bodies (two rows of palisading nuclei separated by fibrillary material) | Hard, firm |
| Antoni B | Loose, myxomatous, degenerative; ectatic/thick-walled blood vessels; cystic spaces | Soft, edematous |
Immunohistochemistry:
- S-100 positive (nuclear and cytoplasmic) - hallmark
- Also positive for vimentin and myelin basic protein (in Antoni A)
- EMA-positive capsule (derived from perineurium)
- Very few/no nerve fibers within the tumor bulk (a compressed nerve may be seen at one edge)
Treatment
Peripheral schwannomas:
- Surgical excision via longitudinal perineurial incision with careful blunt dissection
- Tumor can be shelled out without sacrificing nerve fascicles
- Excision is almost invariably curative
- Transient neurologic deficits occur in ~1/3 of cases post-resection
- Risk of neurologic injury is higher with tumors > 3 cm, age > 50, and longer symptom duration
Vestibular schwannomas:
- Very small, asymptomatic lesions: observe with serial MRIs
- Larger/symptomatic lesions: surgery or stereotactic radiosurgery (SRS)
- In patients with small tumors and intact hearing: early surgical intervention improves chance of hearing preservation
Malignant variant (MPNST - "malignant schwannoma"):
- Arises from long-standing neurofibromas in NF1 setting (NOT from benign schwannomas)
- Treatment: wide resection + radiotherapy
Key Differentials
| Feature | Schwannoma | Neurofibroma |
|---|---|---|
| Encapsulation | Yes | No |
| Nerve involvement | Displaces fascicles | Infiltrates fascicles |
| NF association | NF2 (also NF1) | NF1 (von Recklinghausen) |
| S-100 | Positive | Positive (less uniform) |
| Malignant potential | Very rare | Higher (plexiform type in NF1) |
| Surgery | Nerve-sparing excision possible | May require nerve sacrifice |
Recent Evidence (2024-2026)
Two recent systematic reviews are worth noting for vestibular schwannoma management:
- A 2024 network meta-analysis (PMID 39627752) compared treatment options for unilateral vestibular schwannoma across surgery, SRS, and observation.
- A 2026 systematic review and meta-analysis (PMID 41794963) in Journal of Neurology evaluated quality of life across all three management strategies (observation, SRS, microsurgery), providing patient-centred guidance.
Sources: Harrison's Principles of Internal Medicine 22E (p. 765) | Andrews' Diseases of the Skin (p. 719) | Campbell's Operative Orthopaedics 15e (p. 1262-1263)
This is a shared conversation. Sign in to Orris to start your own chat.