Treatment of acute pancreatitis
Reading File
Finding Sources
Searching PubMed
"acute pancreatitis" AND management
Finding Sources
Searching PubMed
"acute pancreatitis" AND treatment
Finding Sources
Reading Article
PMID: 38857482
Reading Article
PMID: 40651900
Reading File
Reading File
Loading Image
Reading File
Reading Article
PMID: 40085761
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full response.
Treatment of Acute Pancreatitis
Management algorithm (from Maingot's Abdominal Operations):
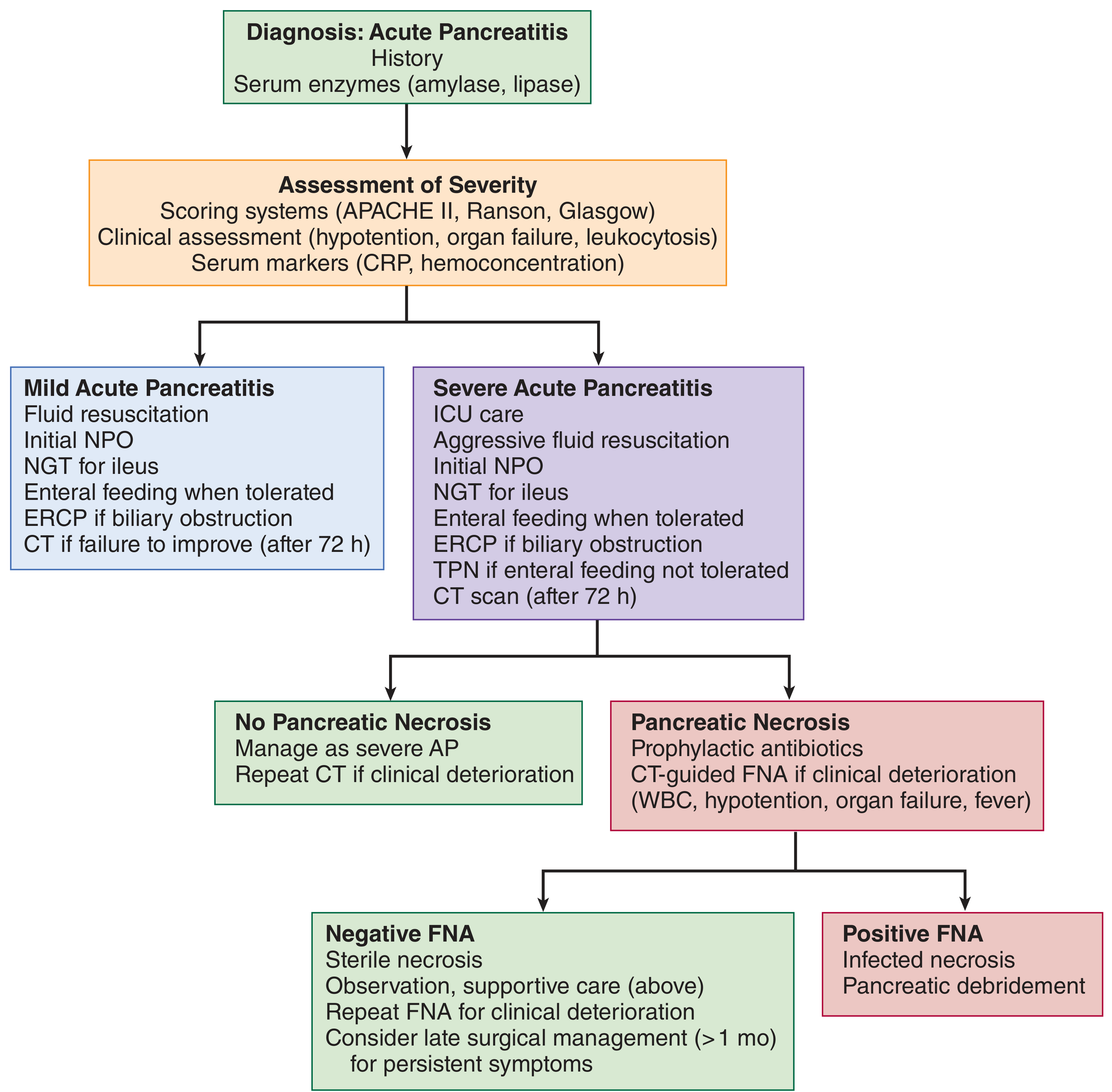
1. Diagnosis & Severity Assessment
Acute pancreatitis is diagnosed when at least 2 of 3 criteria are met:
- Characteristic epigastric pain (often radiating to the back)
- Serum lipase or amylase >3x upper limit of normal (lipase preferred - higher sensitivity/specificity)
- Characteristic findings on imaging (CT/MRI)
Note: The degree of enzyme elevation does not correlate with disease severity.
Severity classification (Revised Atlanta 2012):
| Severity | Definition |
|---|---|
| Mild | No organ failure, no local/systemic complications |
| Moderately severe | Transient organ failure (<48 h) and/or local or systemic complications |
| Severe | Persistent organ failure (>48 h) - single or multi-organ |
| Critical | Persistent organ failure + infected pancreatic necrosis |
Scoring tools used in practice: Ranson criteria, APACHE II, Glasgow, BISAP, CT Severity Index (CTSI). They have similar predictive accuracy, with different strengths for each clinical setting.
2. Fluid Resuscitation (MOST IMPORTANT EARLY INTERVENTION)
Early, aggressive IV fluid resuscitation is the cornerstone of initial treatment. Fluid therapy prevents systemic hypoperfusion and pancreatic microvascular ischemia.
-
Lactated Ringer's (LR) is preferred over normal saline (NS)
- LR is more physiologic (balanced electrolyte solution)
- LR may provide anti-inflammatory effects via lactate-mediated mechanisms
- A 2025 meta-analysis of 6 RCTs (n=1,500 patients) showed LR vs. NS: significantly lower risk of moderate-to-severe AP (OR 0.48; 95% CI 0.34-0.67), shorter hospital stay, lower ICU admission rate (RR 0.42), and fewer local complications (Zhao et al., Int J Surg 2025, PMID 40085761)
-
Rate: Aggressive resuscitation - typically 250-500 mL/h during the first 12-24 hours in moderate-severe disease; careful goal-directed therapy to avoid overhydration
-
Titrate to: urine output >0.5 mL/kg/h, HR <100, MAP >65 mmHg, BUN trending down
3. Pain Management
- Adequate analgesia is essential; IV opioids (morphine, hydromorphone, fentanyl) are widely used and are safe
- NSAIDs and acetaminophen can supplement but are often insufficient alone in acute presentations
- There is no evidence that one analgesic is superior to another specifically for pancreatitis
- Epidural analgesia is an option in severe cases
4. Nutrition
Key principle: Enteral feeding is strongly preferred over TPN.
- Mild AP: Oral diet should be restarted as soon as it is tolerated (often within 24-48 hours). There is no need to wait until pain resolves or amylase normalizes.
- Moderate-severe AP:
- Early enteral nutrition within 24-72 hours of admission is associated with decreased mortality, organ failure, and infectious complications vs. delayed nutrition
- Nasogastric (NG) or nasojejunal (NJ) tube feeding - RCTs show no significant difference in outcomes between gastric vs. jejunal delivery, so a nasogastric tube is acceptable
- NPO initially if there is ileus or if the patient cannot tolerate any intake
- TPN (parenteral nutrition) is reserved for cases where enteral feeding is not tolerated (refractory vomiting, intestinal obstruction, high-output fistula)
- Enteral nutrition maintains gut barrier function, reduces bacterial translocation, and reduces risk of infectious complications
5. Antibiotics
- Prophylactic antibiotics are NOT indicated in acute pancreatitis - this includes even severe or necrotizing pancreatitis without evidence of infection
- Harrison's (2025 ed.): "Prophylactic antibiotics are no longer recommended for severe acute pancreatitis"
- Antibiotics ARE indicated for:
- Documented infected pancreatic necrosis (confirmed by FNA or gas on CT, or clinical deterioration with fever/leukocytosis)
- Cholangitis (ascending cholangitis complicating biliary pancreatitis)
- Other clear sources of bacterial sepsis
- Preferred agents for infected necrosis: carbapenems (imipenem, meropenem) or fluoroquinolones + metronidazole (good pancreatic tissue penetration)
6. Role of ERCP
- ERCP is indicated in:
- Acute cholangitis complicating gallstone pancreatitis (urgent, within 24-72 hours)
- Biliary obstruction with evidence of persistent common bile duct stones
- ERCP is NOT indicated in mild biliary pancreatitis without cholangitis or persistent biliary obstruction (does not improve outcomes and risks complications)
- Rectal indomethacin (NSAIDs) or pancreatic duct stenting is used to prevent post-ERCP pancreatitis in high-risk patients
7. Management of Complications
Pancreatic Necrosis
| Type | Management |
|---|---|
| Sterile necrosis | Conservative - supportive care, antibiotics NOT required |
| Infected necrosis | Antibiotics (carbapenems preferred) + drainage/debridement |
When to intervene in infected necrosis:
- Minimally invasive approach preferred (step-up approach)
- CT/EUS-guided percutaneous or endoscopic drainage as first step
- Video-assisted retroperitoneal debridement (VARD) or endoscopic necrosectomy if drainage fails
- Open surgical necrosectomy - last resort (high morbidity/mortality)
- Intervention ideally delayed >4 weeks to allow "walled-off necrosis" (WON) to mature (better defined walls, safer to drain)
- FNA is now used less routinely; clinical judgment + CT findings guide decisions
Pseudocyst
- Most resolve spontaneously
- Drainage indicated if: symptomatic (pain, gastric outlet obstruction), infection, enlarging, or >6 weeks without resolution
- Endoscopic (EUS-guided cyst-gastrostomy or cyst-duodenostomy) is preferred over surgical drainage
Pancreatic Ascites/Pleural Effusion
- From ductal disruption; ERCP with stenting ± somatostatin analogue
8. Special Situations
Biliary/Gallstone Pancreatitis
- Cholecystectomy should be performed before discharge (or at least during the same hospitalization) in mild disease to prevent recurrence
- In severe disease, cholecystectomy is deferred until recovery
Hypertriglyceridemia-induced Pancreatitis
- Insulin infusion or plasmapheresis to rapidly lower triglycerides (target <500 mg/dL)
- Fibrates and dietary fat restriction for long-term prevention
Alcohol-induced Pancreatitis
- Alcohol cessation counseling and treatment (reduces recurrence and progression to chronic pancreatitis)
9. ICU Indications
Transfer to ICU is warranted if:
- Persistent organ failure (renal, respiratory, cardiovascular)
- APACHE II score >8 or Ranson score >3 at 48 hours
- Clinical deterioration despite initial management
- Septic shock from infected necrosis
10. Summary of Key Guideline Recommendations (2024-2025)
The 2024 ACG Guidelines (Tenner et al.) and the IAP Revised Guidelines 2025 (endorsed by APA, EPC, IPC, JPS) emphasize:
- LR preferred over NS for fluid resuscitation
- Early enteral nutrition within 24-72 hours
- No prophylactic antibiotics in the absence of infection
- Minimally invasive, step-up approach for infected necrosis
- Cholecystectomy before discharge for biliary pancreatitis
- ERCP only for cholangitis/biliary obstruction
- Conservative management for sterile complications whenever possible
Sources:
- Rosen's Emergency Medicine, 10th ed. - Chapter 77
- Maingot's Abdominal Operations - Chapter 55 (Complications of AP)
- Harrison's Principles of Internal Medicine, 22nd ed. (2025) - Chapter 7.39
- Washington Manual of Medical Therapeutics - Nutrition section
- ACG Guidelines 2024 (PMID 38857482)
- IAP/APA/EPC/IPC/JPS Revised Guidelines 2025 (PMID 40651900)
- Zhao et al., LR vs NS meta-analysis, Int J Surg 2025 (PMID 40085761)
This is a shared conversation. Sign in to Orris to start your own chat.