Pterigyum
Reading File
Finding Sources
Searching PubMed
pterygium
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent clinical images. I now have comprehensive information from multiple authoritative sources. Here is the full answer:
Pterygium
Definition
A pterygium (plural: pterygia) is a triangular fibrovascular sub-epithelial ingrowth of degenerative bulbar conjunctival tissue that grows over the limbus onto the cornea. The name comes from the Greek word for "wing" - it has a characteristic wing-shaped appearance.
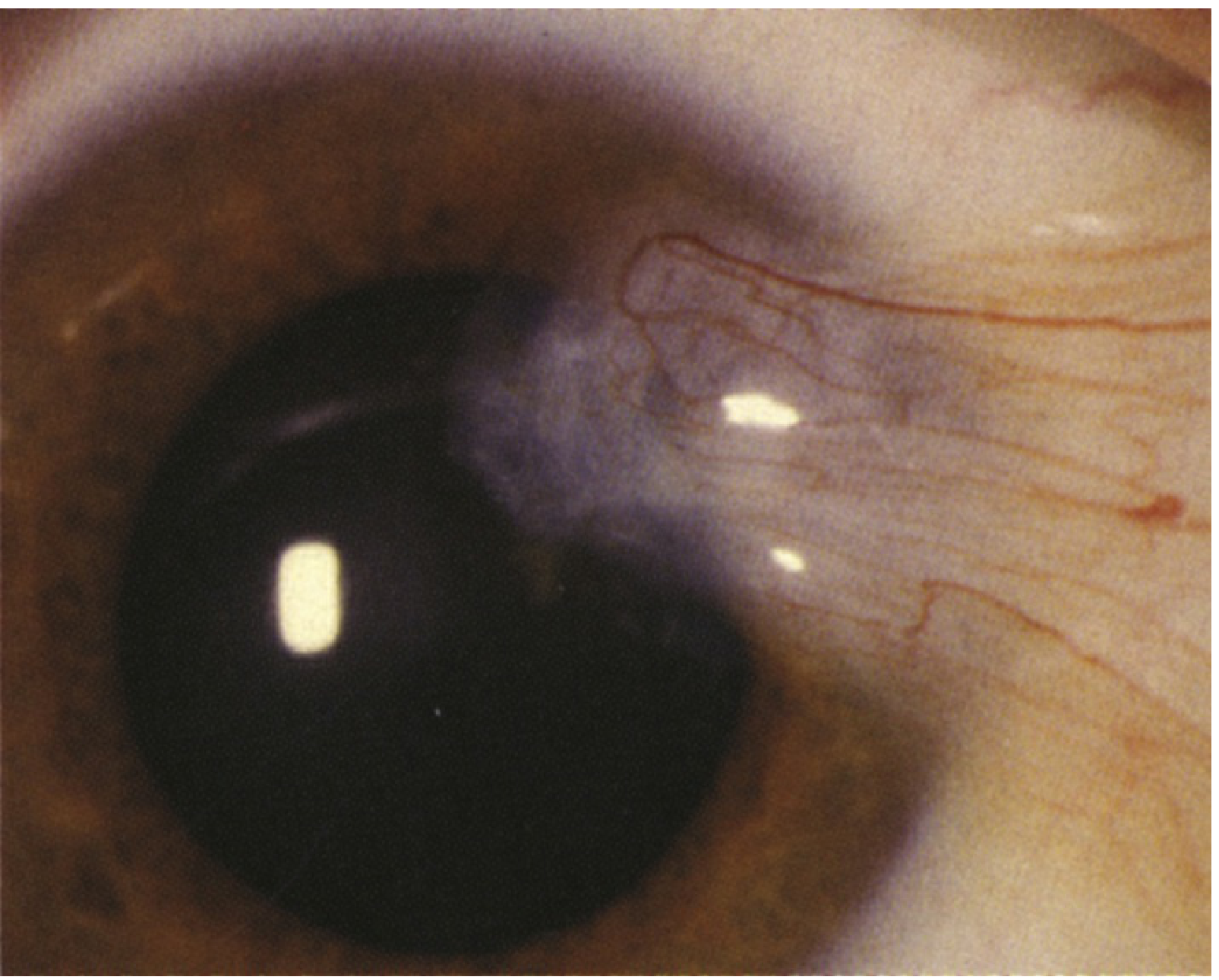
Fig. 4.9.1 - Pterygium (Wills Eye Manual)
Pathophysiology
- Results from elastotic degeneration of deep conjunctival layers, leading to fibrovascular tissue proliferation
- Caused primarily by actinic (UV) damage and chronic irritation - located in the sun-exposed interpalpebral fissure
- Histologically similar to pinguecula: shows elastotic degenerative changes in vascularized subepithelial stromal collagen
- Unlike pinguecula, it invades the Bowman layer of the cornea
- The fibrovascular tissue dissects into the plane normally occupied by Bowman layer
- Tends to run in families; more common in individuals from equatorial regions
Clinical Features
Anatomy of the Lesion
A pterygium has three parts (see Fig. 6.28B below):
- Cap - an avascular halo-like zone at the advancing edge
- Head - the point of corneal invasion
- Body - the fleshy vascularized part on the sclera/conjunctiva
Associated Signs
| Sign | Description |
|---|---|
| Stocker line | Linear epithelial iron deposition in corneal epithelium anterior to the head |
| Fuchs islets | Small discrete whitish flecks of pterygial epithelial cells at the advancing edge |
| Delle | Localized drying/thinning at the advancing edge due to tear film disruption |
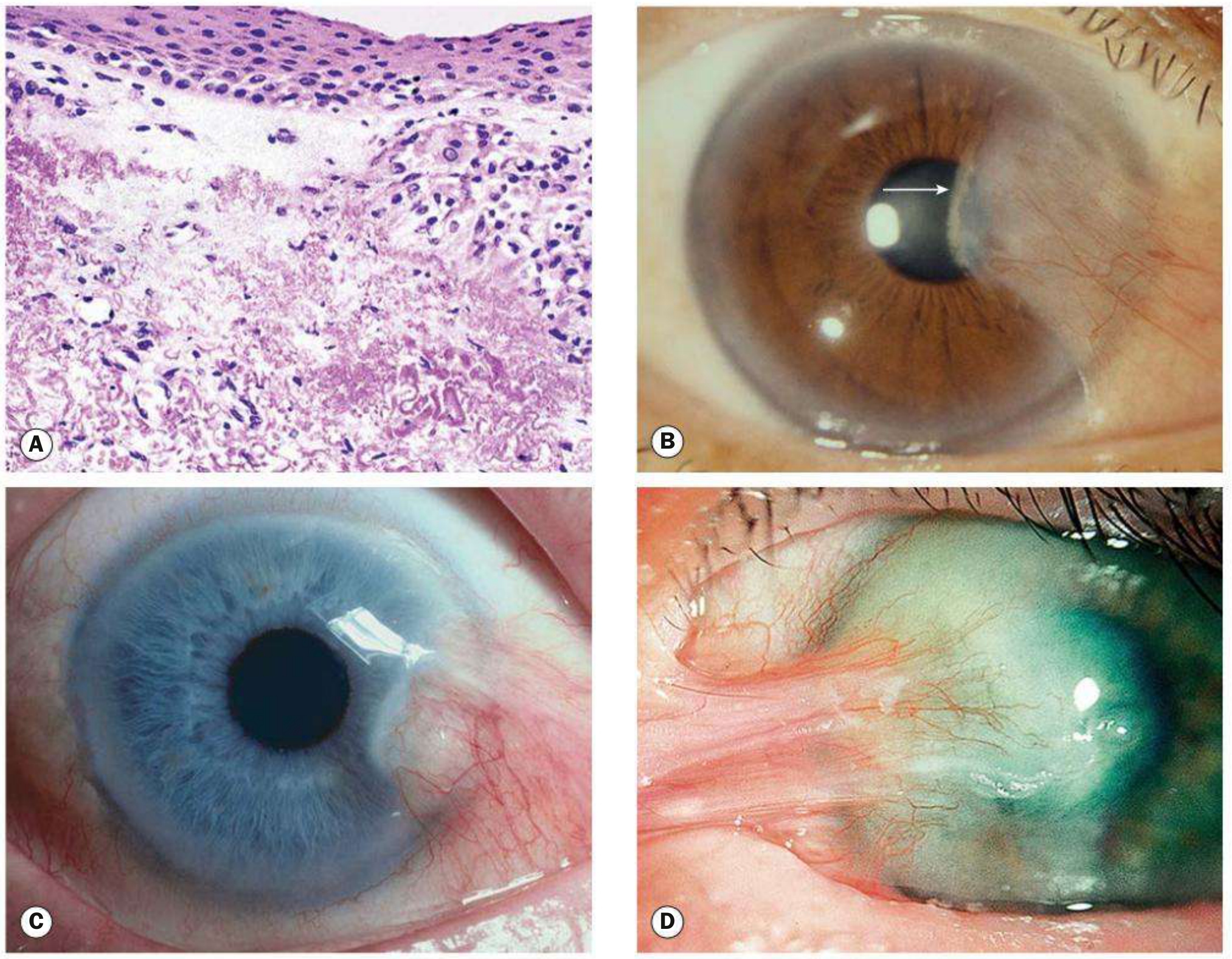
Fig. 6.28 - Pterygium: (A) Histology; (B) classic pterygium with Stocker line (arrow); (C) inflamed pterygium; (D) pseudopterygium from chemical burn (Kanski's Clinical Ophthalmology)
Symptoms
- Most small lesions are asymptomatic
- Irritation and grittiness (from dellen effect at the advancing edge)
- Decreased vision - by obscuring the visual axis or inducing irregular astigmatism
- Cosmetic concern (common reason for seeking treatment)
- Intermittent inflammation (pingueculitis-like episodes)
- Contact lens intolerance due to edge lift
- Extensive or recurrent lesions may cause subconjunctival fibrosis restricting ocular excursion
Location
- Almost always at the 3 or 9 o'clock perilimbal position (interpalpebral fissure)
- Most commonly nasal in location
Differential Diagnosis
| Condition | Key Distinguishing Feature |
|---|---|
| Pinguecula | Yellow-white elevation adjacent to limbus - does NOT invade cornea |
| Pseudopterygium | Conjunctival band adherent to cornea only at apex; associated with prior trauma/burn/ulcer; may be at any clock position |
| Conjunctival intraepithelial neoplasia (CIN) | Papillomatous, jelly-like, or leukoplakic; may not be wing-shaped or in typical 3/9 o'clock location |
| Limbal dermoid | Congenital rounded white lesion, usually inferotemporal |
| Pannus | Vessels only, minimal elevation; associated with contact lens wear, trachoma, rosacea |
Important: Atypical pterygia require biopsy to rule out CIN or ocular surface squamous neoplasia (OSSN). Submitted excised tissue occasionally reveals precursors of squamous cell carcinoma or melanoma.
Distinguishing pseudopterygium: Located away from the horizontal axis; has firm attachment only at its apex (can pass a probe under the body); associated with a prior causative episode (burn, ulcer, trauma).
Workup
- Slit lamp examination to identify the lesion, evaluate corneal integrity and thickness
- Check for corneal astigmatism (often irregular, may be with-the-rule)
- Measure pterygium size and distance from visual axis; repeat every 3-12 months to assess growth rate
- Biopsy for atypical appearances
Treatment
Conservative (Observation + Symptom Control)
- UV protection - UV-blocking sunglasses or goggles (prevention and slowing progression)
- Artificial tears (preservative-free, q.i.d. to q8h) to reduce irritation
- For inflamed pterygium:
- Mild: Artificial tears q.i.d.
- Moderate-severe: Mild topical steroid (fluorometholone 0.1%, loteprednol 0.2-0.5% q.i.d.) or topical NSAID (ketorolac 0.4-0.5% q.i.d.) or topical antihistamine/mast cell stabilizer (bepotastine, olopatadine)
- For delle: Artificial tear ointment q2h
Surgical Indications
Surgery is indicated when:
- Pterygium threatens the visual axis or induces significant astigmatism
- Excessive irritation not relieved by conservative treatment
- Interference with contact lens wear
- Significant cosmetic concern
- Consider removal prior to cataract or refractive surgery
Surgical Techniques
| Technique | Notes |
|---|---|
| Bare sclera excision alone | ~80% recurrence rate - not recommended alone |
| Conjunctival autograft | Gold standard; donor from superior/upper-temporal para-limbal region; secured with 10-0 nylon or fibrin tissue glue (e.g., TISSEEL) - shorter OR time, less postoperative irritation |
| Amniotic membrane graft | Alternative to conjunctival autograft |
| Mitomycin C (MMC) adjuvant | Reduces recurrence; more commonly reserved for recurrent pterygia due to risk of corneoscleral thinning/necrosis |
| Beta-irradiation | Alternative adjuvant to patching techniques |
| Peripheral lamellar keratoplasty | For deep lesions |
Tip: The risk of recurrence is significantly reduced by using a conjunctival autograft or intraoperative mitomycin C application.
Follow-Up
- Asymptomatic, stable: check every 1-2 years
- Measure size every 3-12 months to track progression toward visual axis
- If on topical steroids: check IOP after a few weeks; taper and discontinue once inflammation resolves
Recent Evidence (2025)
A 2025 systematic review and meta-analysis (PMID: 40562088) found that adjuvant topical 0.05% cyclosporine A reduces primary pterygium recurrence rates post-excision, adding to the options alongside MMC. A separate 2025 systematic review (PMID: 40235101) addressed the impact of pterygium on refractive errors, confirming significant irregular astigmatism induction that can be partially reversed by excision.
Sources: Kanski's Clinical Ophthalmology (10th ed.), p. 215-216 | The Wills Eye Manual, p. 191-194 | Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 1207
This is a shared conversation. Sign in to Orris to start your own chat.