Diabetes full details note with type mbbs
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I have very rich content from both Harrison's and Robbins. I now have enough to write a comprehensive MBBS-level note on Diabetes Mellitus. Let me compile the full detailed note.
DIABETES MELLITUS - Full MBBS Notes
Sources: Harrison's Principles of Internal Medicine 22E (2025), Robbins & Cotran Pathologic Basis of Disease
DEFINITION
Diabetes mellitus (DM) is a group of metabolic disorders sharing the common feature of hyperglycemia caused by defects in insulin secretion, insulin action, or both. Chronic hyperglycemia leads to secondary damage in multiple organ systems, especially the kidneys, eyes, nerves, and blood vessels.
- Robbins & Cotran Pathologic Basis of Disease, p. 1014
EPIDEMIOLOGY
- Affects >30 million people (~11% of population) in the USA
- ~1.9 million have Type 1 DM; the rest (~90-95%) have Type 2 DM
- ~96 million US adults have "prediabetes"
- WHO estimates 422 million people worldwide
- 7th leading cause of death in the USA
- Economic burden: ~$327 billion/year (USA)
- Higher prevalence in Native Americans, African Americans, and Hispanics (1.5-2x higher risk)
CLASSIFICATION
Type 1 DM (T1DM)
- Autoimmune destruction of pancreatic beta cells
- Absolute insulin deficiency
- ~5-10% of all diabetes
- Most common in patients <20 years
Type 2 DM (T2DM)
- Combination of peripheral insulin resistance + relative insulin deficiency
- ~90-95% of all diabetes
- Most are overweight/obese (80%)
- Classically "adult-onset" but now increasing in children
Other Specific Types
| Category | Examples |
|---|---|
| MODY (genetic beta-cell defects) | MODY1 (HNF4A), MODY2 (GCK), MODY3 (HNF1A), MODY4 (PDX1), MODY5 (HNF1B), MODY6 (NEUROD1) |
| Genetic defects in insulin action | Type A insulin resistance, lipoatrophic diabetes |
| Exocrine pancreatic disease (Type 3C) | Chronic pancreatitis, pancreatectomy, pancreatic cancer, cystic fibrosis, hemochromatosis |
| Endocrinopathies | Acromegaly, Cushing syndrome, Conn syndrome |
| Drug-induced | Glucocorticoids, thiazides, nicotinic acid, interferon-α, phenytoin, beta-adrenergic agonists |
| Infections | Congenital rubella, CMV |
| Genetic syndromes | Down syndrome, Klinefelter syndrome, Turner syndrome, Prader-Willi |
| Gestational DM (GDM) | Onset or first recognition during pregnancy |
DIAGNOSTIC CRITERIA (ADA / WHO)
Normal blood glucose: 70-120 mg/dL
Diabetes is diagnosed by ANY ONE of the following (confirmed on a repeat test, except #2):
| Test | Diabetes | Prediabetes |
|---|---|---|
| Fasting plasma glucose (FPG) | ≥126 mg/dL | 100-125 mg/dL (IFG) |
| Random plasma glucose | ≥200 mg/dL + symptoms | - |
| 2-hr OGTT (75g load) | ≥200 mg/dL | 140-199 mg/dL (IGT) |
| HbA1c | ≥6.5% | 5.7-6.4% |
- Repeat confirmation required for all except a symptomatic random glucose ≥200
- Acute illness (burns, trauma, infection) can cause transient hyperglycemia - diagnosis requires persistence after resolution
- Robbins & Cotran, p. 1015
COMPARATIVE FEATURES: T1DM vs T2DM
| Feature | Type 1 DM | Type 2 DM |
|---|---|---|
| Onset | Usually childhood/adolescence | Usually adult; increasing in children |
| Body weight | Normal or weight loss | 80% obese |
| Insulin levels | Progressive decrease (absolute deficiency) | High early; normal/low late |
| Autoantibodies | Anti-GAD65, anti-IA2, anti-ZnT8 | None |
| Acute complication | Diabetic ketoacidosis (DKA) | Hyperosmolar hyperglycemic state (HHS) |
| HLA linkage | MHC class II (HLA-DR3, DR4) | No HLA linkage |
| Key genes | CTLA4, PTPN22, insulin VNTR | TCF7L2, PPARG, FTO |
| Pathogenesis | Autoimmune T-cell destruction of beta cells | Insulin resistance + beta-cell failure |
| Islet pathology | Insulitis (T-cell + macrophage infiltrate), beta-cell depletion | Amyloid deposition, mild beta-cell depletion |
PATHOGENESIS
Pancreatic Islet Cell Anatomy
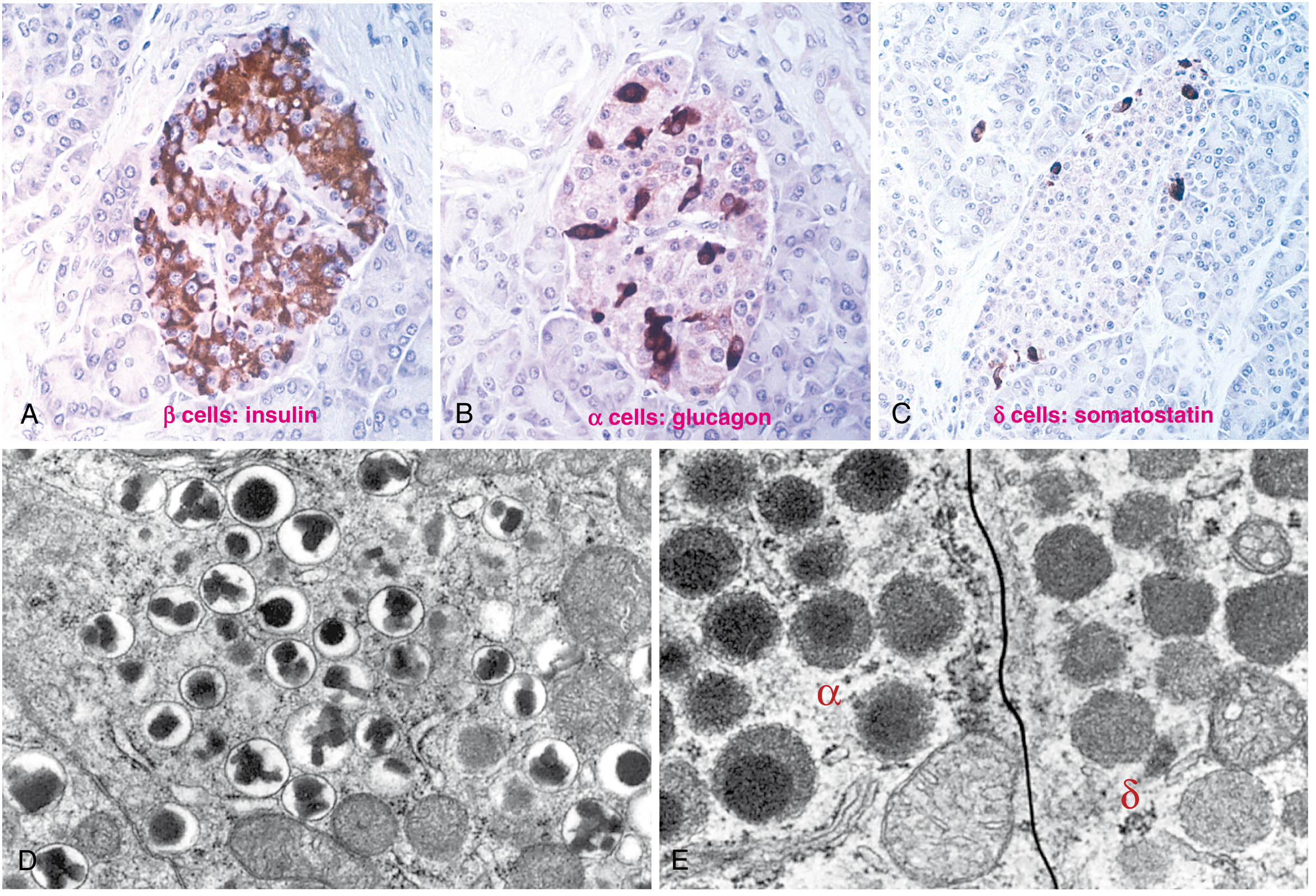
Fig. Hormone production in pancreatic islet cells - Robbins & Cotran, p. 1014
Glucose Homeostasis
- Glucose maintained 70-120 mg/dL by 3 processes:
- Hepatic glucose production (gluconeogenesis, glycogenolysis)
- Peripheral glucose utilization (primarily skeletal muscle)
- Insulin and counterregulatory hormones (glucagon, cortisol, catecholamines)
- Fasting state: low insulin + high glucagon → hepatic glucose output
- Fed state: insulin rises, glucagon falls → glucose uptake in muscle, liver, adipose
Insulin Synthesis and Release
- Produced in beta cells as preproinsulin → cleavage to proinsulin → insulin + C-peptide
- C-peptide has no known metabolic function but is useful as a marker of endogenous insulin secretion
- Glucose is the primary stimulus for insulin secretion (via GLUT-2 uptake, glucokinase phosphorylation, ATP generation, KATP channel closure, membrane depolarization, Ca2+ influx)
- Other stimuli: GLP-1, GIP (incretins), amino acids, parasympathetic stimulation
Type 1 DM Pathogenesis
- Genetic susceptibility: HLA-DR3/DR4, HLA-DQ polymorphisms (strongest risk); CTLA4, PTPN22, insulin gene VNTR
- Environmental trigger: viral infection (Coxsackie B, mumps, rubella), dietary factors, gut microbiome
- Breakdown of self-tolerance: autoreactive CD4+ and CD8+ T cells attack beta cells
- Insulitis: inflammatory infiltrate (T cells and macrophages) in islets
- Progressive beta-cell destruction → absolute insulin deficiency
- Key autoantibodies (markers, not necessarily pathogenic): anti-GAD65, anti-IA2, anti-ZnT8, anti-insulin antibodies
- Insulitis is present for years before clinical onset; ~80-90% beta-cell loss before symptoms appear
Type 2 DM Pathogenesis
- Genetic factors: polygenic (TCF7L2, FTO, PPARG); strong family history
- Environmental factors: obesity (especially visceral), sedentary lifestyle, caloric excess
- Insulin resistance: decreased sensitivity of muscle, liver, and adipose to insulin
- Visceral fat releases free fatty acids and adipokines → impair insulin signaling
- Mechanism: serine phosphorylation of IRS-1 by activated kinases (IKK-β, JNK) → blocks PI3K-Akt pathway
- Compensatory hyperinsulinemia: beta cells increase insulin output initially
- Beta-cell failure: progressive decline in beta-cell mass and function; amyloid (IAPP - islet amyloid polypeptide) deposits in islets
- Relative insulin deficiency despite initially elevated insulin levels
INSULIN PREPARATIONS
| Preparation | Onset | Peak | Duration |
|---|---|---|---|
| Rapid-acting (Aspart, Glulisine, Lispro) | <0.25 h | 0.5-1.5 h | 3-5 h |
| Short-acting (Regular) | 0.5-1 h | 2-3 h | 4-8 h |
| Inhaled insulin | <0.25 h | 1-2 h | 3 h |
| Intermediate (NPH) | 2-4 h | 4-10 h | 10-16 h |
| Long-acting (Glargine, Detemir) | 1-4 h | Flat/no peak | 20-24 h |
| Ultra-long (Degludec) | 1-9 h | No peak | >42 h |
- Harrison's 22E, p. 3263
MANAGEMENT
General Goals
- HbA1c target: <7% for most patients; individualize based on age, comorbidities
- Blood pressure: <130/80 mmHg
- LDL: <100 mg/dL (or <70 mg/dL if CVD present)
- Lifestyle: diet, exercise, weight loss
Type 1 DM Management
- Insulin is mandatory (absolute deficiency)
- Basal-bolus regimen: long-acting (basal) + rapid-acting with meals (bolus)
- Intensive management: multiple daily injections (MDI), CSII (insulin pump), sensor-augmented systems, Automated Insulin Delivery (AID) with CGM
- Goals: prevent DKA, maintain near-normal glycemia
Type 2 DM - Oral & Injectable Agents
| Drug Class | Mechanism | Key Example | Notes |
|---|---|---|---|
| Biguanides | Inhibit hepatic gluconeogenesis, improve insulin sensitivity | Metformin | First-line; avoid if eGFR <30 |
| Sulfonylureas | Stimulate insulin secretion (KATP channel) | Glipizide, Glyburide | Risk of hypoglycemia |
| SGLT-2 inhibitors | Block renal glucose reabsorption | Empagliflozin, Dapagliflozin | Cardioprotective, nephroprotective |
| GLP-1 agonists | Increase incretin effect, decrease glucagon | Semaglutide, Liraglutide | Weight loss, CV benefit |
| DPP-4 inhibitors | Prevent incretin degradation | Sitagliptin | Weight neutral |
| Thiazolidinediones | PPAR-γ agonist, improve insulin sensitivity | Pioglitazone | Risk of fluid retention, fractures |
| Alpha-glucosidase inhibitors | Delay carbohydrate absorption | Acarbose | GI side effects |
| Meglitinides | Short-acting insulin secretagogues | Repaglinide | Taken with meals |
COMPLICATIONS
MICROVASCULAR (Diabetes-specific)
1. Diabetic Nephropathy (Diabetic Kidney Disease)
- Leading cause of end-stage renal disease (ESRD) in the developed world
- Mechanism: hyperfiltration → glomerular hypertension → mesangial expansion → GBM thickening → proteinuria
- Nodular glomerulosclerosis (Kimmelstiel-Wilson lesion): pathognomonic
- Stages: microalbuminuria (30-300 mg/day) → macroalbuminuria → declining GFR → ESRD
- Management: ACE inhibitors/ARBs (first-line), SGLT-2 inhibitors, glycemic and BP control
2. Diabetic Retinopathy
- Most common cause of new-onset blindness in working-age adults
- Non-proliferative (NPDR): microaneurysms, hard exudates, cotton-wool spots, intraretinal hemorrhages
- Proliferative (PDR): neovascularization (new vessel formation) → vitreous hemorrhage, retinal detachment
- Diabetic macular edema (DME): can occur at any stage
- Screening: annual dilated fundoscopy; treatment: laser photocoagulation, anti-VEGF injections
3. Diabetic Neuropathy
- Most common complication overall
- Distal symmetric polyneuropathy: most common; "glove and stocking" sensory loss; loss of vibration/position sense; painful neuropathy; risk of foot ulcers
- Mononeuropathy: CN III most common (pupil-sparing; diabetic CN III palsy)
- Autonomic neuropathy: gastroparesis, diabetic diarrhea, urinary retention, erectile dysfunction, orthostatic hypotension, hypoglycemia unawareness, Charcot foot
MACROVASCULAR (Atherosclerotic Cardiovascular Disease)
- 2-4x higher risk of coronary artery disease (CAD), stroke, and peripheral arterial disease (PAD)
- ASCVD may precede hyperglycemia in T2DM
- Dyslipidemia (high TG, low HDL, small dense LDL), hypertension, and hyperglycemia all contribute
- Heart failure risk is significantly increased
- Management: statins, ACE inhibitors, SGLT-2 inhibitors (heart failure benefit), aspirin in high-risk patients
ACUTE COMPLICATIONS
Diabetic Ketoacidosis (DKA)
- Mainly in T1DM (occasionally T2DM)
- Precipitants: infections, missed insulin, new diagnosis
- Mechanism: absolute insulin deficiency → lipolysis → excess free fatty acids → ketogenesis → ketonemia + metabolic acidosis
- Features: polyuria, polydipsia, Kussmaul breathing, fruity breath, vomiting, abdominal pain, altered consciousness
- Diagnosis: Blood glucose >250 mg/dL + ketones + pH <7.3 + bicarbonate <15 mEq/L
- Management: IV fluids (normal saline), insulin infusion, potassium replacement, treat precipitant
Hyperosmolar Hyperglycemic State (HHS)
- Mainly in T2DM; older patients
- Extreme hyperglycemia (>600 mg/dL) without significant ketosis
- Serum osmolality >320 mOsm/kg
- Profound dehydration, neurological changes
- Mortality higher than DKA
- Management: aggressive IV fluid replacement, insulin, electrolyte correction
Hypoglycemia
- Blood glucose <70 mg/dL
- Caused by excess insulin, missed meals, exercise
- Adrenergic symptoms: sweating, tremor, palpitations, anxiety
- Neuroglycopenic symptoms: confusion, seizures, coma
- Treatment: 15g fast-acting carbohydrate; IV dextrose or glucagon injection if severe
- Hypoglycemia unawareness: loss of warning symptoms with repeated episodes (autonomic neuropathy)
OTHER COMPLICATIONS
| Complication | Details |
|---|---|
| Diabetic foot | Combination of neuropathy + peripheral vascular disease → ulcers, infections, osteomyelitis, Charcot arthropathy |
| Infections | Increased susceptibility; candidiasis (oral, genital), UTIs, necrotizing fasciitis, mucormycosis (rhinocerebral), malignant otitis externa (Pseudomonas) |
| Cataracts | Osmotic lens changes; earlier onset |
| Glaucoma | Neovascular glaucoma due to retinal ischemia |
| Gastroparesis | Autonomic neuropathy; delayed gastric emptying; nausea, early satiety |
| Cheiroarthropathy | Thickened skin, reduced joint mobility ("prayer sign") |
| Dermatological | Necrobiosis lipoidica, acanthosis nigricans, diabetic dermopathy |
| Metabolic bone disease | Osteoporosis; increased fracture risk |
| Cognitive impairment | 2-4x increased risk of Alzheimer's |
| Depression | Bidirectional association |
| MAFLD/NASH | Metabolic associated fatty liver disease |
GESTATIONAL DIABETES MELLITUS (GDM)
- Defined as any degree of glucose intolerance first recognized during pregnancy
- Affects 6-7% of pregnancies
- Mechanism: placental hormones (hPL, progesterone, cortisol) cause insulin resistance
- Screening: 24-28 weeks gestation (50g GCT; if positive → 100g OGTT)
- Risk to fetus: macrosomia, birth trauma, neonatal hypoglycemia, stillbirth, respiratory distress
- Risk to mother: 50% risk of developing T2DM within 10 years
- Management: diet + exercise first; insulin if targets not met (metformin and glyburide may be used but cross placenta)
MONITORING
| Parameter | Target / Method |
|---|---|
| HbA1c | Reflects average glucose over 3 months; target <7% |
| Self-monitoring blood glucose (SMBG) | Fasting <100 mg/dL; postprandial <140 mg/dL (2-hr) |
| Continuous Glucose Monitoring (CGM) | Real-time glucose; "time in range" (70-180 mg/dL) >70% |
| Urine albumin:creatinine ratio | Annually; early nephropathy detection |
| Lipid profile | Annually |
| Foot examination | Each visit |
| Ophthalmology | Annually (T1DM: 5 years after diagnosis; T2DM: at diagnosis) |
| Blood pressure | Each visit |
PREVENTION
Type 1 DM
- No established prevention; trials with immunosuppression are ongoing
Type 2 DM (Diabetes Prevention Program)
- Lifestyle modification (7% weight loss + 150 min/week exercise): reduced incidence by 58%
- Metformin: reduced incidence by 31%
- GLP-1 agonists, bariatric surgery also highly effective
HIGH-YIELD POINTS FOR EXAMS
| Point | Detail |
|---|---|
| Diagnostic FPG cutoff | ≥126 mg/dL |
| Prediabetes HbA1c range | 5.7-6.4% |
| T1DM autoantibodies | Anti-GAD65 (most common), anti-IA2, anti-ZnT8 |
| T1DM HLA association | HLA-DR3 and HLA-DR4 (class II MHC) |
| T2DM islet pathology | Amyloid (IAPP) deposition |
| T1DM islet pathology | Insulitis (T lymphocyte infiltrate) |
| Diabetic nephropathy hallmark | Kimmelstiel-Wilson nodular glomerulosclerosis |
| Diabetic retinopathy hallmark | Microaneurysms (earliest lesion) |
| Fastest-acting insulin | Lispro/Aspart/Glulisine (<15 min onset) |
| First-line T2DM drug | Metformin |
| DKA vs HHS | DKA = T1DM, ketones, acidosis; HHS = T2DM, extreme hyperglycemia, no ketones |
| GDM screening timing | 24-28 weeks gestation |
| C-peptide clinical use | Distinguishes T1DM (low/absent) from T2DM (normal/high) |
| Charcot foot | Neuropathic arthropathy; warm, swollen, insensate foot |
| Diabetic CN III palsy | Pupil-SPARING (vs posterior communicating artery aneurysm = pupil-involving) |
| SGLT-2 inhibitors benefit | Renal protection + heart failure reduction |
References: Harrison's Principles of Internal Medicine 22E (2025); Robbins & Cotran Pathologic Basis of Disease, Chapter 24
This is a shared conversation. Sign in to Orris to start your own chat.