Bacterial graph curve
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching the Web
bacterial growth curve four phases lag log stationary death microbiology
Reading File
Loading Image
Loading Image
Here is a complete breakdown of the Bacterial Growth Curve, sourced directly from Medical Microbiology 9e.
Bacterial Growth Curve
The growth curve plots log bacterial number (y-axis) against time (x-axis) in a closed (batch) culture. It has four sequential phases:
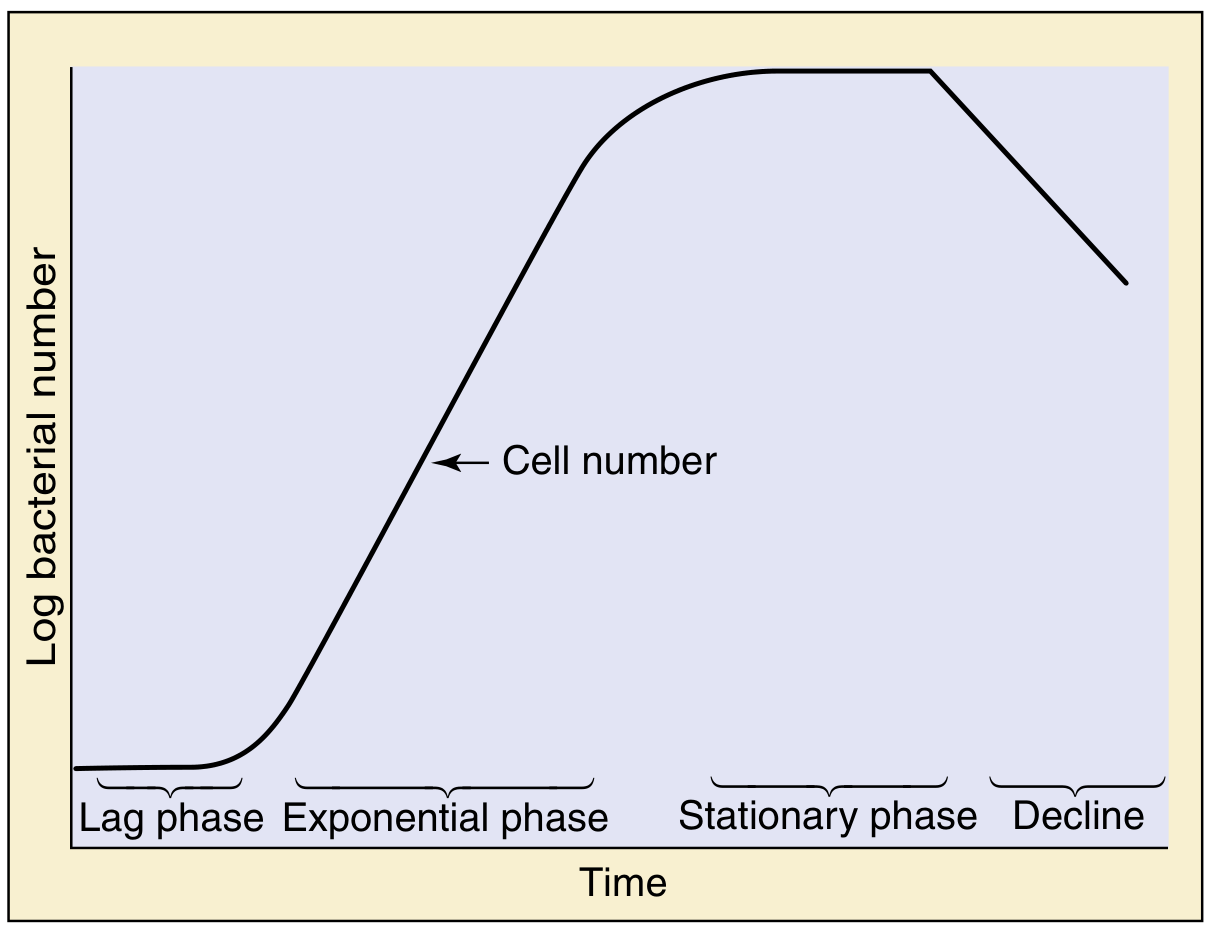
Fig. 13.9 - Phases of bacterial growth, starting with an inoculum of stationary-phase cells. (Medical Microbiology 9e)
1. Lag Phase
- Bacteria are added to a new medium and require time to adapt before dividing.
- No significant increase in cell number occurs.
- Cells are metabolically active - synthesizing enzymes, ribosomes, and other machinery needed for growth.
- Duration depends on the age of the inoculum and how different the new environment is from the original.
2. Exponential (Log) Phase
- Bacteria divide at a constant, characteristic doubling time determined by strain and environmental conditions.
- Cell number increases as 2^n, where n = number of generations (doublings).
- This is the phase of most rapid, predictable growth.
- Cells are most uniform in size, metabolic activity, and biochemical composition.
- Bacteria are most sensitive to antibiotics (especially cell-wall active agents like beta-lactams) during this phase, since they are actively dividing.
3. Stationary Phase
- The culture runs out of nutrients, or toxic metabolic byproducts accumulate in the medium.
- The rate of cell division equals the rate of cell death - net cell count plateaus.
- Cells begin to show stress responses: DNA may be cannibalized for deoxyribonucleotide precursors, peptidoglycan and proteins are degraded for metabolites, and cells shrink.
- In some species, signals here initiate sporulation.
- Some organisms promote uptake of foreign DNA (transformation) as a survival strategy.
4. Decline (Death) Phase
- Cell death exceeds cell division; viable count falls.
- Some bacteria stop dividing but remain viable (persisters) - these are often insensitive to antibiotics, which is clinically important for chronic or relapsing infections.
- Cell lysis, loss of structural integrity, and final population collapse occur.
Key Clinical Relevance
| Phase | Antibiotic Sensitivity | Notes |
|---|---|---|
| Lag | Low | Cells not dividing |
| Exponential | Highest | Best target for beta-lactams, aminoglycosides |
| Stationary | Low | Nutrient-starved, stress responses active |
| Decline | Very low | Persisters resist antibiotics - source of relapse |
- Generation time (doubling time) varies widely: E. coli ~20 min, Mycobacterium tuberculosis ~18-24 hours - which is why TB treatment takes months.
- The curve is generated from batch (closed) culture - in continuous culture (chemostat), bacteria can be maintained indefinitely in log phase by constantly adding nutrients and removing waste.
Source: Medical Microbiology 9e, "Population Dynamics," p. 160
Microbiology question in general Microbiology for bpt student
Asking for Preferences
All
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Here is a comprehensive set of General Microbiology Questions and Answers for BPT Students, covering all major topics:
🦠 General Microbiology - BPT Question Bank
SECTION 1: Bacterial Structure & Classification
Q1. What are the four basic shapes of bacteria?
A.
| Shape | Term | Example |
|---|---|---|
| Spherical | Coccus | Staphylococcus, Streptococcus |
| Rod-shaped | Bacillus | E. coli, Clostridium |
| Spiral/curved | Spirillum / Vibrio | Vibrio cholerae, Treponema |
| Comma-shaped | Vibrio | Vibrio cholerae |
Q2. What is the difference between Gram-positive and Gram-negative bacteria?
A.
| Feature | Gram-Positive | Gram-Negative |
|---|---|---|
| Cell wall peptidoglycan | Thick (multilayer) | Thin (single layer) |
| Outer membrane | Absent | Present |
| Lipopolysaccharide (LPS/endotoxin) | Absent | Present |
| Color after Gram stain | Purple/Violet | Pink/Red |
| Periplasmic space | Absent/narrow | Present |
| Examples | Staph, Strep, Bacillus | E. coli, Pseudomonas, Salmonella |
- Medical Microbiology 9e, "Bacterial Structure"
Q3. What is peptidoglycan and why is it medically important?
A. Peptidoglycan (murein) is the rigid structural layer of the bacterial cell wall. It:
- Maintains cell shape and prevents osmotic lysis
- Is the target of beta-lactam antibiotics (penicillin, cephalosporins) which inhibit its cross-linking
- Is thicker in Gram-positive bacteria
- Is absent in human cells - making it an ideal antibiotic target
Q4. Name the structures found ONLY in bacteria (not in human cells).
A.
- Cell wall (peptidoglycan)
- 70S ribosomes (human cells have 80S)
- Pili (fimbriae)
- Flagella with unique basal body structure
- Plasmids
- Endospores (in some species)
- Capsule (in some species)
Q5. What is the function of the bacterial capsule?
A. The capsule:
- Protects bacteria from phagocytosis (main virulence factor)
- Helps in adherence to host tissues and surfaces
- Protects against desiccation
- Detected by the Quellung reaction (capsular swelling with specific antibody)
- Examples of encapsulated bacteria: Streptococcus pneumoniae, Klebsiella, Haemophilus influenzae, Neisseria meningitidis
Q6. What are endospores? Which bacteria produce them?
A. Endospores are dormant, highly resistant survival structures formed under adverse conditions (nutrient depletion).
- One cell forms one spore (sporulation), and the spore is liberated when the mother cell undergoes autolysis
- Can survive for centuries, resistant to heat, drying, radiation, and many chemicals
- All medically important spore-formers are Gram-positive rods
- Examples: Clostridium tetani (tetanus), C. botulinum (botulism), C. difficile (pseudomembranous colitis), Bacillus anthracis (anthrax)
- Autoclave at 121°C for 15 min is required to destroy spores
SECTION 2: Staining Techniques
Q7. Describe the steps of the Gram Stain.
A.
| Step | Reagent | Gram+ result | Gram- result |
|---|---|---|---|
| 1 | Crystal violet (primary stain) | Purple | Purple |
| 2 | Gram's iodine (mordant) | Purple-black | Purple-black |
| 3 | Alcohol/acetone (decolorizer) | Retains purple | Decolorized |
| 4 | Safranin (counterstain) | Purple | Pink/Red |
Mechanism: Gram-positive cells have a thick peptidoglycan wall that traps the crystal violet-iodine complex on decolorization. Gram-negative cells lose it due to dissolution of the thin lipid-containing outer membrane.
Q8. What is the Ziehl-Neelsen (ZN) stain used for?
A. ZN stain (acid-fast stain) is used for Mycobacteria (TB, leprosy) and Nocardia.
- Primary stain: Carbol fuchsin (red) - requires heat to penetrate the waxy mycolic acid wall
- Decolorizer: Acid-alcohol
- Counterstain: Methylene blue
- Result: Acid-fast organisms stain red/pink (AFB+), others stain blue
SECTION 3: Sterilization & Disinfection
Q9. Define and distinguish: Sterilization, Disinfection, Antisepsis, Asepsis.
A.
| Term | Definition | Kills spores? |
|---|---|---|
| Sterilization | Complete destruction of ALL microorganisms including spores | Yes |
| Disinfection | Destruction of most pathogens (not necessarily spores) | No |
| Antisepsis | Disinfection applied to living tissue (skin, mucous membranes) | No |
| Asepsis | Prevention of microbial contamination (technique) | N/A |
| Bactericidal | Kills bacteria | - |
| Bacteriostatic | Inhibits bacterial growth (doesn't kill) | - |
Q10. What are the methods of sterilization?
A.
Physical Methods:
| Method | Temp/Details | Use |
|---|---|---|
| Autoclave (moist heat) | 121°C, 15 min, 15 psi | Most reliable; kills spores |
| Dry heat (hot air oven) | 160°C, 60 min | Glassware, oils, powders |
| Boiling | 100°C, 20 min | Does NOT kill spores |
| Pasteurization | 72°C, 15 sec (HTST) | Milk; kills pathogens, not spores |
| UV radiation | 260 nm | Air, surfaces |
| Ionizing radiation (gamma) | - | Disposable syringes |
| Filtration | 0.22 µm membrane | Heat-sensitive liquids (sera, vaccines) |
Chemical Methods:
- Ethylene oxide - heat-sensitive instruments
- Formaldehyde, glutaraldehyde - endoscopes
- Chlorine, hypochlorite - water, surfaces
Key point for BPT: Autoclave is the gold standard for sterilizing surgical instruments and physiotherapy equipment.
SECTION 4: Bacterial Growth & Reproduction
Q11. What are the four phases of the bacterial growth curve?
A.
| Phase | What happens |
|---|---|
| Lag | Adaptation period; no increase in cell number |
| Log (Exponential) | Rapid division; cells double every generation (2^n); most antibiotic-sensitive phase |
| Stationary | Nutrients depleted/toxins accumulate; birth rate = death rate |
| Decline (Death) | Death > division; persister cells may remain antibiotic-resistant |
Q12. What is binary fission?
A. Binary fission is the asexual reproduction method of bacteria:
- DNA replicates
- Cell wall and membrane extend
- Septum forms in the middle
- Cell divides into two identical daughter cells
- E. coli doubles every ~20 minutes; M. tuberculosis every ~18-24 hours (explains why TB treatment takes months).
SECTION 5: Infection & Immunity
Q13. What is the difference between innate and adaptive immunity?
A.
| Feature | Innate Immunity | Adaptive Immunity |
|---|---|---|
| Speed | Immediate (minutes-hours) | Slow (days-weeks) |
| Specificity | Non-specific | Highly specific |
| Memory | No | Yes (key feature) |
| Components | Skin, neutrophils, macrophages, NK cells, complement | T cells, B cells, antibodies |
| Response to 2nd exposure | Same | Faster and stronger (memory) |
Q14. What are the five classes of immunoglobulins (antibodies)?
A.
| Class | Key Feature |
|---|---|
| IgG | Most abundant; crosses placenta; secondary response |
| IgM | First antibody produced (primary response); pentamer |
| IgA | Found in secretions (saliva, breast milk, tears, mucosa) |
| IgE | Involved in allergy and parasitic infections |
| IgD | B cell surface receptor; function less clear |
Q15. What is the chain of infection?
A. Six essential links:
- Infectious agent (pathogen)
- Reservoir (human, animal, environment)
- Portal of exit (respiratory tract, blood, feces)
- Mode of transmission (droplet, contact, airborne, vector, fecal-oral)
- Portal of entry (skin, respiratory, GI, urogenital)
- Susceptible host
Breaking any link prevents infection - critical concept for physiotherapists in infection control.
SECTION 6: Viruses, Fungi & Parasites (Brief)
Q16. How do viruses differ from bacteria?
A.
| Feature | Bacteria | Virus |
|---|---|---|
| Cell structure | Prokaryotic cell | Not a cell (acellular) |
| Nucleic acid | Both DNA & RNA | Either DNA or RNA |
| Ribosomes | Yes (70S) | No |
| Reproduction | Binary fission | Replication inside host cell |
| Antibiotic sensitivity | Yes (most) | No |
| Size | 1-10 µm | 20-300 nm (smaller) |
Q17. What is MRSA? Why is it important in physiotherapy settings?
A. MRSA = Methicillin-Resistant Staphylococcus aureus
- Resistant to all beta-lactam antibiotics due to altered penicillin-binding protein (PBP2a)
- Spreads via direct contact and contaminated surfaces/equipment
- BPT relevance: Physiotherapy equipment (mats, ultrasound probes, hydrotherapy pools), close patient contact, and hospital wards are common transmission sites
- Prevention: Hand hygiene, gloves, surface disinfection, isolating infected patients
SECTION 7: Hospital-Acquired Infections (HAI) - High Yield for BPT
Q18. What is a nosocomial (hospital-acquired) infection?
A. An infection acquired in a healthcare setting, not present at the time of admission (develops after 48 hours of hospitalization).
- Common sites: UTI (most common), pneumonia, surgical site, bloodstream
- Common pathogens: E. coli, Klebsiella, Pseudomonas, Staph aureus, Candida
- BPT students must know: Physiotherapists are at risk of transmitting HAIs through hands, equipment, and close contact. Hand washing (WHO 5 moments) is the single most effective prevention.
Q19. What is the significance of biofilm in microbiology?
A. Biofilms are communities of bacteria adhering to surfaces, enclosed in a self-secreted polysaccharide matrix.
- Up to 1000x more resistant to antibiotics than planktonic (free-floating) bacteria
- Form on medical devices: catheters, prosthetic joints, endoscopes
- Highly relevant in chronic wound infections - a major physiotherapy concern
- Examples: Pseudomonas aeruginosa in chronic lung infections, dental plaque (Streptococcus mutans)
QUICK REVISION TABLE - One-Liners
| Topic | Key Fact |
|---|---|
| Smallest bacteria | Mycoplasma (no cell wall) |
| Largest bacteria | Thiomargarita |
| Obligate intracellular | Chlamydia, Rickettsia, viruses |
| Commonest cause of UTI | E. coli |
| Spore-forming anaerobe | Clostridium |
| Atypical pneumonia | Mycoplasma pneumoniae |
| Gram stain inventor | Hans Christian Gram (1884) |
| Autoclave temperature | 121°C, 15 psi, 15 min |
| Primary antibody response | IgM first, then IgG |
| Rabies virus shape | Bullet-shaped (rhabdovirus) |
Sources: Medical Microbiology 9e; Jawetz, Melnick & Adelberg's Medical Microbiology 28e; Sherris & Ryan's Medical Microbiology 8e
Tip for BPT exams: Focus especially on infection control (sterilization, HAIs, chain of infection) and common pathogens in wound/respiratory infections, as these are most clinically relevant for physiotherapy practice. Would you like detailed questions on any specific topic?
This is a shared conversation. Sign in to Orris to start your own chat.