Cell physiology in detail from basics to clinical
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Here is the complete, detailed guide to cell physiology - from fundamental building blocks to clinical relevance.
Cell Physiology: From Basics to Clinical Application
1. The Cell: Overview and Structural Organization
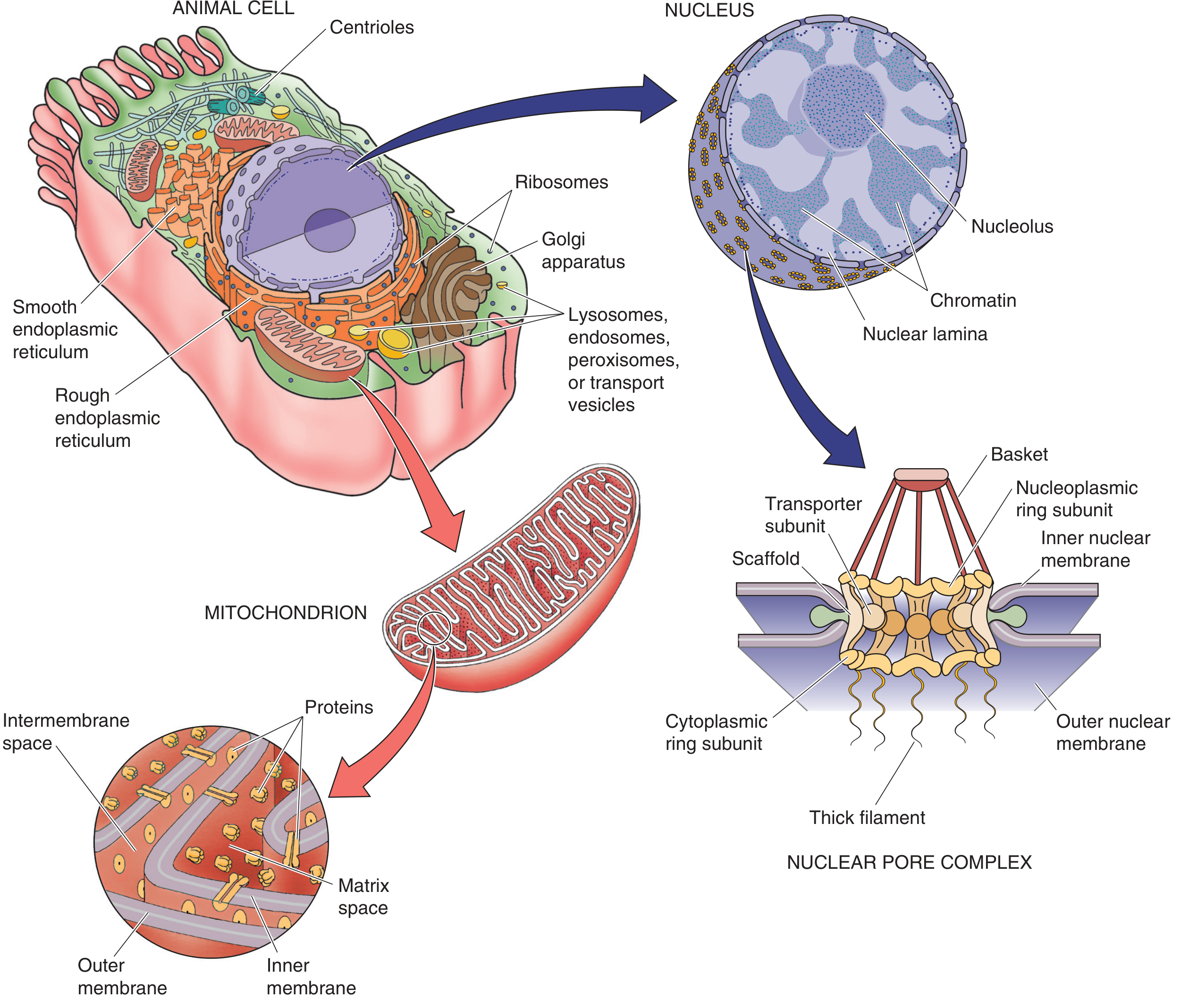
A eukaryotic cell is not a bag of enzymes in water - it is a highly compartmentalized structure where each membrane-enclosed organelle performs distinct functions. Under light microscopy the interior appears grainy; under electron microscopy a remarkable complexity emerges.
2. Organelles and Their Functions
Nucleus
- Largest organelle (2-20 µm diameter); stores, replicates, and reads genetic information
- Bounded by double nuclear membrane with nuclear pore complexes (NPC) - each NPC is ~120 nm and controls selective import/export of RNA, proteins, and ions
- Contains chromatin (DNA + histone proteins) and the nucleolus (site of rRNA synthesis and ribosome assembly)
- The nuclear lamina (intermediate filaments) provides structural scaffolding - mutation in lamin A/C causes Hutchinson-Gilford progeria and several cardiomyopathies (laminopathies)
Endoplasmic Reticulum (ER)
- Rough ER: studded with ribosomes; site of synthesis of secretory, membrane, and lysosomal proteins; adds N-linked glycans
- Smooth ER: lipid synthesis, steroid hormone production, drug detoxification (cytochrome P450 enzymes), and calcium storage
- The ER lumen is a major Ca²⁺ reservoir - a Ca²⁺-ATPase (SERCA pump) actively sequesters Ca²⁺ from cytoplasm into ER lumen. This stored Ca²⁺ is released in response to IP₃ and plays a major role in intracellular signaling
- Clinical: In heart failure, downregulation of SERCA2a reduces SR Ca²⁺ loading, impairing contractile force. Gene therapy targeting SERCA2a has been an area of investigation
Golgi Complex
- Stack of flattened saccules (cisternae) - functions as the cell's "post office"
- Processes, sorts, and targets newly synthesized proteins to their correct subcellular destinations (plasma membrane, lysosomes, secretion)
- Adds O-linked glycans and processes N-linked glycans further
- Clinical: I-cell disease (mucolipidosis II) - lysosomal enzymes are misrouted to the extracellular space instead of lysosomes, causing lysosomal storage
Mitochondrion
- "Balloon within a balloon" - outer membrane and inner membrane create two compartments: intermembrane space and matrix
- Inner membrane is thrown into folds called cristae, dramatically increasing surface area for oxidative phosphorylation
- Site of: Krebs (TCA) cycle, beta-oxidation of fatty acids, electron transport chain, ATP synthesis
- Contains its own DNA (mtDNA) - maternally inherited; encodes 13 proteins, 22 tRNAs, 2 rRNAs
- Produces ~36 ATP per glucose molecule (vs. only 2 by glycolysis)
- Clinical: Mitochondrial diseases (MELAS, MERRF, Leber hereditary optic neuropathy) arise from mtDNA mutations; tissues with highest energy demand (CNS, muscle, heart) are most affected. Metformin acts in part by inhibiting mitochondrial Complex I
Lysosomes
- Membrane-enclosed bags of ~50 hydrolytic enzymes (acid hydrolases) that function at pH ~5
- The vacuolar H⁺-ATPase acidifies the lysosomal lumen
- Digest macromolecules via: endocytosis (receptor-mediated, phagocytosis, pinocytosis), autophagy
- Clinical: Lysosomal storage diseases - Gaucher's (glucocerebrosidase deficiency), Niemann-Pick (sphingomyelinase deficiency), Tay-Sachs (hexosaminidase A deficiency), Pompe's (acid maltase/alpha-glucosidase deficiency). All cause accumulation of undegraded substrates
Cytoskeleton
Three filament systems maintain cell shape, enable movement, and organize intracellular traffic:
| Filament | Diameter | Protein | Functions |
|---|---|---|---|
| Microfilaments | ~7 nm | Actin | Cell shape, movement, cytokinesis, microvilli |
| Intermediate filaments | ~10 nm | Vimentin, keratin, desmin, neurofilaments | Structural integrity, nuclear lamina |
| Microtubules | ~25 nm | Tubulin (α, β dimers) | Mitotic spindle, intracellular transport (kinesin/dynein motors), cilia/flagella |
Clinical: Colchicine inhibits microtubule polymerization - used in gout; taxanes stabilize microtubules - used as chemotherapy (prevents mitotic spindle breakdown). Chediak-Higashi syndrome involves defects in microtubule-based vesicle trafficking; Kartagener syndrome involves dynein arm defects causing immotile cilia.
3. The Cell Membrane
Structure: Fluid Mosaic Model
The plasma membrane is a phospholipid bilayer (~7.5 nm thick) in which protein molecules are embedded. Key properties:
- The lipid bilayer is not miscible with extra- or intracellular fluid - it is a hydrophobic barrier to water-soluble substances
- Lipid-soluble substances (O₂, CO₂, steroid hormones, fatty acids, ethanol) cross by simple diffusion directly through the bilayer
- The bilayer is not static - lipids diffuse laterally (flip-flop between leaflets is rare and requires flippases)
- Cholesterol intercalates between phospholipids, regulating fluidity: prevents crystallization at low temperatures and prevents excess fluidity at high temperatures. It also organizes lipid rafts - microdomains enriched in cholesterol and sphingolipids that concentrate signaling proteins
Membrane Proteins
- Integral (intrinsic) proteins: span the bilayer (transmembrane proteins); include ion channels, carrier proteins, receptors, enzymes
- Peripheral (extrinsic) proteins: attached to the cytoplasmic face by electrostatic interactions; include cytoskeletal anchors
- Channel proteins: aqueous pores allowing selective passage of water (aquaporins) or ions. They do NOT use energy
- Carrier proteins (transporters): bind the substrate, change conformation, and release it on the other side. Can be passive (facilitated diffusion) or active
4. Membrane Transport
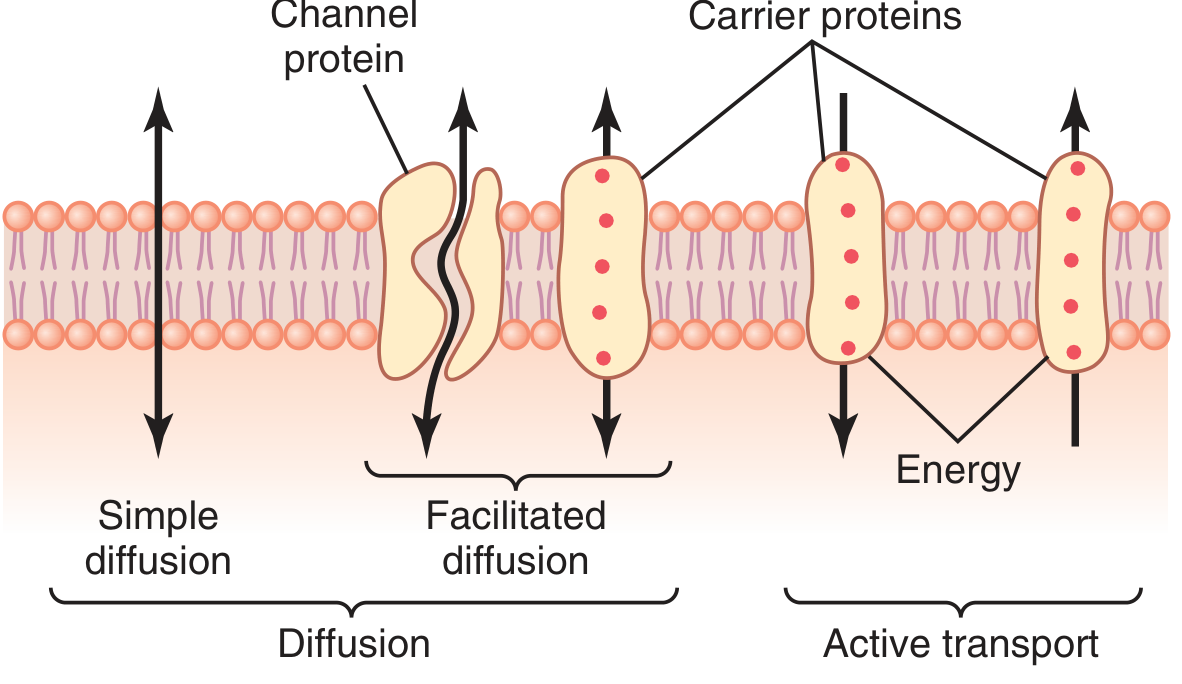
A. Passive Transport (No Energy Required)
1. Simple Diffusion
- Movement of molecules down their concentration gradient (from high to low)
- Net flux is proportional to the concentration difference and the membrane's permeability to that molecule
- Fick's law of diffusion: Flux = P × A × ΔC (where P = permeability coefficient, A = area, ΔC = concentration gradient)
- Applies to: O₂, CO₂, N₂, steroid hormones, fatty acids, very small uncharged polar molecules (water crosses slowly this way)
2. Facilitated Diffusion
- Down the concentration gradient, but via a protein carrier or channel
- Saturable (Michaelis-Menten kinetics), inhibitable by structural analogs
- Examples: GLUT1 (erythrocyte glucose transporter), GLUT2 (liver/pancreatic beta-cell), GLUT4 (insulin-regulated, in muscle and fat)
- Clinical: GLUT1 deficiency syndrome (De Vivo disease) - seizures, developmental delay; treated with ketogenic diet
3. Osmosis
- Movement of water across a semipermeable membrane from low-solute to high-solute concentration
- Osmolarity of body fluids = ~300 mOsm/L (plasma ~1 mOsm/L higher than interstitial fluid due to plasma proteins)
- Effective osmolarity (tonicity) is what determines cell volume changes:
- Isotonic (0.9% NaCl) - no cell volume change
- Hypotonic - cells swell (may lyse = hemolysis)
- Hypertonic - cells shrink (crenation)
- Clinical: Hyponatremia causes cerebral edema (cells swell); severe hyponatremia (Na⁺ <120 mEq/L) causes seizures and herniation. Rapid correction risks osmotic demyelination syndrome (central pontine myelinolysis)
B. Active Transport (Energy Required)
Primary Active Transport - directly uses ATP:
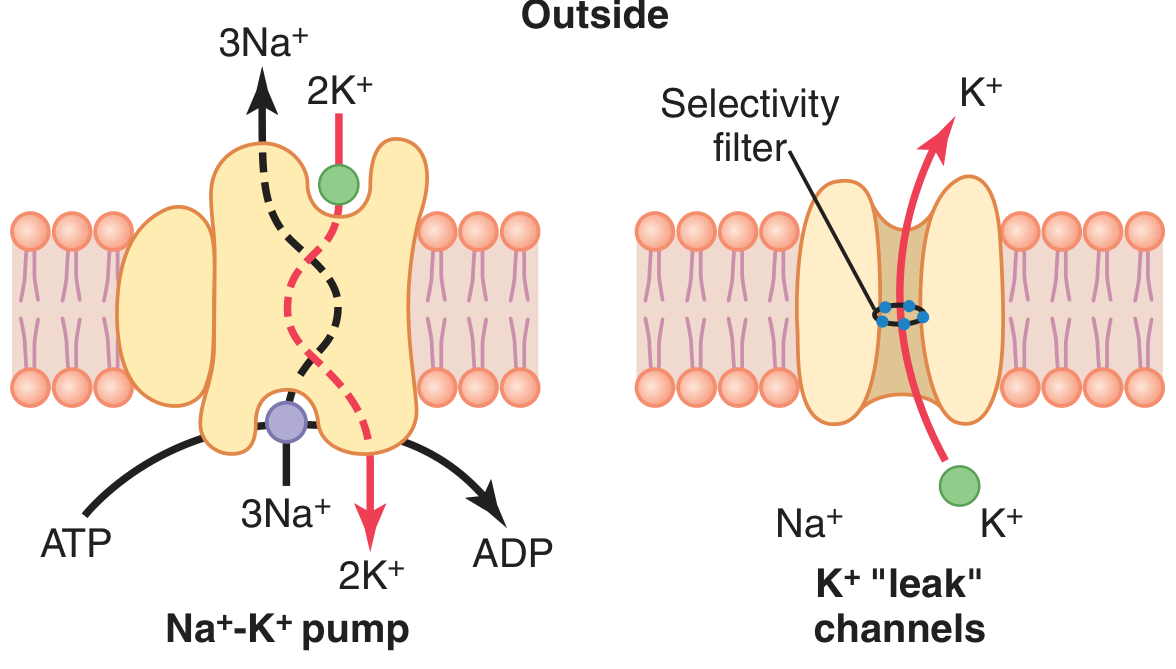
- Na⁺-K⁺-ATPase (Sodium-Potassium Pump): the most important pump in animal cells
- Pumps 3 Na⁺ OUT and 2 K⁺ IN per ATP hydrolyzed
- Creates and maintains: Na⁺ outside = 142 mEq/L, Na⁺ inside = 14 mEq/L; K⁺ inside = 140 mEq/L, K⁺ outside = 4 mEq/L
- Is electrogenic (net loss of 1 positive charge per cycle) - directly contributes ~-3 mV to the resting membrane potential
- Essential for: maintaining cell volume, resting membrane potential, and as the energy source for secondary active transport
- Clinical: Digoxin inhibits Na⁺-K⁺-ATPase → increases intracellular Na⁺ → reduces Na⁺/Ca²⁺ exchanger activity → increases intracellular Ca²⁺ → positive inotropy. Hyperkalemia inhibits the pump. Ouabain is a classic Na⁺-K⁺-ATPase inhibitor used in research
- Ca²⁺-ATPase (PMCA, SERCA): pump Ca²⁺ out of cytoplasm
- H⁺-K⁺-ATPase: in gastric parietal cells - target of proton pump inhibitors (omeprazole, pantoprazole)
Secondary Active Transport - uses the Na⁺ gradient created by the Na⁺-K⁺ pump (indirect use of ATP):
- Cotransport (symport): Na⁺ moves with the solute in the same direction. Example: SGLT1/2 (Na⁺-glucose co-transport in the gut and kidney)
- Clinical: SGLT2 inhibitors (gliflozins - empagliflozin, dapagliflozin) block glucose reabsorption in proximal tubule; used in T2DM, heart failure, and CKD
- Countertransport (antiport): Na⁺ moves in as another ion moves out. Example: Na⁺/Ca²⁺ exchanger (NCX), Na⁺/H⁺ exchanger (NHE)
- Clinical: NHE1 inhibition is a target for cardioprotection in ischemia-reperfusion
Vesicular Transport:
- Endocytosis: receptor-mediated (clathrin-coated pits, e.g., LDL receptor), phagocytosis, pinocytosis, caveolae-mediated
- Exocytosis: secretory vesicles fuse with plasma membrane; regulated by Ca²⁺ (neurotransmitter release, insulin secretion)
- Clinical: Familial hypercholesterolemia - defective LDL receptor leads to impaired receptor-mediated endocytosis of LDL → markedly elevated LDL-C and premature atherosclerosis
5. Resting Membrane Potential
The resting membrane potential (Vm) of most excitable cells is -70 to -80 mV (interior negative). This is established by:
Step 1 - Ion gradients created by the Na⁺-K⁺ pump:
- High K⁺ inside / low K⁺ outside
- Low Na⁺ inside / high Na⁺ outside
- Negative organic anions (proteins, phosphates) trapped inside
Step 2 - Selective permeability at rest:
- Resting membrane is far more permeable to K⁺ and Cl⁻ than to Na⁺ or Ca²⁺
- K⁺ leaks out through K⁺ "leak" channels (tandem-pore domain channels) down its concentration gradient, leaving negative charges behind → interior becomes negative
- The K⁺ equilibrium potential (EK) = -94 mV (Nernst equation with 35:1 K⁺ inside/outside ratio)
- Na⁺ has a small opposing inward leak, so Vm (-70 mV) is slightly less negative than pure EK
Nernst Equation (equilibrium potential for any ion):
E = (RT/zF) × ln([ion]outside / [ion]inside) At 37°C: E = (61.5/z) × log([ion]o / [ion]i)
Goldman-Hodgkin-Katz (GHK) equation: accounts for multiple ions by weighting each by its permeability - predicts Vm ≈ -70 mV given the relative permeabilities PK >> PCl >> PNa >> PCa
Chord Conductance Equation:
Em = (gK/gT)·EK + (gNa/gT)·ENa + (gCl/gT)·ECl + (gCa/gT)·ECa
At rest, gK and gCl dominate, pulling Vm toward their equilibrium potentials.
Role of Na⁺-K⁺ ATPase:
- Direct (small): electrogenic contribution (-3 mV) from 3Na out / 2K in
- Indirect (major): maintains the K⁺ concentration gradient that drives the K⁺ diffusion potential
6. Action Potentials
Action potentials are all-or-none electrical signals used by nerve and muscle to transmit information. They are generated by voltage-gated ion channels.
Properties
- Stereotypical size and shape - same amplitude each time for a given cell type
- All-or-none: either reaches threshold and fires fully, or does not fire at all
- Propagation: nondecremental - the amplitude does not decrease along the axon
- Threshold: typically ~-55 mV (about 15 mV depolarization from rest)
Phases of a Nerve Action Potential (Hodgkin-Huxley model)
| Phase | Event | Ion Movement |
|---|---|---|
| Resting | Vm = -70 mV | K⁺ leak channels open; Na⁺ channels closed |
| Depolarization / Upstroke | Voltage-gated Na⁺ channels open rapidly; inward Na⁺ current > outward K⁺ current | Na⁺ flows IN rapidly |
| Overshoot | Vm reaches ~+30 mV; approaches ENa (+65 mV) | Na⁺ channels begin to inactivate |
| Repolarization | Voltage-gated K⁺ channels open (delayed); Na⁺ channels inactivate | K⁺ flows OUT |
| Undershoot (afterhyperpolarization) | K⁺ channels still open; Vm transiently more negative than rest (approaches EK = -94 mV) | K⁺ still flowing OUT |
| Return to rest | K⁺ channels close; Na⁺ channels recover from inactivation | Na⁺-K⁺ pump restores gradients |
Refractory Periods
- Absolute refractory period (ARP): During depolarization and early repolarization; Na⁺ channels are in the inactivated state and cannot re-open regardless of stimulus strength. Prevents re-excitation and ensures unidirectional propagation
- Relative refractory period (RRP): After ARP; some Na⁺ channels have recovered but membrane is hyperpolarized; a suprathreshold stimulus can elicit an action potential but it will be smaller
Propagation and Conduction Velocity
- At each point, the local current from an active segment depolarizes adjacent membrane to threshold
- Myelinated axons: saltatory conduction - action potential "jumps" from node of Ranvier to node; much faster
- Factors increasing conduction velocity: myelination (most important), larger axon diameter, higher temperature
- Clinical: Multiple sclerosis - demyelination slows or blocks conduction velocity. Sodium channel blocker local anesthetics (lidocaine, bupivacaine) - block the inactivated state of Na⁺ channels; preferentially affect rapidly firing pain fibers
7. Cell Signaling and Signal Transduction
Every cell receives and processes information from its environment. External signals include hormones, neurotransmitters, growth factors, metabolites, ions, light, and mechanical stimuli.
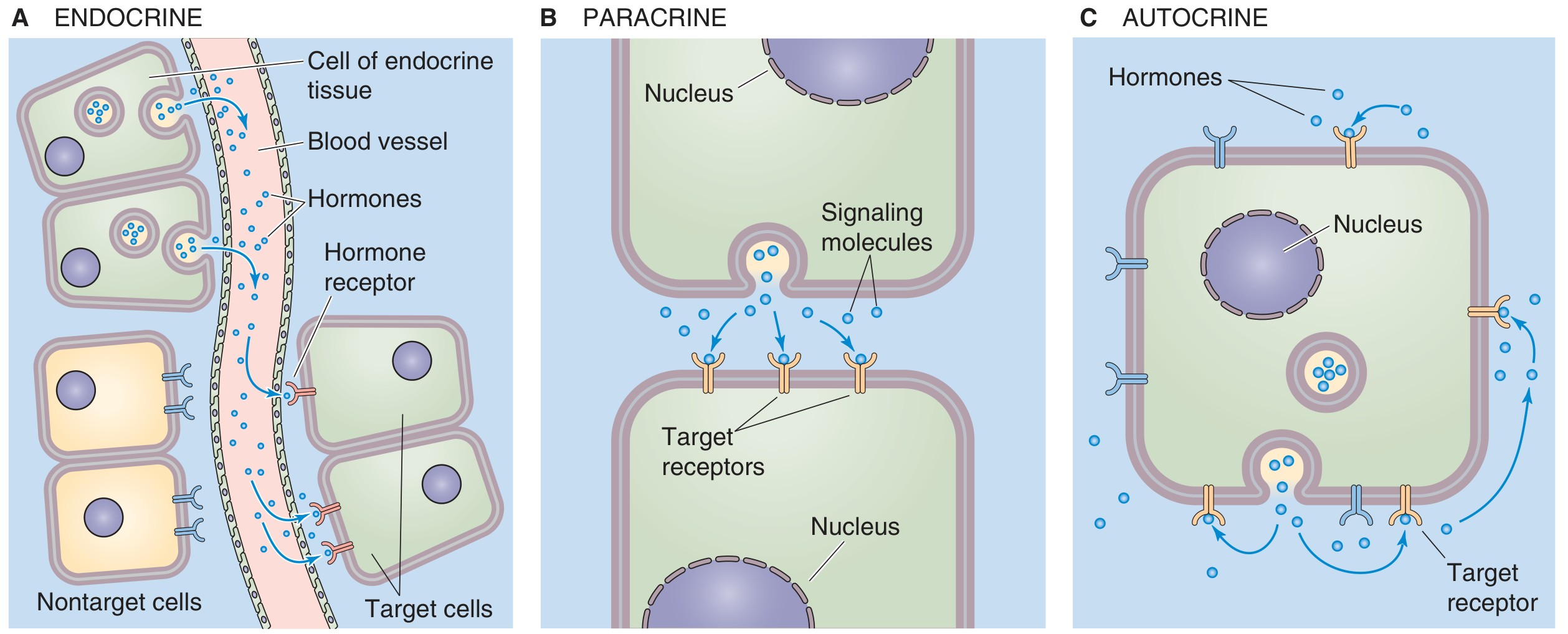
Modes of Cell-to-Cell Communication
| Mode | Mechanism | Example |
|---|---|---|
| Endocrine | Signal enters blood; acts on distant cells | Insulin from pancreatic β-cells acts on muscle/fat |
| Paracrine | Signal acts on neighboring cells in same tissue | ACh at neuromuscular junction |
| Autocrine | Signal acts on the same cell that secreted it | Growth factors in cancer |
| Juxtacrine | Physical cell-cell or cell-matrix contact | Notch-Delta signaling in development |
Types of Receptors
1. Ligand-gated ion channels (ionotropic receptors)
- Receptor IS the channel - binding opens the channel directly
- Fastest response (milliseconds)
- Examples: nicotinic ACh receptor (opens Na⁺/K⁺ channel), GABA-A receptor (opens Cl⁻ channel), NMDA/AMPA glutamate receptors
- Clinical: Benzodiazepines potentiate GABA-A (increase frequency of Cl⁻ channel opening); barbiturates increase duration; used as anxiolytics and for seizures. Myasthenia gravis - autoantibodies against nicotinic ACh receptors at NMJ
2. G protein-coupled receptors (GPCRs)
- Largest family of cell-surface receptors (~800 in humans); 7 transmembrane domains (serpentine receptors)
- Coupled to heterotrimeric G proteins (Gα, Gβ, Gγ)
- Ligand binding → G protein activation (GDP → GTP exchange on Gα) → Gα and Gβγ dissociate and activate effectors
- Major subtypes:
| G protein | Effect | Example |
|---|---|---|
| Gs | Activates adenylyl cyclase → ↑cAMP → PKA activation | β-adrenergic receptor, glucagon receptor |
| Gi | Inhibits adenylyl cyclase → ↓cAMP | α2-adrenergic, muscarinic M2 |
| Gq | Activates PLC-β → IP₃ + DAG → Ca²⁺ release + PKC activation | α1-adrenergic, muscarinic M1/M3, angiotensin II AT1 |
- cAMP activates protein kinase A (PKA) → phosphorylates downstream targets
- IP₃ triggers Ca²⁺ release from ER; DAG activates protein kinase C (PKC)
- Clinical: Cholera toxin ADP-ribosylates Gsα → constitutive activation → massive ↑cAMP in intestinal epithelium → Cl⁻ secretion and profuse watery diarrhea. Pertussis toxin ADP-ribosylates Giα → blocks inhibitory signaling. Many drugs target GPCRs: β-blockers, ACE inhibitors (indirectly), opioids (μ-receptor, Gi-coupled), statins' pleiotropic effects
3. Receptor Tyrosine Kinases (RTKs)
- Ligand binding → receptor dimerization → autophosphorylation of tyrosine residues → activation of downstream cascades (RAS-MAPK, PI3K-Akt, PLC-γ)
- Examples: insulin receptor (heterotetrameric, but same principle), EGF receptor, PDGF receptor, VEGF receptor
- RAS-MAPK pathway: growth, proliferation
- PI3K-Akt-mTOR pathway: survival, protein synthesis, metabolism
- Clinical: RAS mutations are found in ~30% of human cancers (KRAS in pancreatic cancer, colorectal cancer, lung adenocarcinoma) - constitutively active RTK downstream signaling. Imatinib (Gleevec) inhibits BCR-ABL tyrosine kinase in CML. Trastuzumab (Herceptin) targets HER2/neu RTK in breast cancer. Insulin resistance in Type 2 diabetes involves defective downstream insulin receptor signaling (IRS-1 and PI3K pathway)
4. Nuclear (Intracellular) Receptors
- For hydrophobic ligands that cross the membrane (steroid hormones, thyroid hormones, vitamin D, retinoids)
- Ligand binding → receptor dimerization → translocation to nucleus → binding to hormone response elements (HREs) in DNA → regulate gene transcription (hours-days)
- Clinical: Glucocorticoid receptors: cortisol/dexamethasone → anti-inflammatory gene expression; Androgen receptors: testosterone/DHT → prostate cancer; Thyroid hormone receptor mutations → resistance to thyroid hormone (Refetoff syndrome)
5. Gap Junctions
- Formed by connexins; allow direct passage of ions and small molecules (<1200 Da) including Ca²⁺ and cAMP between adjacent cells
- Regulated by intracellular Ca²⁺, pH, and Vm - elevated Ca²⁺ closes gap junctions (protective in ischemia)
- Clinical: Connexin 26 (GJB2) mutations are the most common cause of hereditary non-syndromic sensorineural hearing loss. Gap junctions are critical for cardiac electrical conduction
8. Cell Cycle and Proliferation
The cell cycle is the fundamental mechanism to maintain tissue homeostasis and enable reproduction of identical genetic information.
Phases
| Phase | Events |
|---|---|
| G1 (first gap) | Cell grows; receives pro/anti-proliferative signals; most important checkpoint |
| S (synthesis) | DNA replication; each chromosome is duplicated |
| G2 (second gap) | Cell verifies DNA replication; grows further; prepares for mitosis |
| M (mitosis) | Chromosomes condense, align, and separate; cytoplasm divides (cytokinesis) |
| G0 | Quiescent state; most post-mitotic cells (neurons, cardiac myocytes) |
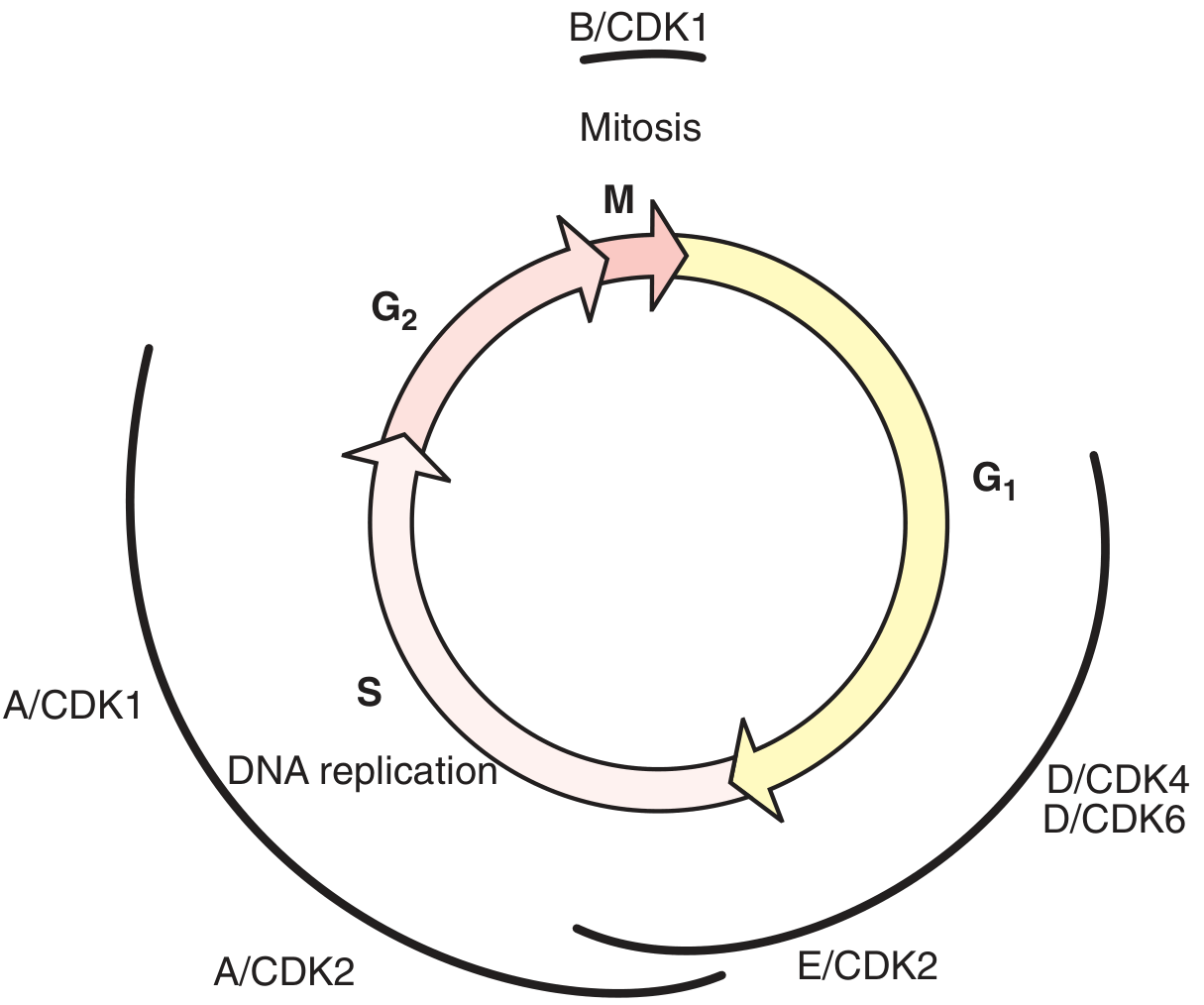
Cyclin-CDK Control
The "engine" of the cell cycle is cyclin-dependent kinases (CDKs). CDKs are constitutively expressed but inactive without their cyclin partners. Cyclin expression oscillates during the cycle:
| Complex | Phase controlled |
|---|---|
| Cyclin D / CDK4,6 | Early G1 |
| Cyclin E / CDK2 | Late G1 → S transition |
| Cyclin A / CDK2 | S phase |
| Cyclin A / CDK1 | G2 → M |
| Cyclin B / CDK1 | M phase (MPF) |
Key checkpoint: The G1 Restriction Point (R point)
- Cyclin D/CDK4,6 phosphorylate Retinoblastoma protein (pRb)
- Phospho-pRb releases E2F transcription factor → activates genes for S phase entry
- CDK inhibitors (CKIs) act as brakes: p21 (WAF1), p27 (KIP1), p16 (INK4a) inhibit CDK activity
- p53 (the "guardian of the genome") - activated by DNA damage → induces p21 → cell cycle arrest. If damage is irreparable → p53 triggers apoptosis. Clinical: p53 is mutated in >50% of human cancers (Li-Fraumeni syndrome = germline p53 mutation). CDK4/6 inhibitors (palbociclib, ribociclib, abemaciclib) are used in HR+/HER2- breast cancer
DNA Repair
- G1/S checkpoint: detects unreplicated DNA damage; p53-p21 axis
- Intra-S checkpoint: slows replication if damage detected
- G2/M checkpoint: ensures DNA is fully replicated before mitosis
- Repair mechanisms: nucleotide excision repair (NER), base excision repair (BER), mismatch repair (MMR), homologous recombination (HR), non-homologous end joining (NHEJ)
- Clinical: BRCA1/BRCA2 mutations impair HR → increased breast/ovarian cancer risk. Lynch syndrome = defective MMR genes (MLH1, MSH2, MSH6) → hereditary colorectal cancer. Xeroderma pigmentosum = defective NER → extreme UV sensitivity and skin cancer
9. Apoptosis (Programmed Cell Death)
Apoptosis is the physiologic, caspase-dependent, controlled death of unwanted cells. Unlike necrosis, it maintains membrane integrity so the cell "dies with dignity" without spilling contents that would damage neighbors.
Comparison: Apoptosis vs. Necrosis
| Feature | Necrosis | Apoptosis |
|---|---|---|
| Cell swelling | Yes | No |
| Cell shrinkage | No | Yes |
| Plasma membrane damage | Yes | No |
| Membrane blebbing | No | Yes |
| Chromatin aggregation | No | Yes |
| DNA fragmentation | Random | Oligonucleosomal (ladder pattern) |
| Cytochrome c release from mitochondria | No | Yes |
| Caspase activation | No | Yes |
| Inflammation | Yes (contents released) | No |
Pathways
Intrinsic (Mitochondrial) Pathway
- Triggered by internal stress: DNA damage, hypoxia, ER stress, growth factor withdrawal
- Pro-apoptotic Bcl-2 family proteins (Bax, Bak, Bad, Bid) permeabilize the outer mitochondrial membrane
- Cytochrome c leaks into cytosol → forms the apoptosome with Apaf-1 and procaspase-9 → activates caspase-9 → activates executioner caspases (caspase-3, -6, -7)
- Anti-apoptotic proteins Bcl-2 and Bcl-xL block this by preventing cytochrome c release
- Clinical: Chronic lymphocytic leukemia (CLL) and follicular lymphoma overexpress Bcl-2 (t(14;18) translocation in follicular lymphoma). Venetoclax is a BH3-mimetic that inhibits Bcl-2, restoring apoptosis in CLL
Extrinsic (Death Receptor) Pathway
- Triggered by external death signals: FasL binding Fas (CD95), TRAIL binding DR4/DR5, TNF binding TNFR1
- Receptor activation → DISC (death-inducing signaling complex) formation → caspase-8 activation → executioner caspases
- Clinical: The extrinsic pathway is exploited by cytotoxic T lymphocytes (CTLs) via FasL-Fas interaction and perforin/granzyme mechanisms to kill virus-infected or cancer cells. Autoimmune lymphoproliferative syndrome (ALPS) = defective Fas-mediated apoptosis → lymphoproliferation
Morphological Features of Apoptosis
- DNA fragmentation by Ca²⁺/Mg²⁺-dependent endonucleases → oligonucleosomal "ladder" on gel electrophoresis
- Cell volume decreases; cytoskeletal reorganization
- Membrane blebbing
- Chromatin condensation and nuclear fragmentation
- Cell breaks into membrane-bound apoptotic bodies that are phagocytosed by macrophages or neighboring cells
10. Cellular Homeostasis: Integrated Clinical Correlations
Ischemia-Reperfusion Injury
During ischemia: ATP depletion → Na⁺-K⁺-ATPase fails → intracellular Na⁺ rises → Na⁺/Ca²⁺ exchanger reverses → intracellular Ca²⁺ overload → mitochondrial dysfunction, calpain activation, phospholipase A₂ activation → cell death. On reperfusion: sudden burst of reactive oxygen species (ROS) amplifies the injury and opens the mitochondrial permeability transition pore (mPTP) → apoptosis/necrosis
Ion Channel Channelopathies
| Disease | Channel | Mechanism |
|---|---|---|
| Long QT syndrome | HERG K⁺ channel (LQT2), Na⁺ channel SCN5A (LQT3) | Prolonged repolarization → torsades de pointes |
| Cystic fibrosis | CFTR Cl⁻ channel | Loss of Cl⁻ secretion → thick mucus in lung, gut, pancreas |
| Hypokalemic periodic paralysis | L-type Ca²⁺ channel (Cav1.1) | Muscle inexcitability during hypokalemia |
| Myotonia congenita | ClC-1 Cl⁻ channel | Impaired repolarization in skeletal muscle |
Cellular Edema vs. Vasogenic Edema
- Cytotoxic edema: failure of Na⁺-K⁺-ATPase (ischemia, hypoxia) → intracellular Na⁺ accumulation → osmotic water entry → cell swells; BBB is intact
- Vasogenic edema: BBB disruption → protein-rich fluid leaks into brain interstitium; Na⁺-K⁺-ATPase still functional
Pharmacological Targets Rooted in Cell Physiology
| Drug | Target | Mechanism |
|---|---|---|
| Digoxin | Na⁺-K⁺-ATPase | Inhibition → ↑intracellular Ca²⁺ → positive inotropy |
| Furosemide | Na⁺-K⁺-2Cl⁻ cotransporter (NKCC2) | Blocks secondary active transport in thick ascending limb |
| Omeprazole/PPIs | H⁺-K⁺-ATPase | Irreversibly inhibit gastric proton pump |
| SGLT2 inhibitors | Na⁺-glucose cotransporter | Block renal glucose reabsorption |
| Local anesthetics | Voltage-gated Na⁺ channels | Block Na⁺ influx → prevent action potential generation |
| Colchicine | Microtubule polymerization | Inhibits neutrophil migration; treats gout and pericarditis |
| Vincristine/Taxanes | Microtubules | Arrest mitotic spindle formation/breakdown → halt M phase |
| CDK4/6 inhibitors | Cyclin D-CDK4/6 | Prevent pRb phosphorylation → block G1-S transition |
| Venetoclax | Bcl-2 | BH3-mimetic → restores apoptosis in Bcl-2-overexpressing tumors |
Summary: The Cell in One Framework
STRUCTURE → FUNCTION → PHYSIOLOGY → PATHOLOGY → PHARMACOLOGY
Lipid bilayer → Barrier/permeability → Selective ion gradients → Channelopathies → Na⁺ channel blockers
Na⁺-K⁺-ATPase → Ion gradient engine → Resting membrane Vm → Ischemic injury → Digoxin, ouabain
Voltage-gated → Action potential → Neural/muscle signals → LQT, epilepsy → Lidocaine, anticonvulsants
ion channels
GPCRs / RTKs → Signal transduction → Hormone responses → Cancer, diabetes → β-blockers, imatinib
Cyclin-CDKs → Cell cycle → Proliferation control → Cancer → Palbociclib
Caspases / Bcl-2 → Apoptosis → Tissue homeostasis → Lymphoma, CLL → Venetoclax
Lysosomes → Macromolecule digestion→ Cellular recycling → Storage diseases → ERT (Gaucher, Pompe)
Sources:
- Medical Physiology (Boron & Boulpaep), Chapters 2-3 - Organelles, Signal Transduction
- Guyton and Hall Textbook of Medical Physiology, Chapters 4-5 - Membrane Transport, Resting Membrane Potential
- Costanzo Physiology 7th Edition, Chapter 1 - Resting Potential, Action Potentials
- Schwartz's Principles of Surgery 11th Ed., Chapter 15 - Cell Cycle, Apoptosis, Signal Transduction
- Histology: A Text and Atlas (Ross & Pawlina) - Apoptosis morphology
This is a shared conversation. Sign in to Orris to start your own chat.