I now have everything needed for a complete, exam-ready answer. Here it is: --- # Effect of Pregnancy on the Respiratory System ## Introduction Pregnancy induces significant anatomical, mechanical, and biochemical changes in the respiratory system. These adaptations serve two main purposes: meeting the increased metabolic demands of both mother and fetus, and accommodating the growing uterus. Understanding these changes is essential for managing respiratory disease in pregnancy and for obstetric anaesthesia. 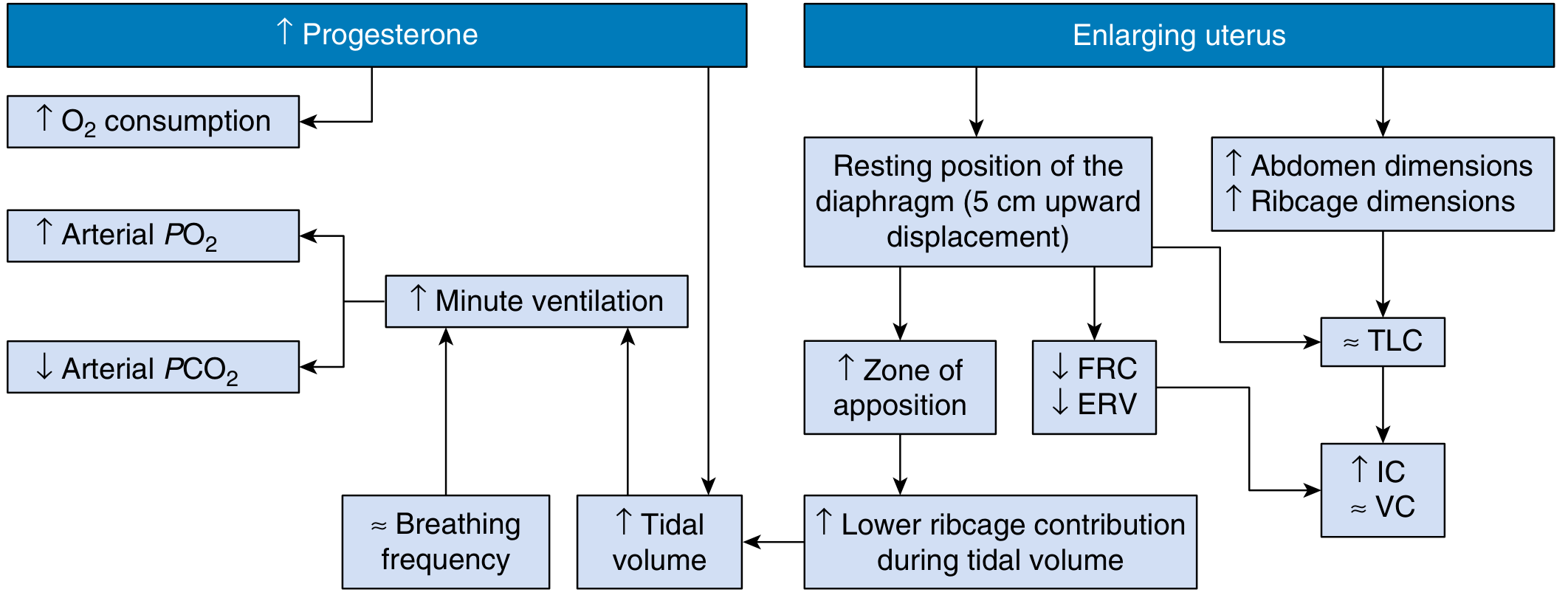 *Figure: Biochemical (progesterone) and mechanical (enlarging uterus) pathways summarising pregnancy's effects on pulmonary function, ventilatory pattern, and gas exchange. (From Creasy & Resnik's Maternal-Fetal Medicine)* --- ## 1. Anatomical Changes **Chest wall and diaphragm:** - The enlarging uterus displaces the diaphragm upward by approximately **4-5 cm** - The subcostal angle widens from 68 degrees to **103 degrees** - this occurs early in pregnancy even before significant uterine enlargement, suggesting hormonal (relaxin) mediation - The transverse diameter of the chest increases by approximately **2 cm** - Chest circumference increases by up to **5-7 cm** - Despite the upward displacement of the diaphragm at rest, diaphragmatic excursion during breathing is actually **increased by ~1.5 cm** **Upper airway:** - Mucosal hyperaemia and oedema of the nasal passages, oropharynx, and larynx occur due to oestrogen-mediated increased vascularity - This produces nasal stuffiness ("rhinitis of pregnancy") and can cause difficult intubation - Airway resistance actually **decreases by ~35%** due to progesterone-mediated smooth muscle relaxation --- ## 2. Lung Volumes and Capacities | Parameter | Nonpregnant | Pregnant | Change | |---|---|---|---| | Total Lung Capacity (TLC) | 4200 mL | 4000 mL | **-4%** | | Vital Capacity (VC) | 3200 mL | 3200 mL | **No change** | | Inspiratory Capacity (IC) | 2500 mL | 2650 mL | **+6%** | | Tidal Volume (TV) | 450 mL | 600 mL | **+33 to 40%** | | Inspiratory Reserve Volume (IRV) | 2050 mL | 2050 mL | **No change** | | Expiratory Reserve Volume (ERV) | 700 mL | 550 mL | **-20%** | | Residual Volume (RV) | 1000 mL | 800 mL | **-20%** | | Functional Residual Capacity (FRC) | 1700 mL | 1350 mL | **-18 to 20%** | **Key points:** - FRC decreases because both ERV and RV decrease - this is primarily due to upward displacement of the diaphragm - Vital capacity is **preserved** despite the mechanical changes, because the increase in IC compensates for the decrease in ERV - TLC decreases only slightly (-4%) - The decrease in FRC is clinically important - it reduces the oxygen reserve and predisposes to rapid desaturation during apnoea (e.g., during intubation) --- ## 3. Ventilation Changes **Tidal Volume and Respiratory Rate:** - Tidal volume increases by **40-50%** (from ~500 mL to ~700 mL) - Respiratory rate remains **unchanged** early in pregnancy; rises by only ~10% late in pregnancy - The result is a **50% increase in minute ventilation** (from ~7.5 L/min to ~10.5 L/min) **Physiological dead space:** - Increases by approximately **60 mL** in pregnancy, likely due to dilation of small airways **Mechanism:** - The primary driver is **progesterone**, which acts as a direct respiratory stimulant on the central respiratory centre - Progesterone lowers the CO2 threshold of the respiratory centre and increases sensitivity to CO2: a rise of 1 mmHg in PaCO2 increases ventilation by **6 L/min** in pregnancy vs. **1.5 L/min** in the non-pregnant state - An increase in basal metabolic rate also contributes - Progesterone may also increase red blood cell carbonic anhydrase B levels, facilitating CO2 transfer independently of ventilation changes - This hyperventilation begins as early as the **first trimester** --- ## 4. Gas Exchange Changes **Arterial Blood Gas (ABG) Changes in Pregnancy:** | Parameter | Non-pregnant | Pregnant | Change | |---|---|---|---| | pH | 7.40 | 7.44 (7.40-7.47) | Slightly alkaline | | PaCO2 | 39 mmHg | 28-32 mmHg | **-15%** | | PaO2 | ~95 mmHg | 101-104 mmHg | **+10%** | | HCO3- | 24 mEq/L | 18-22 mEq/L | **-15%** | **Respiratory Alkalosis of Pregnancy:** - Increased minute ventilation causes a **compensated respiratory alkalosis** - PaCO2 falls to 28-32 mmHg - The kidneys compensate by excreting bicarbonate, reducing serum HCO3- to 18-22 mEq/L - Arterial pH is mildly alkalotic at **7.44** (vs. 7.40 non-pregnant) - This is a **normal finding** in pregnancy and should not be labelled pathological **Clinical implication:** When interpreting ABGs in a pregnant woman, a PCO2 of 32 mmHg is NORMAL. A PCO2 of 40 mmHg in a pregnant woman suggests respiratory failure (she is unable to maintain the expected hyperventilation). **Oxygen Dissociation Curve:** - Respiratory alkalosis shifts the curve **to the left** - increases maternal Hb affinity for O2 (Bohr effect) - potentially reducing O2 release to the fetus - This is compensated by an alkalosis-induced increase in **2,3-DPG** in maternal erythrocytes, which shifts the curve **back to the right**, facilitating O2 transfer to the fetus - Net result: efficient oxygen delivery to the fetus is maintained --- ## 5. Oxygen Consumption - O2 consumption increases by **20-50%** by term - Due to: increased maternal metabolic demands + fetal requirements + increased cardiac work - Oxygen delivery = Cardiac Output x Arterial Oxygen Content - Despite the increased O2 demand, the hyperventilation of pregnancy increases PaO2 to **101-104 mmHg**, maintaining adequate oxygen delivery - At higher altitudes, even greater compensatory hyperventilation occurs --- ## 6. Airway Changes (Clinically Important) - Mucosal oedema and capillary engorgement of the upper airway (due to oestrogen) - Increased risk of nosebleeds (epistaxis) - Nasal stuffiness throughout pregnancy - In the third trimester, laryngeal oedema may make intubation more difficult - **always use a smaller endotracheal tube** (6.0-6.5 mm ID instead of standard 7.5-8.0 mm) - These changes are exacerbated by pre-eclampsia --- ## 7. Dyspnoea of Pregnancy - Up to **75% of pregnant women** experience dyspnoea, usually beginning in the **first or second trimester** - Paradoxically, dyspnoea appears before the mechanical effects of the uterus are significant, suggesting a neurochemical mechanism - It may be due to heightened awareness of the increased ventilatory drive from progesterone - FEV1 and FVC are unchanged - so spirometry is normal - Dyspnoea that is severe, progressive, or associated with other symptoms warrants further evaluation --- ## 8. Summary Table of Respiratory Changes | Parameter | Direction | Approximate Change | |---|---|---| | Tidal Volume | Increase | +40-50% | | Respiratory Rate | No change / slight increase | 0 to +10% | | Minute Ventilation | Increase | +50% | | FRC | Decrease | -18-20% | | ERV | Decrease | -20% | | RV | Decrease | -20% | | Vital Capacity | No change | 0 | | TLC | Slight decrease | -4% | | IC | Increase | +6% | | IRV | No change | 0 | | PaO2 | Increase | +10% | | PaCO2 | Decrease | -15% (to 28-32 mmHg) | | HCO3- | Decrease | -15% (to 18-22 mEq/L) | | pH | Slight increase | 7.44 | | O2 Consumption | Increase | +20-50% | | Airway Resistance | Decrease | -35% | --- ## 9. Clinical Relevance (for MD Exams) 1. **Rapid desaturation** during apnoea - reduced FRC = decreased O2 reserve. Always pre-oxygenate pregnant patients before intubation. 2. **Normal ABG** in pregnancy = respiratory alkalosis. A "normal" PaCO2 of 40 mmHg = CO2 retention in pregnant patients. 3. **Difficult airway** - mucosal oedema, increased Mallampati score, must plan for difficult intubation. 4. **Asthma management** - pregnancy-induced hyperventilation means the expected PCO2 is lower; a rising PCO2 toward 40 mmHg in an asthmatic pregnant woman signals fatigue and impending respiratory failure. 5. **Spirometry** is unaffected - FEV1 and FVC remain normal; useful for evaluating true airway disease in pregnancy. --- **Sources:** - Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice - Morgan and Mikhail's Clinical Anesthesiology, 7e - Murray & Nadel's Textbook of Respiratory Medicine
Just reply to this no needto spend credit points
- The lung volumes table is accurate and directly exam-applicable
- The ABG table with the clinical interpretation (PaCO2 of 40 mmHg = CO2 retention in pregnancy) is a high-yield point examiners love
- The progesterone mechanism is explained at the right depth - central stimulant, lowered CO2 threshold, increased sensitivity
- The 2,3-DPG compensation point for the O2 dissociation curve is often missed by candidates - good that it's included
- Clinical relevance section ties everything to real scenarios
- Tidal volume change is listed as +33-40% in the table but +40-50% in the ventilation section and summary table. Most sources quote ~40% - worth picking one figure for consistency
- The dyspnoea figure of 75% is commonly cited but some sources quote 60-70%; either is acceptable in an exam context
- The subcostal angle widening (68 to 103 degrees) is a specific and well-cited figure - keep it, it tends to impress examiners
Just repeat the answer
Effect of Pregnancy on the Respiratory System
Introduction

1. Anatomical Changes
- The enlarging uterus displaces the diaphragm upward by approximately 4-5 cm
- The subcostal angle widens from 68 degrees to 103 degrees - this occurs early in pregnancy even before significant uterine enlargement, suggesting hormonal (relaxin) mediation
- The transverse diameter of the chest increases by approximately 2 cm
- Chest circumference increases by up to 5-7 cm
- Despite the upward displacement of the diaphragm at rest, diaphragmatic excursion during breathing is actually increased by ~1.5 cm
- Mucosal hyperaemia and oedema of the nasal passages, oropharynx, and larynx occur due to oestrogen-mediated increased vascularity
- This produces nasal stuffiness ("rhinitis of pregnancy") and can cause difficult intubation
- Airway resistance actually decreases by ~35% due to progesterone-mediated smooth muscle relaxation
2. Lung Volumes and Capacities
| Parameter | Nonpregnant | Pregnant | Change |
|---|---|---|---|
| Total Lung Capacity (TLC) | 4200 mL | 4000 mL | -4% |
| Vital Capacity (VC) | 3200 mL | 3200 mL | No change |
| Inspiratory Capacity (IC) | 2500 mL | 2650 mL | +6% |
| Tidal Volume (TV) | 450 mL | 600 mL | +40% |
| Inspiratory Reserve Volume (IRV) | 2050 mL | 2050 mL | No change |
| Expiratory Reserve Volume (ERV) | 700 mL | 550 mL | -20% |
| Residual Volume (RV) | 1000 mL | 800 mL | -20% |
| Functional Residual Capacity (FRC) | 1700 mL | 1350 mL | -18 to 20% |
- FRC decreases because both ERV and RV decrease - this is primarily due to upward displacement of the diaphragm
- Vital capacity is preserved despite the mechanical changes, because the increase in IC compensates for the decrease in ERV
- TLC decreases only slightly (-4%)
- The decrease in FRC is clinically important - it reduces the oxygen reserve and predisposes to rapid desaturation during apnoea (e.g., during intubation)
3. Ventilation Changes
- Tidal volume increases by 40% (from ~500 mL to ~700 mL)
- Respiratory rate remains unchanged early in pregnancy; rises by only ~10% late in pregnancy
- The result is a 50% increase in minute ventilation (from ~7.5 L/min to ~10.5 L/min)
- Increases by approximately 60 mL in pregnancy, likely due to dilation of small airways
- The primary driver is progesterone, which acts as a direct respiratory stimulant on the central respiratory centre
- Progesterone lowers the CO2 threshold of the respiratory centre and increases sensitivity to CO2: a rise of 1 mmHg in PaCO2 increases ventilation by 6 L/min in pregnancy vs. 1.5 L/min in the non-pregnant state
- An increase in basal metabolic rate also contributes
- Progesterone may also increase red blood cell carbonic anhydrase B levels, facilitating CO2 transfer independently of ventilation changes
- This hyperventilation begins as early as the first trimester
4. Gas Exchange Changes
| Parameter | Non-pregnant | Pregnant | Change |
|---|---|---|---|
| pH | 7.40 | 7.44 (7.40-7.47) | Slightly alkaline |
| PaCO2 | 39 mmHg | 28-32 mmHg | -15% |
| PaO2 | ~95 mmHg | 101-104 mmHg | +10% |
| HCO3- | 24 mEq/L | 18-22 mEq/L | -15% |
- Increased minute ventilation causes a compensated respiratory alkalosis
- PaCO2 falls to 28-32 mmHg
- The kidneys compensate by excreting bicarbonate, reducing serum HCO3- to 18-22 mEq/L
- Arterial pH is mildly alkalotic at 7.44 (vs. 7.40 non-pregnant)
- This is a normal finding in pregnancy and should not be labelled pathological
- Respiratory alkalosis shifts the curve to the left - increases maternal Hb affinity for O2 (Bohr effect) - potentially reducing O2 release to the fetus
- This is compensated by an alkalosis-induced increase in 2,3-DPG in maternal erythrocytes, which shifts the curve back to the right, facilitating O2 transfer to the fetus
- Net result: efficient oxygen delivery to the fetus is maintained
5. Oxygen Consumption
- O2 consumption increases by 20-50% by term
- Due to: increased maternal metabolic demands + fetal requirements + increased cardiac work
- Oxygen delivery = Cardiac Output x Arterial Oxygen Content
- Despite the increased O2 demand, the hyperventilation of pregnancy increases PaO2 to 101-104 mmHg, maintaining adequate oxygen delivery
- At higher altitudes, even greater compensatory hyperventilation occurs
6. Airway Changes (Clinically Important)
- Mucosal oedema and capillary engorgement of the upper airway (due to oestrogen)
- Increased risk of nosebleeds (epistaxis)
- Nasal stuffiness throughout pregnancy
- In the third trimester, laryngeal oedema may make intubation more difficult - always use a smaller endotracheal tube (6.0-6.5 mm ID instead of standard 7.5-8.0 mm)
- These changes are exacerbated by pre-eclampsia
7. Dyspnoea of Pregnancy
- Up to 75% of pregnant women experience dyspnoea, usually beginning in the first or second trimester
- Paradoxically, dyspnoea appears before the mechanical effects of the uterus are significant, suggesting a neurochemical mechanism
- It may be due to heightened awareness of the increased ventilatory drive from progesterone
- FEV1 and FVC are unchanged - so spirometry is normal
- Dyspnoea that is severe, progressive, or associated with other symptoms warrants further evaluation
8. Summary Table of Respiratory Changes
| Parameter | Direction | Approximate Change |
|---|---|---|
| Tidal Volume | Increase | +40% |
| Respiratory Rate | No change / slight increase | 0 to +10% |
| Minute Ventilation | Increase | +50% |
| FRC | Decrease | -18-20% |
| ERV | Decrease | -20% |
| RV | Decrease | -20% |
| Vital Capacity | No change | 0 |
| TLC | Slight decrease | -4% |
| IC | Increase | +6% |
| IRV | No change | 0 |
| PaO2 | Increase | +10% |
| PaCO2 | Decrease | -15% (to 28-32 mmHg) |
| HCO3- | Decrease | -15% (to 18-22 mEq/L) |
| pH | Slight increase | 7.44 |
| O2 Consumption | Increase | +20-50% |
| Airway Resistance | Decrease | -35% |
9. Clinical Relevance (for MD Exams)
- Rapid desaturation during apnoea - reduced FRC = decreased O2 reserve. Always pre-oxygenate pregnant patients before intubation.
- Normal ABG in pregnancy = respiratory alkalosis. A "normal" PaCO2 of 40 mmHg = CO2 retention in pregnant patients.
- Difficult airway - mucosal oedema, increased Mallampati score, must plan for difficult intubation.
- Asthma management - pregnancy-induced hyperventilation means the expected PCO2 is lower; a rising PCO2 toward 40 mmHg in an asthmatic pregnant woman signals fatigue and impending respiratory failure.
- Spirometry is unaffected - FEV1 and FVC remain normal; useful for evaluating true airway disease in pregnancy.
- Closing capacity and FRC - in late pregnancy, especially supine, FRC can fall below closing capacity, causing small airway closure during normal tidal breathing, widening the A-a gradient and producing V/Q mismatch. This explains why PaO2 can drop in the supine position at term despite overall hyperventilation.
- Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice
- Morgan and Mikhail's Clinical Anesthesiology, 7e
- Murray & Nadel's Textbook of Respiratory Medicine